Ordered, immediately called back and the same day delivered the order.Very pleased with the work. Thank you for prompt and accurate work https://africarx.co.za/ great prices, delivered on the day of the order. Pleasant managers consult by phone.
Mw4042 bradley
Journal of Antimicrobial Chemotherapy (1999) 43, 261–266 The control of hyperendemic glycopeptide-resistant Enterococcus spp. on a haematology unit by changing antibiotic usage Susan J. Bradleya,b, Angela L. T. Wilsona, Michael C. Allenc, Hilary A. Shera, Anthony H. Goldstoneb and Geoffrey M. Scotta* aDepartments of Clinical Microbiology and bHaematology, University College London Hospitals, London, WC1E 6DB; cWyeth UK Ltd, Maidenhead, Berks, SL6 0PH, UKThe rectal carriage of glycopeptide-resistant Enterococcus spp. (GRE) had been established at approximately 50% in a series of prevalence studies on a busy haematological malignancy unit. The aim of this study was to reduce the chance of patients acquiring GRE. A prospective three- phase sequential study was performed. In Phase 1, the acquisition rate of GRE detectable by rectal swab was measured without any intervention for a period of 4 months. For the following 8 months (Phase 2), the first-line treatment for febrile neutropenic episodes was changed from monotherapy with ceftazidime to piperacillin/tazobactam. In addition, an intense education programme was introduced to improve hygiene to reduce the risk of case-to-case spread. In the final 4 months (Phase 3), ceftazidime was again used as the first-line antimicrobial, while continuing the same level of training in relation to hygiene. The carriage of GRE was measured from rectal swabs done weekly. During the initial 4 months, at any time, 40–50% of patients in the unit were colonized with GRE, and 43 of 75 (57%) new patients initially negative for GRE acquired it within 6 weeks of their admission. In Phase 2, 25 patients out of 129 (19%) acquired GRE, with the acquisition rate falling progressively so that in the last 3 months, only one new patient acquired GRE (logrank comparison of probabilities for cohort 1 vs cohort 2b: P < 0.0001). A return to ceftazidime in Phase 3 was associated with a return of the risk of acquir- ing detectable GRE colonization, despite continued hygiene teaching and surveillance, with 21 out of 58 patients (36%) acquiring GRE (cohort 1 vs cohort 3: P 0.08). Glycopeptide usage was not reduced during the period of the study. Clinical cases were seen only in Phases 1 and 3. Although the reduction in the risk of acquiring GRE may have been due in part to hygiene prac- tices as well as to the change in antimicrobial usage, or may have occurred spontaneously for other reasons, the return of the problem with the reintroduction of ceftazidime strongly sug- gests that this antibiotic was responsible for encouraging the acquisition of detectable GRE. Introduction
with clinical isolates from three patients during one weekand, at that time, eight (38%) of 21 patients were found to
Enterococci have gradually increased in importance as
be colonized on stool culture. Over the following 18
nosocomial pathogens, accounting for up to 12% of all months, surveillance studies confirmed similarly high colo-hospital-acquired infections.1 In addition to intrinsic toler-
nization rates, and there were 12 cases of GRE bacter-
ance to -lactam and aminoglycoside antibiotics, the aemia. This report is of a study to examine the effect ofacquisition of transferable high-level resistance to amino-
replacing ceftazidime as first-line treatment for febrile
glycoside,2 -lactam3 and glycopeptide4,5 antimicrobials has
neutropenic episodes with piperacillin/tazobactam on the
meant that infections with some strains of enterococci are
Ceftazidime is active against most coliforms and pseudo-
Glycopeptide-resistant Enterococcus spp. (GRE) were
monads and perhaps one half of coagulase-negative
first detected on this haematology unit in December 1993,
staphylococci which cause bacteraemia in neutropenic
*Correspondence address. Department of Clinical Microbiology, University College London Hospitals, Grafton Way,
London WC1E 6DB. Tel: 44-171-380-9914; Fax: 44-171-388-8514.
