Ordered, immediately called back and the same day delivered the order.Very pleased with the work. Thank you for prompt and accurate work https://africarx.co.za/buy-levitra-south-africa.html great prices, delivered on the day of the order. Pleasant managers consult by phone.
Proposed moss nutrition tape subjects
Clinical Rounds in Functional and Nutritional Medicine David M. Brady, ND, DC, CCN, DACBN (Food Intolerance) Introduction:
This is the fifth in a series of Clinical Rounds, which will be appearing as a part of ND News & Review. In these Clinical Rounds real case studies from my practice will be presented. It is my aim to present interesting cases, which will facilitate thought and discussion about novel diagnostic and therapeutic techniques for a myriad of clinical conditions that are likely to appear in your offices. Patient Presentation and History:
A 38 year-old female presented with the primary complaint of a severe facial rash. Her entire symptom/complaint list was as follows: • Severe facial rash
• Fatigue • Frequent cold, flu, and laryngitis
• Asthma The onset of her symptoms was approximately 1.5 years prior to presentation, with the exception of her asthma, which dated back to childhood. I particularly remember my medical assistant coming to me after she had taken the patient’s vital signs and saying to me “You are not going to believe the facial dermatitis that this poor woman has.” When I entered the room my immediate impression was that this woman was having a major skin reaction to either a contact or food allergen. Upon completing her medical history I learned that she had been seen by multiple physicians at the Yale College of Medicine, and was actually the focus of a case discussion between the departments of dermatology and allergy at Yale. Prior Management:
Standard patch testing was performed on the patient at Yale, which included various contacts, molds, and foods. The only positives were lanolin, carbol mix, and black rubber mix, all common ingredients in cosmetics. She did not think that these were the cause since she did not customarily wear many cosmetics and total discontinuation did not resolve her problem. She was specifically told that she was not allergic to any foods. She was subsequently put on topical steroid cream, which showed only mild improvement, mostly with the itching. However, the effects diminished over the time and eventually it did not provide any benefit at all. She was then given oral steroids in the low potency class without results. Steroids in the high potency class did not fair much better.
Eventually, she was taken off all medications and told to just use Vasoline on her rashes as a lubricant. She was essentially out of options. She then was told about our integrative medical practice by a friend and presented to us. Physical Examination:
The patient had a well-demarcated eczematous appearing rash involving the forehead, peri-orbital region, cheeks, upper arms and back. Her face appeared “raw” with cracks that appeared to be bleeding. She was obviously very distressed and stated “I am afraid to leave my house because I look like a monster.” EENT examination revealed a reddened oropharynx without tonsillar exudate and obvious candidiasis (aka: “thrush”) along the tongue and bucal mucosa. On follow-up questioning she did admit to frequent vaginal yeast infections and peri-anal itching. Mild lymphadenopathy was noted in the cervical chains. Ears, eyes, and thyroid exams were normal. Heart evaluation revealed a normal rate and rhythm without murmur, and lung examination revealed normal breath sounds. Abdominal examination was essentially normal with the exception of mild tenderness to deep palpation in the extreme quadrants. Initial Impressions:
The presence of this type of skin disorder always causes the functional medicine practitioner to consider an allergy-related problem. The prior work-up by the conventional allergists and dermatologists seems to have ruled out a topical contact allergy, making food allergy a more likely etiology. Since intestinal hyperpermeability (aka: “leaky gut”) can cause a dramatic increase in the antigenic and toxic load into systemic circulation, mucosal gut disorders and hepatic detoxification insufficiency must also be considered as strong contributing factors. The oral thrush, reddened oropharynx, fatigue, and chronic infections may be due to the immunosuppression from the multiple courses of steroids and/or the constant demand placed upon the immune system from the chronic ingestion of antigenic foods. Diagnostic Work-Up: Test Result
Serum Candida Antibodies & Complexes: Negative Epstein-Barr Virus Titers:
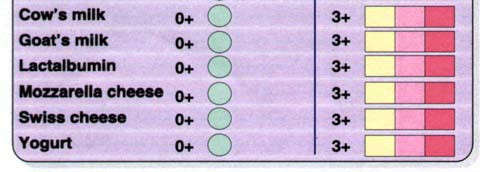
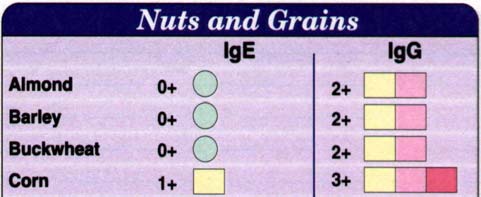
Corn: 3+ (IgG) Salmon, Apricot, Onion, Garlic: 3+ (IgG)
Discussion of Diagnostics:
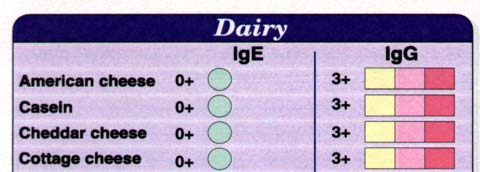
