Thank you, it's cool. Used for the first time because only then was the right drug. Very revealing detail: ordered Express shipping to get the order within 3 hours because didn't know how to get the order faster https://africarx.co.za/buy-levitra-south-africa.html The drug is authentic exactly. Consistent with the stated prices the Staff is knowledgeable.
Bodyfocushealthgroup.com.au
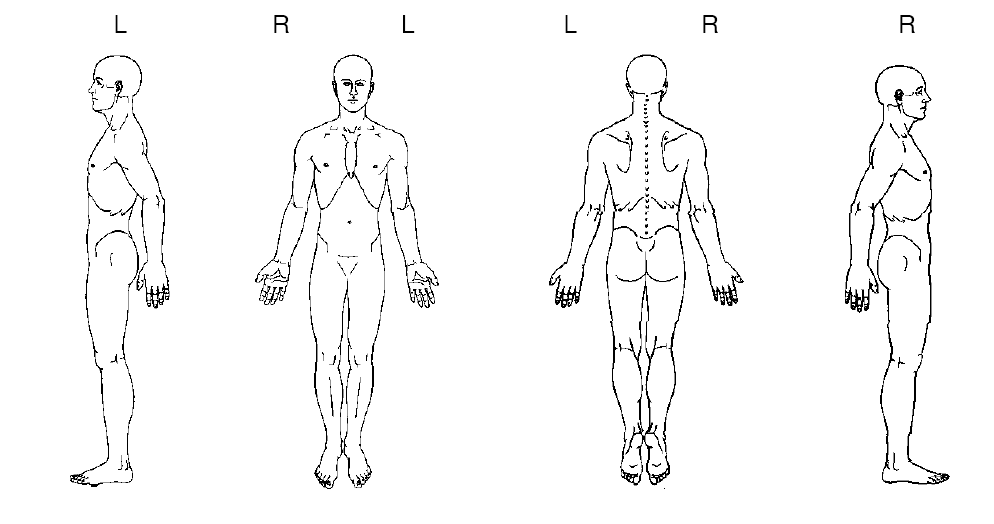
CONFIDENTIAL PATIENT CASE HISTORY As a multidisciplinary practice providing comprehensive care, we focus on your ability to be healthy. Our goals are: firstly, to address the issues that brought you to this practice; secondly, to treat the cause of your condition (not just treat the symptoms or place a temporary patch over your condition); and thirdly, to offer you the opportunity of improved health potential and wellness services in the future. Answering the following questions will give us a profile of your health, and ensure that we optimise your outcome and deliver treatment excellence. What is your major complaint? _________________________________________________________________ Draw on the sketch below the area(s) where you feel your problem to be.
When did your symptoms start? _________________________________________________________________ Was it a gradual or sudden onset? _________________________________________________________________ Have you had this or a similar problem in the past? _________________________________________________________________ If you are experiencing pain, please tick the words that best describe your pain:
Confidential Patient Case History Form Version 1.0,
Do you get?
needles Since the problem started it is:
About the same Getting better Getting worse
What makes your pain worse? Your pain interferes with: What type of work do you do? __________________________________________________________ Any Bladder or Bowel changes since this episode started? __________________________________________________________ Do you experience any nausea, dizziness, difficulty swallowing, changes in vision, or fainting spells, fever, skin rashes associated with your symptoms? __________________________________________________________ Other health professionals seen for this problem (please list): Medical Doctor____________________________________________________________ Specialist Doctor/Surgeon_____________________________________________________ Physiotherapist/Chiropractor __________________________________________________________________ Other __________________________________________________________________ List any medications you are taking __________________________________________________________________ __________________________________________________________________ __________________________________________________________________ __________________________________________________________________ Have you ever taken oral cortisone or prednisone (including asthma medications such as pulmicort, symbicort, flixotide & seretide)? Y/N Are you pregnant? Y/N
Confidential Patient Case History Form Version 1.0,
Do you have or have you ever had?: (please tick)
High blood pressure
Patient’s Signature: _______________ Print Name: ______________________ Practitioner's Signature: _________________ Date: _____________________
Confidential Patient Case History Form Version 1.0,
02_Inhalt_183-302 31.01.2005 7:18 Uhr Seite 237Rempfler · FIFA-Reglement als anationales materielles Recht? FIFA-Reglement als anationales materielles Recht? Lic. iur. Christa Rempfler, St. Gallen Das Handelsgericht des Kantons St. Gallen hat die KlageStreitigkeit dem «Schiedskomitee» der FIFA zu unter-einer in der Schweiz domizilierten Spielervermittlungs-agentur (deren Inhaber die vo
Advice for high altitude expeditions Dr Daniel Martin MBChB, BSc Anaesthetics and intensive care medicine specialist registrar University College London Hospital 10/2005 • Introduction • Acclimatisation • Acute Mountain Sickness (AMS) • How to avoid AMS • Treatment of established AMS • High altitude pulmonary oedema (HAPE) • Prevention of H

 CONFIDENTIAL PATIENT CASE HISTORY
CONFIDENTIAL PATIENT CASE HISTORY 
 Do you have or have you ever had?: (please tick)
Do you have or have you ever had?: (please tick)