1999 The British Society for Antimicrobial Chemotherapy
S. J. Bradley et al.
patients. However, cephalosporins are, in practice, inactive
lence and acquisition rate of GRE colonization. During the
against enterococci and treatment would be expected to
subsequent 8 months (Phase 2), ceftazidime was replaced
select for an enlarged enteric pool of endogenous entero-
by piperacillin/tazobactam monotherapy for the initial
cocci. Furthermore, cephalosporins have been suggested as
treatment of febrile neutropenia. Throughout the study,
a risk factor for the emergence of GRE.4,6 Piperacillin/
ciprofloxacin was used for -lactam-allergic patients.
tazobactam was chosen as a substitute for ceftazidime in
Glycopeptides (including teicoplanin) were to be reserved
this study because it is more active than cephalosporins for piperacillin/tazobactam-resistant Gram-positive iso-and quinolones such as ciprofloxacin against endogenous
lates or unremitting fever after 48 h. Metronidazole was
penicillin-sensitive strains of enterococci and would there-
preferred to oral vancomycin for presumed antibiotic-
fore not tend to select for bowel overgrowth with these
associated diarrhoea. The change in antibiotic policy
applied to all patients on the unit, including those admittedduring Phase 1 still in hospital or readmitted during Phase2, those declining to participate in the study, and those who
Patients and methods
Patients with haematological malignancy who were ad-mitted to the unit between June 1995 and October 1996
Since the main objective was to reduce the risk of patients
inclusive and who gave informed consent, were recruited to
becoming carriers of GRE, thereby reducing the risk of
the study. The adult haematology unit comprises approxi-
clinical infection due to this group of organisms, new infec-
mately 35 designated beds in three adjacent wards, most
tion control measures were also introduced at this time.
patients being nursed in single rooms. The majority of
These included the identification of GRE carriers by mark-
patients were undergoing marrow or peripheral stem-cell
ing their rooms discreetly (not previously done), intensive
transplants or receiving induction or consolidation chemo-
education of nursing, medical and domestic staff about
therapy for haematological malignancy. Ceftazidime alone
cross-infection and hand hygiene and, in particular, the
had been used for primary treatment of febrile neutropenic
introduction of alcoholic chlorhexidine hand-rub or alco-
episodes since 1988, apart from clinical trials of cipro-
hol gel outside each room. During induction into the study,
floxacin performed in 1988 and of meropenem in 1990–91.
patients were also educated about GRE and likely methods
Gentamicin was added to initial therapy for septic shock.
of transmission, and were encouraged in their own hand
Teicoplanin replaced vancomycin for proven or suspected
hygiene in the ward environment, particularly in the toilets
Gram-positive infections in 1990. Prophylactic antibiotics
and before eating. Alcohol wipes were provided in com-
and gut decontamination were not used for neutropenic
munal toilets as GRE could be isolated from hard surfaces
there. After a review of practices, new guidelines fordomestic staff for ward cleaning were introduced, including(following experiments to demonstrate its efficacy) the
decontamination of hard surfaces in rooms vacated by
Patients were screened for GRE colonization by weekly
GRE carriers with a phenolic disinfectant (Hycolin 2%;
rectal swab. Swabs were enriched in brain heart infusion
Pearson, Glendale, CA, USA). The use of sterilized food
broth (Oxoid, Basingstoke, UK) containing tryptose 10
for neutropenic patients had been discontinued in 1992,
g/L, NaCl 5 g/L, nalidixic acid 7.5 mg/L, colistin 5 mg/L and
and in this study, there were no changes in catering
horse serum 10%, and incubated for 24 h at 42°C. The
practice. Surveillance failed to show GRE in the kitchen
broth was subcultured to selective medium containing bile
aesculin agar (Difco, Detroit, MI, USA), nalidixic acid 15mg/L, colistin 10 mg/L, vancomycin 8 mg/L and horse
serum 10%, and incubated aerobically at 42°C for 24 h. Aesculin-positive colonies were subcultured overnight on
After 8 months in Phase 2, the antibiotic policy was
to 5% horse blood agar, and enterococci identified to
changed back to that in place during the introductory
species level by ‘API Strep’ (Bio-Mérieux, Hazelwood,
phase, with ceftazidime replacing piperacillin/tazobactam.
MO, USA). High- and low-level vancomycin resistance
Educational seminars were held for nursing, medical and
was confirmed by growth up to a 5 g and 30 g disc respec-
domestic staff to ensure that the heightened infection con-
tively on Isosensitest agar (Oxoid).