The CBC was performed in order to evaluate the patient for anemia due to the fatigue, as well as to check infectious status. The patient did not appear to be anemic or to have an acute infection. Serum chemistries did not reveal any significant internal pathology. The normal candida serum antibodies and complexes may seem odd given the obvious oral thrush and history of vaginal yeast infections. However, this is seen quite frequently when the yeast is confined mainly to the G.I. tract and has not become systemic. EBV titers were ordered due to the long-standing fatigue and the patient’s history of a severe case of mononucleosis as a teenager. Elevated titers may be contributing to the patient’s fatigue and immunosuppression, and the activation of the virus may be related to the steroid use. The intestinal permeability study showed that lactulose, a large normally non- absorbable sugar, is passing through a “leaky” intestinal mucosa. The smaller sugar, mannitol, is not being absorbed at normal levels, suggesting some degree of malabsorption. While this may seem counter-intuitive to have “leaky gut” and “malabsorption” simultaneously, it is actually seen quite frequently. While the large lactulose is finding it’s way through the gaps between damaged mucosal cells, the smaller mannitol is not being actively absorbed through the cells as it should be due to inflammatory damage of the gastrointestinal villi. This inflammatory damage results in a loss of mucosal surface area and malabsorption. The net effect is a gut that is “leaky” to large molecules (ie: antigenic proteins and large toxins), while a malabsorption of smaller molecules (ie: micronutrients) also exists. Stool analysis was deferred due to the lack of overt G.I. symptoms. It was to be considered if the initial therapeutic strategy did not produce satisfactory results. Hepatic detoxification does not appear to be significantly impaired at this point, but the glutathione phase II conjugation pathway was a bit sluggish. The initial food allergy panel was performed via ELISA IgE/IgG methodology. It was very obvious that the patient had a major problem with dairy. All dairy-related items such as; American cheese, caseine, cheddar cheese, cottage cheese, cow’s milk, goat’s milk, lactalbumin, Mozzarella cheese, Swiss cheese, and yogurt, were all graded as 3+ IgG responses. Further questioning of the patient based on the laboratory results revealed that she had a childhood that included chronic ear infections and antibiotic use. Her parents always made her drink milk, and even to this day she eats a bowl of vanilla ice cream almost every evening as a “comfort food.” She rents a room in the house of a Mexican-American family who cooks most of her meals for her. The Mexican-influenced diet is very high in dairy and corn (another one of her 3+ foods). Can over-exposure to these foods,
combined with a “leaky gut”, resulting in a severe cyclic food allergy and many of her symptoms? Initial Therapeutic Plan:
The initial therapeutic strategy was meant to provide rejuvenation of the skin, improve intestinal function and hepatic detoxification, enhance immune function, and combat the candidiasis and viral challenge. Intervention Goal
• Eliminate dairy & corn from diet
• Mycelized vitamin A (Bio-AE-mulsion: Biotics)
• Diflucan: prescription (not tolerated: withdrawn) anti-fungal
• Lauric acid (Monolaurin: Ecol. Formulations)
• Vitamin C (Bio-C-Plus 1000: Biotics) immune
• Glutamine and GI herbal formulation powder
The patient did not respond well at all to the Diflucan. It was decided to put her on a very brief course of the medication due to the frank oral thrush. However, she experienced headache, and just complained of feeling sick when she took it. It was withdrawn and she was then put on natural anti-fungal products (Allicidin: pre-formed and stabilized allicin extract from garlic, and oil or oregano). 4 Week Follow-up:
• Facial rash 50% improvement
• No apparent oral thrush • Normal pharynx
12 Week Follow-up: • Facial rash 100% resolved • Neck & arm rashes 100% resolved
• No respiratory, throat, or ear infections • Improved energy & vitality
Clinical Management (Long-term): • Elimination of dairy from diet
• Reintroduction & rotation of corn • Multivitamin (Bio-Multi-Plus: Biotics)
• Antioxidant complex (Bio-Protect: Biotics)
• GLA (EPO: Oakmont Labs)
