Ordered, immediately called back and the same day delivered the order.Very pleased with the work. Thank you for prompt and accurate work https://africarx.co.za/ great prices, delivered on the day of the order. Pleasant managers consult by phone.
Aps1.cdr
IV LIDOCAINE - EFFECTIVE TREATMENT FOR REFRACTORYMIGRAINES AND PAIN IN THE CLINIC
John Claude Krusz, PhD, MD, Jane Cagle, LVN , Stephanie Hall, BS, MPH, William R Knoderer, MD, DDS
Anodyne Headache and PainCare, Dallas, Texas, United States, 75231-4308. CONCLUSIONS
Our primary goal was to provide additional treatment options for our existing headache (and pain)
We conclude that IV lidocaine can be used in the clinic efficaciously and safely for treatment of
patients. Therefore, we did not treat patients that were not already in the practice and well-known to us.
flareups. Sodium channel over-activity may be playing a role in the
Objectives: In the search for additional pharmacologic agents that can be given intravenously in the headache and
Patients had failed at home usual treatment for their migraines. None were allergic to local anesthetics by
maintenance or perpetuation of migraine headaches, as it is known to do in neuropathic pain disorders.
pain clinic, we chose to use IV lidocaine treatment for headache and pain flare-ups refractory to usual treatment at
Lidocaine is safe, very effective and very well tolerated, but must be monitored. Successful treatment may
97 patients were treated (59 female/38 male) [average age 40.8 yrs] for refractory migraine
allow choice of a sodium channel active agent for oral prophylaxis of migraines or neuropathic pain. The
Background: Lidocaine has been used to treat neuropathic pain by virtue of its ability to block sodium channels
headaches and pain flareup in the clinic. 60 patients were treated for pain flareup and 37 patients were
study also raises questions about mechanisms of aberrant neurotransmitter activity involving sodium
and thus block neuropathic pain signaling. On the theory that migraines or other headaches may be, in part,
treated for refractory migraine. A total of 147 lidocaine infusions were administered, as 50 patients
channels playing a role in refractory migraine. This initial open-label study is ongoing in our clinic and
neuropathically mediated, we treated refractory migraines with this agent in the clinic.
received a second lidocaine infusion. Refractory pain disorders that were treated included: lumbar and
double-blind studies are definitely warranted to further explore the validity of IV lidocaine treatment forrefractory migraines, thus offering another excellent treatment option in the appropriate setting. Methods: A total of 97 patients were treated (59 female/38 male) [average age 40.8 yrs] for refractory migraine
cervical radiculopathy (n=42), TMD (n=5), anesthesia dolorosa (n=1), TN (n=4) and CRPS (n=8). 16 of
headaches and pain in the clinic. 60 were treated for pain and 37 for migraines. Refractory pain disorders included:
37 migraine patients (43%) had concomitant pain flareup, usually in the neck and shoulders.
lumbar and cervical radiculopathy (n=42), TMD (n=5), anesthesia dolorosa (n=1), TN (n=4) and CRPS (n=8). Atotal of 147 IV treatments were administered for all patients. An IV line was started with pulse oximetry monitoring.
After initial evaluation by a neurologist or nurse practitioner with weight recorded, an antecubital IV
DISCUSSION
An initial dose of 3mg/kg lidocaine (in normal saline) was infused over 90 minutes. Patients rated initial migraine orpain severity [0-10 VAS] and at timed 15 minute intervals. Following initial treatment, additional 1.5-2 mg/kg
line was started with normal saline and with pulse oximetry monitoring. An initial dose of 3mg/kg lidocaine
lidocaine was infused over 1 hour if there were no side effects and if pain or migraine reduction was less than 50%.