For 4 months the antibiotic policy was not changed. This
The cumulative total time of exposure on the ward, exclud-
period (Phase 1) was used to establish the baseline preva-
ing periods spent at home, was used to calculate the
Effect of piperacillin/tazobactam on VRE carriage
interval between induction into the study on first admission
were induction and consolidation chemotherapy and
and acquisition of detectable GRE in the rectal swab.
peripheral blood stem-cell transplants. There were minor
Kaplan–Meier time-to-event analysis was done to deter-
changes in the types of patient treated (for example, there
mine the probabilities of remaining free of GRE by cohort,
were more with multiple myeloma in Phase 2) and in the
and logrank tests performed to ascertain statistical signifi-
types of treatment administered (for example, more
cance between cohorts.7 A P value of 0.05 was deemed to
patients had chemotherapy alone rather than transplant-
ation in Phase 2) and, by chance, a decreasing number ofallogeneic bone marrow transplants were done.
Forty-three out of 75 (57%) patients in cohort 1 acquired
GRE. The acquisition rate fell progressively for thosepatients admitted during Phase 2, with 20 out of 70 (29%)
acquiring GRE in cohort 2a, and five out of 59 (8%) in
In total, 293 patients were recruited to the study. Fewer
cohort 2b. Only one patient acquired GRE in the last 3
than 5% of new admissions to the wards refused to take
part. The likelihood of acquiring GRE was analysed in four
The return of ceftazidime in Phase 3 was associated with
separate 4 month cohorts: those admitted to the wards a rise in GRE acquisition for those patients in cohort 3 withduring Phase 1 (cohort 1), during the first 4 months of the
21 out of 58 (36%) becoming colonized.
intervention Phase 2 (cohort 2a), during the second 4
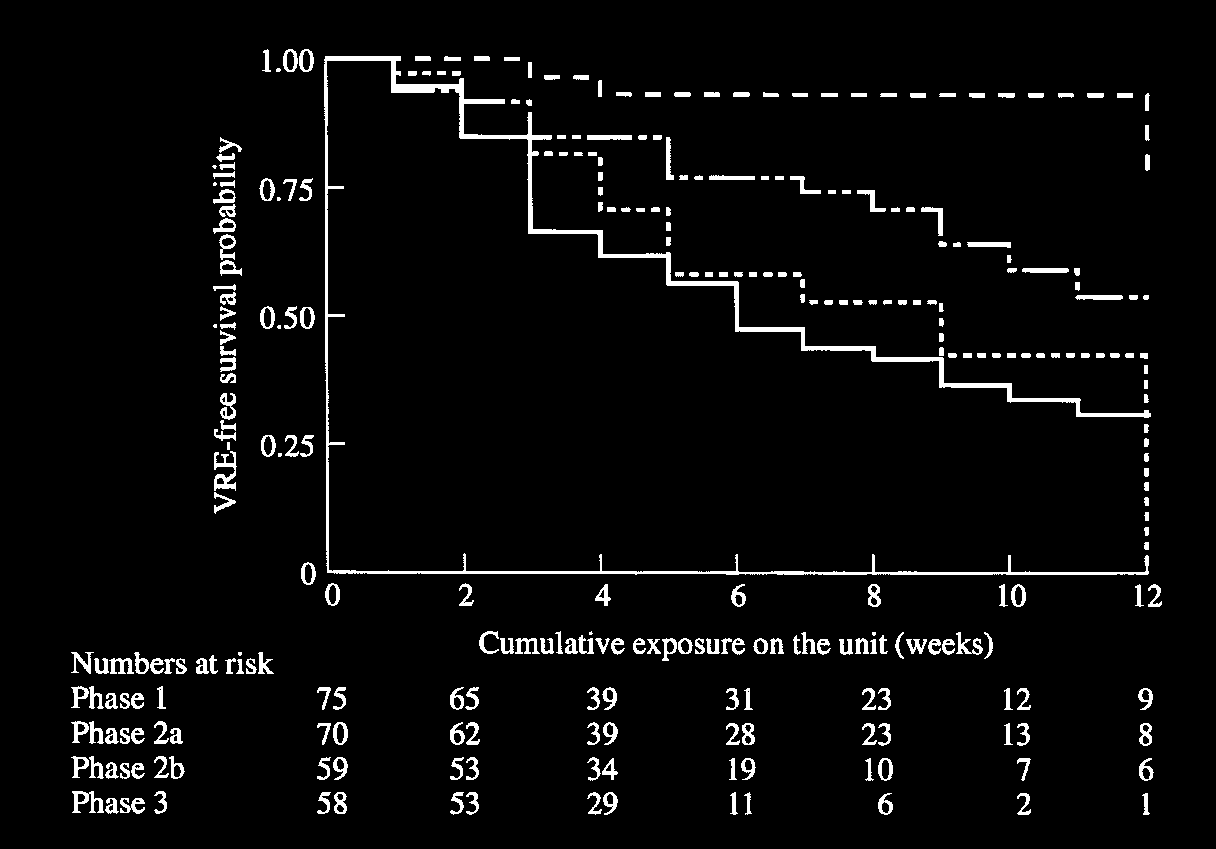
Figure 1 shows the Kaplan–Meier plot of the probability
months of Phase 2 (cohort 2b) and finally during the period
of remaining free of GRE colonization by cohort according
of return to ceftazidime usage (Phase 3 and cohort 3). Once
to time of exposure on the wards. (Time spent at home in
assigned to a cohort, patients were followed up through all
between courses of chemotherapy was not included as
subsequent admissions as belonging to that cohort, what-
exposure.) During the second phase of the study, patients
were significantly more likely to remain free of GRE
Of the patients screened during the first week of the
colonization than during the Phase 1 (cohort 1 vs cohort 2b:
study, 58% were already GRE carriers and were excluded
0.0001), and this improved with time during Phase 2
from subsequent analysis. During Phase 1 as a whole, 27