10 Month Follow-up: • Intermittent return of facial rash On a ten-month follow-up visit the patient complained that the rash was just starting to return. She had been attempting to slowly rotate corn back into her diet. At this point it was decided to re-test the patient for food allergy. However, in the intervening ten- month period, our practice started using a different methodology for testing food, molds, and chemical intolerance. This test is known as the Whole Health Food Sensitivity Panel by ALCAT and is performed by Cell Science Systems (CSS) in Deerfield Beach, Florida (800-872-5228 - www.ALCAT.com). This test utilizes whole blood, as opposed to serum alone. Rather than just checking for IgE and IgG antibodies related to certain food proteins, it actually analyses cellular changes that occur to leukocytes when they are exposed to challenge foods. The test utilizes modified Coulter cell analyzer technology, which can accurately and electronically detect minute changes in WBC morphology that result from intolerance or allergy phenomena. For lack of a better analogy, it is basically a very scientific, objective, and far more sophisticated, cytotoxic analysis. This methodology can detect responses that occur on any potential pathway (ie: IgG, IgA, IgM, IgE, IgD, complement, pharmacologic, toxic, lectin, etc.). Given the extreme controversy over IgG testing, as well as the opinion of many leaders in the field that high levels of IgG to a food simply imply frequent exposure and may indeed actually be protective, we have continued to utilize ALCAT more and more with very impressive results. The patient’s results were as follows: Test Results
Additional Discussion:
The decision to utilize the ALCAT test was made in order to determine the level of reactivity of the patient’s known food intolerance and to rule-out a food intolerance that had been missed on the initial ELISA test. In this case the ELISA and ALCAT positives had fairly good correlation. I have found that the ALCAT test does detect the positives that appear on ELISA, but has the advantage of often finding significantly more reactions that are occurring on pathways other than IgE and IgG. It is interesting that cow’s milk was no longer the most reactive substance, probably due to her strict avoidance for an extended amount of time. The attempt at re-introduction of corn may be reflected in the very strong reaction to corn on the ALCAT test. Garlic was also still significantly positive. Additional substances were found to be reactive on the ALCAT test, including; beef and mustard. The patient was informed that re-introduction of corn was probably not possible and she was instructed to completely eliminate dairy, corn, garlic, beef, and mustard from her diet. She was also advised to consider elimination of other members of the allium family, such as onions and leeks. She was given the option of attempting provocation-neutralization therapy for her food intolerance, however, it was my opinion that it was not likely to be very effective so she declined. The patient was also kept on her multivitamin, antioxidant complex, and essential fatty acids. It was decided to re- introduce a small dose of HCL and pancreatic enzymes with meals in an attempt to more adequately digest proteins into less antigenic forms. She was more than willing to follow this supplement program and to simply eliminate these foods if it meant that she would not have to suffer the discomfort and embarrassment of her previous condition. Conclusion:
This patient has not had a return of her rash or other symptoms to date. She has become a strong advocate of my practice and has referred multiple patients. Her case was chosen in order to illustrate the importance of the accurate detection and management of food intolerance in our patients with chronic health problems. This case also serves to outline the functional medicine integrated approach to the management of pan-allergic patients. Intestinal health, digestive function, detoxification, and often adrenal function all need to be evaluated and addressed in order to comprehensively treat these conditions. I encourage and welcome questions and comments regarding this case, as well as other clinical issues. Please direct your questions to me via my web site at
, via e-mail or 1- 203-650-1310. Dr. Brady is a Naturopathic Physician, a Board Certified Clinical Nutritionist, and a Doctor of Chiropractic. Dr. Brady is the Chief Medical Officer of Designs for Health, Inc. He is also presently the Director of the Human Nutrition Institute at the University of Bridgeport, and an Associate Professor of Clinical Sciences at the University of Bridgeport, Colleges of Naturopathic Medicine and Chiropractic in Bridgeport, Connecticut. Dr. Brady also maintains a private practice at The Center for the Healing Arts in Orange, CT, where he specializes in “Functional and Metabolic Medicine”.
By Chuck Palahniuk The View from Smalltown, USA The problem is I don’t have a television so I have to visit people. I listen to the radio. Plus, there’s always the phone and e-mails. I had to call a lot of folks. The other problem is that this is Oregon, 2000 miles from the attack. My friend Mike shrugs and says, “So? If people want to live in New York they need to accept the risks.
ANÁPOLIS SERÁ REFERÊNCIA EM GENÉRICOS Município atraiu atenção das multinacionais e tem a maior planta de medicamentos da América Latina, com 105 mil metros quadrados. João Domingos / BRASÍLIA - O Estado de S.Paulo Anápolis deve tornar-se, dentro de dez anos, o maior polo de medicamentos genéricos do País. Dona da maior planta de medicamentos da América Latina, com 105