(in normal saline) was infused over 90 minutes. Patients rated their initial pain or migraine severity [0-10
Our preliminary results certainly speak to the efficacy and safety of IV lidocaine in reducing or
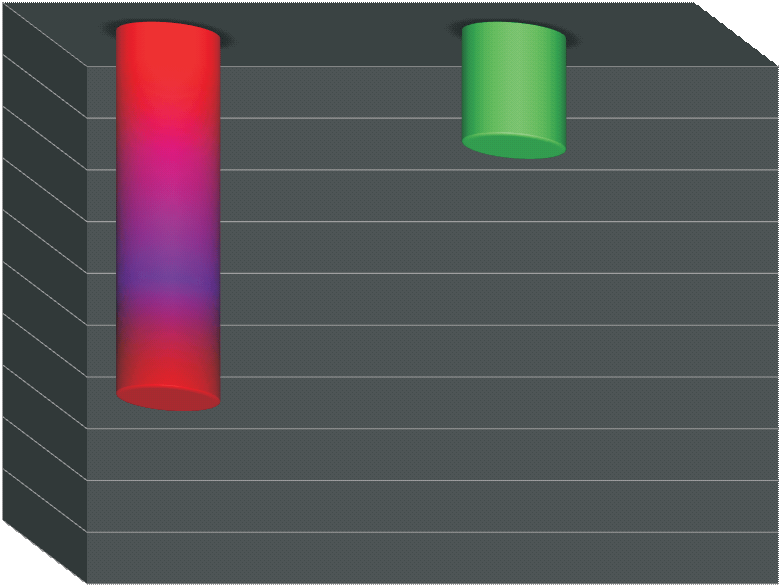
VAS] and at timed 15 minute intervals (see figure 1). Following initial treatment, an additional 1.5-2
Results: The beginning severity for migraines or pain was 7.05/10 before treatment and this was reduced to
abolishing refractory migraine headaches. Review of the literature reveals extremely little data on use of
mg/kg lidocaine was infused over 1-1.5 hours if there were no side effects and if the pain or migraine
2.18/10 in severity after treatment (P. <.001, 2 tailed t test 12). 11 of 37 [32%] patients had complete
this medication in migraines. One study used IV lidocaine to as part of a detoxification protocol for
reduction was less than 50% after the first infusion. Patients were monitored every five to 10 minutes for
abolishment of their migraines. 15 patients were in status migrainosus. 19 of 60 [33%] patients had complete
analgesic overuse headaches and found a 90% success at the end of a weeks’ IV therapy with lidocaine
eradication of pain at the end of infusion. Average time of lidocaine infusion was 135 minutes and average dose was
any side effects such as drowsiness, numbness or dizziness. In most cases, patients had a greater than
and 70% success at 6 months following the treatment [1]. Another study compared IV lidocaine with DHE
334 mg of lidocaine. 50 patients were treated with a second dose of lidocaine. There were 6 patients with transient
#7/10 pain or migraine headache severity, and therefore we recommended that they do not drive to the
and chlorpromazine IV in the ED and found lidocaine to be the least effective agent at 12-24hrs post-
nausea or dizziness transiently during infusion, easily arrested by stopping or slowing the infusion rate. No other
clinic, but rather have somebody bring them.
treatment [2]. A now classic study was done with intranasal lidocaine (4%) and showed efficacy within 15
side effects were seen with treatment.
minutes in 35.8% of 95 subjects treated with 4% intranasal lidocaine compared with 7.4% of 108 subjects
Conclusions: We conclude that IV lidocaine can be used safely and with excellent success in the outpatient
receiving placebo (P < .001). At 6 months, efficacy was maintained in patients who initially displayed a
headache and pain clinic for treatment of refractory pain and migraine flareups. We further conclude that sodium
positive result [3]. Thus, the data is very sparse on use of lidocaine to treat migraines. It is somewhat
channel over-activity or upregulation may be playing a role in the maintenance or perpetuation of pain and migraine
more abundant in the pain literature as an effective treatment for neuropathic pain
headaches. Lidocaine is safe, very effective and very well tolerated, but must be monitored closely duringtreatment. Successful treatment may allow choice of a sodium channel active agent for oral prophylaxis of
Increased neuronal hyperexcitability, including increased sodium channel activity or expression, may
migraines or reduction of neuropathic pain. The study also raises questions about mechanisms of aberrant
well be a crucial process in the pathophysiology of migraines. Neuronal stabilizing agents
neurotransmitter activity involving sodium channels playing a role in refractory pain and migraine conditions.
(anticonvulsants) can reduce this activity and therefore have been used as treatment for migraines.
Double-blind studies are clearly warranted for this effective agent.
Divalproex sodium and topiramate have been approved for this indication in the United States. Oxcarbazepine, lamotrigine and zonisamide, other agents in this group, are sodium channel blockers aswell. Thus, our results suggested switching to a sodium channel agent in our patients with success with IV
lidocaine treatment. Although none of these agents are officially approved for treatment of neuropathicpain, use of these minimum undulating agents is off label for this clinical condition.
Our data is consistent with sodium channel overactivity in refractory migraines and the high rate of
abolishment of allodynia in our patients with this treatment also is supportive for this hypothesis. A recent
review concluded that most of the widely used drugs for migraine prevention work by inhibiting thefunction of either sodium or calcium ion channels. Research done on commonly used migraine prophylactic
drugs, divided into multiple classes, revealed that they all may work on sodium channels, calcium
channels, or both [4,5]. The results do not countermand the simultaneous presence of other
pathophysiological neurotransmitter mechanisms that may summate with or underlie sodium channel
RATIONALE
overactivity. For example, agents that affect glutamate receptor subtypes, calcium channels and CGRP
Lidocaine is a time-proven local anesthetic primarily used for infiltrative anesthesia and as a
component of injection mixtures for various regional and focal nerve blocks. It also has uses in cardiology
to control aberrant cardiac rhythm disorders. Lidocaine’s mechanism of action is to block action potentialfiring in nerve trunks. This is achieved by anesthetics reversibly binding to and inactivating sodium
channels. Sodium influx through these channels is necessary for the depolarization of nerve cell
membranes and subsequent propagation of impulses along the course of the nerve. When a nerve losesdepolarization and capacity to propagate an impulse, the individual loses sensation in the area supplied by
the nerve. The “upstream" consequences at the level of the spinal cord and the central nervous systemare unknown. Lidocaine is thought to exert a central effect in studies of its ability to block neuropathic
CONCLUSIONS
Sodium channel subtypes (NaV 1.4,1.7 and 1.8) have been shown to proliferate or increase or be
upregulated during neuropathic pain processes. Whether a similar activity occurs in refractory migraine
and other headaches is unknown. We wanted to test the idea that migraine headaches may have similarityto neuropathic pain syndromes and that sodium channel overactivity may play a role in maintenance of
ØLidocaine given IV is effective and safe in
migraine headaches, at least after central sensitization may have presumably taken place. We chose to
treating refractory migraines in an outpatient
treat a cohort of refractory migraineurs as well as patients with refractory pain who had failed usual
treatment strategies at home for their migraines. headache clinic setting, providing monitoring is used. OBJECTIVES
Our primary objective and endpoint was to explore the efficacy of IV lidocaine infusion on refractory
ØLidocaine also reduces allodynia in a high
migraines and pain in our patients that had failed treatment with usual medication approaches. Thespecific pharmacology of lidocaine blockade of sodium channels was particularly intriguing. Part of the
percentage of treated patients with migraines.