out of 102 patients were positive on first screening and were
ceftazidime therapy, GRE acquisition rates increased
excluded from Kaplan–Meier analysis. During Phase 2 and
to the level observed in Phase 1 (cohort 3 vs cohort 1:
Phase 3, two out of 131 and two out of 60 patients respec-
tively were positive on first screening and were similarlyexcluded. Overall, this left 262 patients out of the original
GRE isolates obtained by screening
The characteristics of the 262 patients followed up by
Of 544 isolates examined, 476 were Enterococcus faecium.
cohort are shown in the Table. The commonest procedures
All but one isolate were resistant to both vancomycin and
Table. Patient demographics
Most intensive treatment before acquiring GRE or during surveillance (%)
autograft bone marrow/stem-cell transplant
S. J. Bradley et al. Figure 1. Kaplan–Meier analysis to show probability of remaining free of glycopeptide-resisitant Enterococcus spp. (GRE) coloniz- ation by weeks of exposure on the wards from first date of admission. ——, Phase 1; –– - - ––, Phase 2a; – –– , Phase 2b; - - - -, Phase 3.
teicoplanin (VanA phenotype), while a single isolate
patient-days of treatment per month), and paradoxically
used at a very high rate (260 patient-days per month during
phenotype). There were 49 isolates of Enterococcus fae - Phase 2b) when the risk of GRE acquisition was at its calis, 11 isolates of Enterococcus avium—all VanA pheno-
lowest. Very little oral vancomycin was used during the
type, and eight isolates of Enterococcus casseliflavus (VanC
study period, on average 6 patient-days per month during
phenotype, low-level vancomycin resistance).
Phase 1, 3 during Phase 2 and 8 during Phase 3. Discussion
There were five patients with clinical isolates of GRE dur-ing the initial phase of the study: two with isolates from
This study suggests that colonization with GRE can be
urine (one E. faecalis, one E. faecium), two from blood
controlled despite very high endemicity. Replacing cefta-
(both E. faecium) and one with post-mortem isolates from
zidime with piperacillin/tazobactam for broad-spectrum
the spleen and tunnelled intravenous line tip (E. faecium).
antibacterial treatment of febrile neutropenic episodes and
There were no clinical isolates during Phase 2. However, the introduction of improved hygiene were associated within Phase 3, there were three further patients with clinical
a profound reduction in the risk of acquiring detectable
isolates: two from blood (both E. faecium ) and one from
GRE. However, the effect was delayed suggesting that the
urine cultures (E. faecalis), coincident with increased impact of the intervention was complex, and may not haveincidence of detectable rectal carriage.
been detected if patients had simply been randomized to the two antibiotics of interest. The reintroduction ofceftazidime resulted in a significant rise in the risk of GRE
acquisition despite maintaining heightened infection con-
The monthly prescriptions of ceftazidime, piperacillin/
trol measures. The change in incidence of GRE carriage
tazobactam, ciprofloxacin and teicoplanin over the study
was clearly not influenced by teicoplanin usage. Clinical
period are shown in Figure 2. Average ceftazidime usage
cases of GRE infection were only seen when the preva-
was 186 patient-days per month during Phase 1, and 200
lence of carriage was high and not at all during the
patients-days per month for Phase 3. Piperacillin/tazo-
piperacillin/tazobactam phase of the study.
bactam usage was similar during Phase 2, at 197 patient-
Numerous outbreaks of GRE infection and colonization
days per month on average. The use of ciprofloxacin was
have now been documented. Smaller outbreaks have been
fairly constant throughout the study period at an average of
successfully controlled by enforcing strict infection control
57 patient-days per month. Although it was intended that
measures,8–10 but the control of larger outbreaks where
the new antibiotic guidelines and surveillance would
endemicity has become well established has proved more
reduce glycopeptide usage, teicoplanin was used inten-
elusive.11,12 In 1995, the Hospital Infection Control Prac-
sively throughout the study (average 218 (range 126–365)
tices Advisory Committee (HICPAC) from the Centers for
Effect of piperacillin/tazobactam on VRE carriage Figure 2. The usage of the principal intravenous antibiotics (——, ceftazidime; – ––, teicoplanin; · · · ·, piperacillin/tazobactam; –– -––, ciprofloxacin) by month. Phase 1, mid-month 1 to month 4; Phase 2, month 5 to mid month 14; Phase 3, to the end of month 17.
Disease Control, Atlanta issued comprehensive guidelines
At the start of this study, the probability of new patients
aimed at reducing the spread of vancomycin resistance.13
acquiring detectable rectal carriage of GRE in this unit was
These address ‘prudent’ use of vancomycin, education pro-
very high and had been so for at least 18 months according
grammes and the role of the microbiology laboratory in the
to a series of prevalence studies and one 3 month incidence
detection and identification of GRE, and outline measures
study. Although the turn-down in the rate of acquisition of
to prevent and control nosocomial transmission of GRE.
GRE could be ascribed to factors other than the change of
However, these recommendations do not address broad-
ceftazidime to piperacillin/tazobactam, such as improved
spectrum antibiotic usage. A study by Morris et al.11
hygiene, the return of the problem with the reintroduction
showed that reducing oral vancomycin use by 85% and
of ceftazidime, at a time when the prevalence was the low-
intravenous vancomycin by 59%, together with the imple-
est it had been for 30 months while maintaining heightened
mentation of strict infection control practices as outlined
infection control measures, is most persuasive evidence
by HICPAC, failed to reduce the prevalence of GRE.
that ceftazidime alone was responsible.
Quale and co-workers,14 however, showed that restrictingantimicrobials including cefotaxime, ceftazidime and clin-damycin as well as vancomycin could result in a reduction
Acknowledgements
of GRE colonization and infection when the prevalencerate was high, and where infection control measures alone
Dr Bradley and Ms Wilson were generously supported by a
had failed. A similar effect on a different organism was
grant from Wyeth Pharmaceuticals. We are grateful to Ms
observed in a study by Impallomeni et al.15 where a sudden
C. Beer, pharmacist to the leukaemia unit, for invaluable
increase in the incidence of Clostridium difficile diarrhoea
help, to Alison Newberry and Andrew Nunn for statistical
was observed following a 20-fold increase in the use of cefo-
advice and to Professors David Speller, Patrice Courvalin
taxime. Infection control measures did not prevent new
and Roland Leclerq for their encouragement and advice.
cases, but restriction of the use of cefotaxime did. Theeffect of restricting the use of an antibiotic on the suscepti-bility of an organism to that agent has been demonstrated
References
recently in a report by Seppala and co-workers.16 Restrict-
1. Schaberg, D. R., Culver, D. H. & Gaynes, R. P. (1991). Major
ing the use of macrolide antibiotics for the out-patient
trends in the microbial etiology of nosocomial infection. American
treatment of group A streptococcal infections in Finland
Journal of Medicine 38, 72S–5S.