practice mission is to search for pharmacologic agents that can be given intravenously to treat refractory
migraines, headaches and pain flare-ups. Lidocaine has been under-utilized in this regard, and we choseto study it in our refractory clinic patients in an outpatient setting.
The average severity for patients’ refractory migraines or pain was 7.05/10 VAS before treatment. This
Our secondary endpoint was to demonstrate tolerability of IV lidocaine used in an outpatient
was reduced to 2.18/10 VAS in severity after treatment. 11 of 37 [32%] of patients had complete
ØLidocaine open-label initial results should be
abolishment of their migraines and 19 of 60 [33] patients with painful flareup had complete resolution of
tested double-blind.
pain. 15 patients were in status migrainosus. Average time of lidocaine infusion was 135 minutes andaverage dose was 334 mg of lidocaine. 50 patients were treated with a second dose of lidocaine asspecified above. IV lidocaine treatment resulted in a significant decrease in pain and headache severity (pvalue of <.001, two-tailed t test) [see Figure 1]. 24 patients (65%) had facial or scalp allodynia as part oftheir refractory migraine presentation to the clinic and all but 1 patient had greater than 50% resolution ofthis migraine accompaniment. Allodynia was rated by patients on a 0-10 VAS. Allodynia was 5.44/10 at
[1] Williams, DR, Stark, DJ, Intravenous lignocaine (lidocaine) infusion for the treatment of chronic daily headache with
beginning of treatment and 1.3/10 at end of treatment [see Figure 2]. 6 patients experienced transient
substantial medication overuse, Cephalalgia, 23(10):963-71, 2003
nausea and dizziness during infusion, easily arrested by stopping or slowing the infusion rate. No other
[2] Bell R, Montoya D, Shuaib A, Lee MA, A comparative trial of three agents in the treatment of acute migraine headache, AnnEmerg Med. 19(10):1079-82,1990
side effects were seen with treatment. 26 patients who had success with IV lidocaine were switched from
Maizels M, , Geiger AM, Intranasal lidocaine for migraine: a randomized trial and open-label follow-up,
current prophylaxis to other agents with sodium channel blocking activity (i.e., topiramate, oxcarbazepine,
[4] Cohen GL, Migraine prophylactic drugs work via ion channels, Med Hypotheses. 65(1):114-22,
[5] Krusz, JC, Prophylaxis for Chronic Daily Headache and Chronic Migraine with Neuronal Stabilizing Agents, Curr Pain andHeadache Reports 6:480-5, Dec 2002
29-31 octobre 2012, Ecole Centrale de Lyon, Ecully, France CARACTERISATION DU TISSU OSSEUX HUMAIN PAR NANOINDENTATION P. Crozier1, S Meille1, P Clément1, T Douillard1, I Hadjab2, H. Follet2, J. Chevalier1 et G. Boivin2 1. Université de Lyon, INSA Lyon, MATEIS UMR CNRS 5510, F-69621 VILLEURBANNE Cedex 2. Université de Lyon, INSERM, UMR1033, F-69008, Lyon, France Mots Cl
war resisters’ international internationale des résistant(e)s á la guerre internationale der kriegsdienstgegner/innen internacional de resistentes a la guerra internacio de militrezistantoj 5 Caledonian Road, London N1 9DX, Britain A military constitution for the European Union? Or: The European Union too is on a course towards war This text was written by Tobias Pflüger fr


 IV LIDOCAINE - EFFECTIVE TREATMENT FOR REFRACTORYMIGRAINES AND PAIN IN THE CLINIC
John Claude Krusz, PhD, MD, Jane Cagle, LVN , Stephanie Hall,
IV LIDOCAINE - EFFECTIVE TREATMENT FOR REFRACTORYMIGRAINES AND PAIN IN THE CLINIC
John Claude Krusz, PhD, MD, Jane Cagle, LVN , Stephanie Hall,