was associated with a reduction in resistance to this agent
2. Horodniceanu, T., Bougueleret, L., El-Solh, N., Bieth, G. & Del-
from 16.5% to 8.6% over 4 years. A number of other bos, F. (1979). High level, plasmid-borne resistance to gentamicin instudies have shown that exerting control over antibiotic
Streptococcus faecalis subsp. zymogenes. Antimicrobial Agents
usage can prevent the spread of antibiotic resistance, and
and Chemotherapy 16, 686–9.
that relaxing these controls will result in the re-emergence
3. Murray, B. E. & Mederski-Samoroj, B. (1983). Transferable
-lactamase. A new mechanism for in vitro penicillin resistance in
S. J. Bradley et al. Streptococcus faecalis. Journal of Clinical Investigation 72,
multiple antimicrobial agents, including vancomycin. Establishment
of endemicity in a university medical centre. Annals of Internal Medicine 123, 250–9.
4. Uttley, A. H. C., George, R. C., Naidoo, J., Woodford, N., John-son, A. P., Collins, C. H. et al. (1989). High-level vancomycin-
12. Wells, C. L., Juni, B. A., Cameron, S. B., Mason, K. R., Dunn, D.
resistant enterococci causing hospital infections. Epidemiology and
L., Ferrieri, P. et al. (1995). Stool carriage, clinical isolation, and
Infection 103, 173–81.
mortality during an outbreak of vancomycin-resistant enterococci in hospitalized medical and/or surgical patients. Clinical Infectious
5 . Leclercq, R., Derlot, E., Duval, J. & Courvalin, P. (1988). Plasmid-
Diseases 21, 45–50.
mediated resistance to vancomycin and teicoplanin in Enterococcus faecium. New England Journal of Medicine 319, 157–61.
13. Hospital Infection Control Practices Advisory Committee (HIC-PAC). (1995). Recommendations for preventing the spread of
6. Frieden, T. R., Munsiff, S. S., Low, D. E., Willey, B. M., Williams,
vancomycin resistance. Infection Control and Hospital Epidemi-
G., Faur, Y. et al. (1993). Emergence of vancomycin-resistant ology 16, 105–13.
enterococci in New York City. Lancet 342, 76–69.
14. Quale, J., Landman, D., Saurina, G., Atwood, E., DiTore, V. &
7. Peto, R., Pike, M. C., Armitage, P., Breslow, N. E., Cox, D. R.,
Patel, K. (1996). Manipulation of a hospital antimicrobial formulary to
Howard, S. V. et al. (1977). Design and analysis of randomised
control an outbreak of vancomycin-resistant enterococci. Clinical
clinical trials requiring prolonged observation of each patient. II:
Infectious Diseases 23, 1020–5.
analysis and examples. British Journal of Cancer 35, 1–39.
15. Impallomeni, M., Galletly, N. P., Wort, S. J., Starr, J. M. &
8. Karanfil, L. V., Murphy, M., Josephson, A., Gaynes, R., Mandell,
Rogers, T. R. (1995). Increased risk of diarrhoea caused by
L., Hill, B. C. et al. (1992). A cluster of vancomycin-resistant Entero-Clostridium difficile in elderly patients receiving cefotaxime. Britishcoccus faecium in an intensive care unit. Infection Control and Medical Journal 311, 1345–6. Hospital Epidemiology 13, 195–200.
16. Seppala, H., Klaukka, T., Voupio-Varkila, J., Muotiala, A., Hele-
9. Livornese, L. L., Dias, S., Samel, C., Romanowski, B., Taylor, S.,
nius, H., Lager, K. et al. (1997). The effect of changes in the
May, P. et al. (1992). Hospital-acquired infection with vancomycin-
consumption of macrolide antibiotics on erythromycin resistance in
resistant Enterococcus faecium transmitted by electronic thermo-
group A streptococci in Finland. Finnish Study Group for Antimicro-
meters. Annals of Internal Medicine 117, 112–6.
bial Resistance. New England Journal of Medicine 337, 441–6.
10. Handwerger, S., Raucher, B., Altarac, D., Monka, J., Mar-
17. McGowan, J. E. (1994). Do intensive hospital antibiotic control
chione, S., Singh, K. V. et al. (1993). Nosocomial outbreak due to
programs prevent the spread of antibiotic resistance? Infection Enterococcus faecium highly resistant to vancomycin, penicillin and
Control and Hospital Epidemiology 15, 478–83.
gentamicin. Clinical Infectious Diseases 16, 750–5.
11. Morris, J. G., Shay, D. K., Hebden, J. N., McCarter, R. J., Received 4 February 1998; returned 9 June 1998; revised 31 JulyPerdue, B. E., Jarvis, W. et al. (1995). Enterococci resistant to
 S. J. Bradley et al.
S. J. Bradley et al.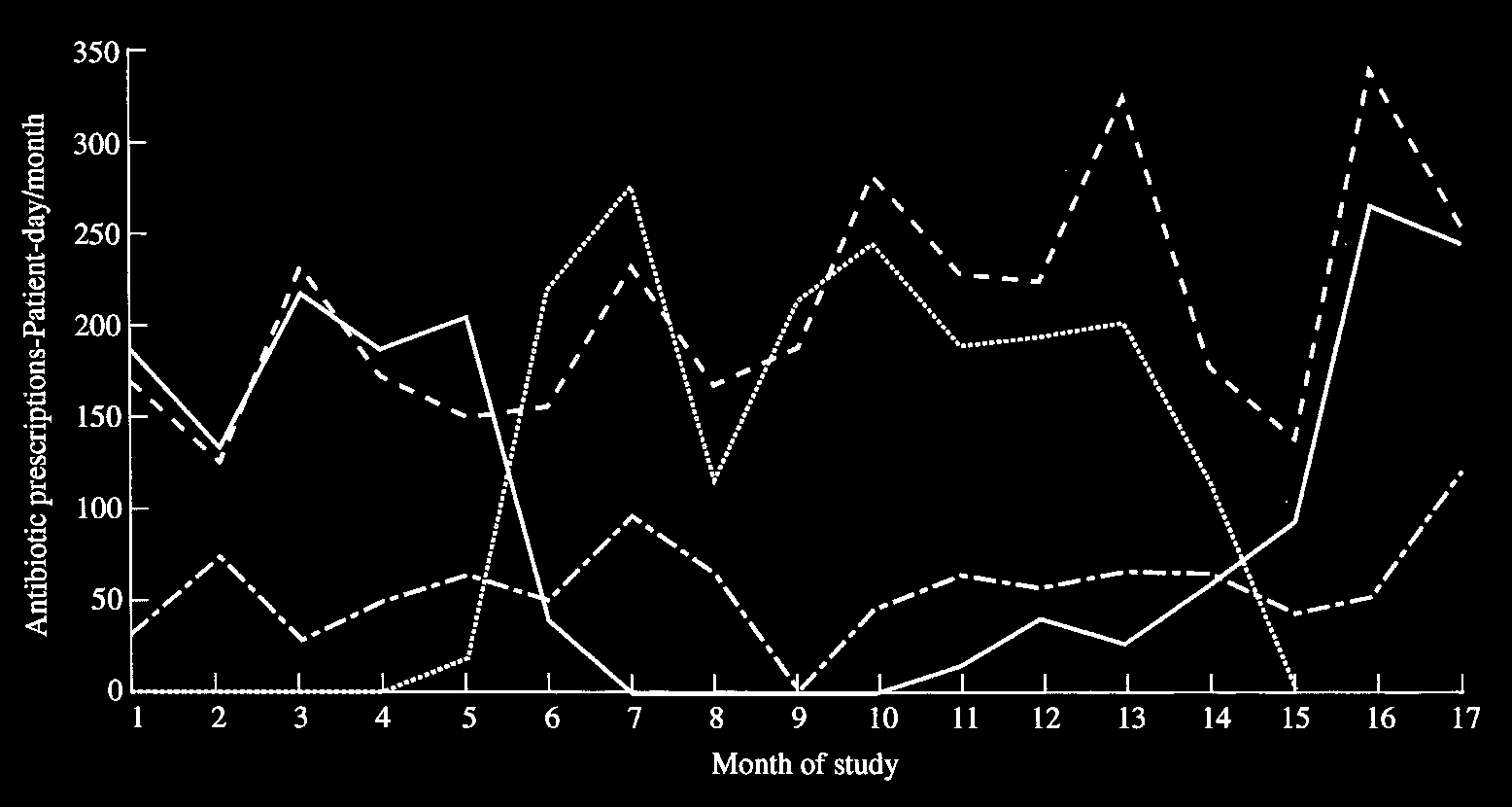 Effect of piperacillin/tazobactam on VRE carriage
Effect of piperacillin/tazobactam on VRE carriage