Thank you, it's cool. Used for the first time because only then was the right drug. Very revealing detail: ordered Express shipping to get the order within 3 hours because didn't know how to get the order faster https://africarx.co.za/buy-cialis-south-africa.html The drug is authentic exactly. Consistent with the stated prices the Staff is knowledgeable.
Food allergy action plan
Allergy Action Plan Parent to complete top portion. Student’s Name: ___________________________________ D.O.B:_____________ Teacher: ________________ Student is allergic to: _____ Insect stings--type: __________________________________________________________________________________ _____ Foods--type: ________________________________________________________________________________________ _____ Pollens--usual time of year reactions occur: _____ spring, _____ summer, _____ fall, _____ winter _____ Animals—type: _____________________________________________________________________________________ _____ Grass _____ Other: _____________________________________________________________________________________________ Doctor who manages student’s allergies: _____________________________ phone: ____________________fax:____________________
Check signs usually present during an allergy attack:
_____ Swelling (if so, where? ______) Is it severe? Yes / No
The severity of symptoms can quickly change. All symptoms can possibly progress to a potentially life-threatening situation. Emergency contacts: 1. Name ___________________________ Relationship _________________ Phone #1____________________ #2____________________
2. Name ___________________________ Relationship _________________ Phone #1____________________ #2____________________
3. Name ___________________________ Relationship _________________ Phone #1____________________ #2____________________
--------------------------------------------------------------------------------------------------- Healthcare Provider, please complete all areas below: Student is Asthmatic? Yes* No *Higher risk for severe reaction. Action Plan for Allergic Reaction In the event of an Emergency, school staff will follow these steps
FOR KNOWN INGESTION - OR FOR SYMPTOMS OF ANAPHYLAXIS:
1. CALL A CODE BLUE TO ACTIVATE FIRST RESPONDER TEAM. (Student should never be alone once reaction begins.)
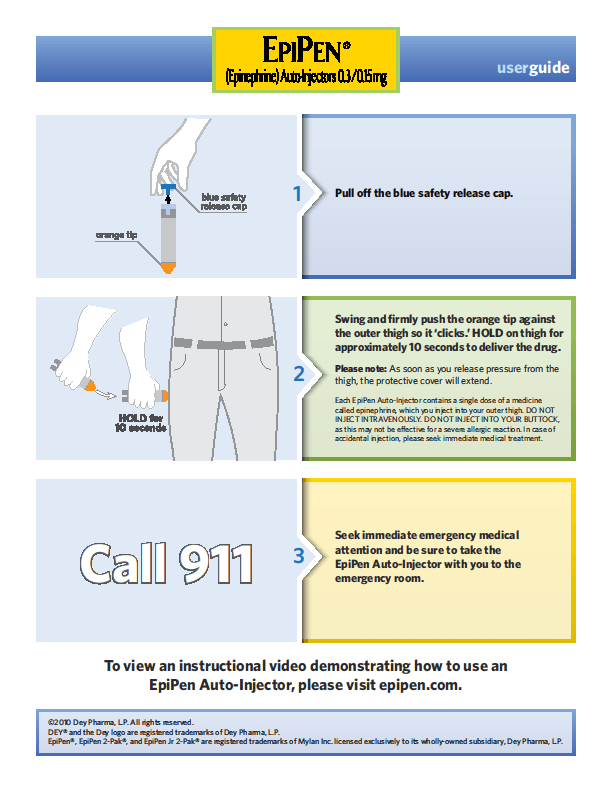
If ingestion/exposure is KNOWN (even without symptoms) OR if ingestion/exposure is SUSPECTED by observing symptoms, administer the
Epinephrine in the UPPER OUTER THIGH (see reverse side for instructions) as ordered below:
EpiPen®, EpiPen®Jr., Twinject™ 0.3mg, Twinject™0.15mg
Epinephrine is stored: ________________________________________________________________________________________________
Time Epinephrine given: ____________ By whom? ______________________________________________________________
Give _______ mg of Benadryl (diphenhydramine)
Time Benadryl (diphenhydramine) given: ____________ By whom? ______________________________________________________________
Call 911. State that an allergic reaction has been treated and additional epinephrine may be needed.
Time 911was called: ____________ By whom? __________________________________________________________________
5. Call parent/emergency contacts-- numbers at top of page.
Student is competent to carry (observed twice/year) and administer his/her own EpiPen® ____Yes ____ No Why/Why not? ____________
Doctor’s Signature______________________________________________________________________________ Date__________________________ (Required for medication authorization of above treatment plan) EVEN IF PARENT/GUARDIAN CANNOT BE REACHED, DO NOT HESITATE TO MEDICATE OR CALL 911!
The school nurse has permission to communicate with the healthcare provider regarding this plan including, but not limited to, orders, clarification of orders, etc. In consideration of the acceptance of the request to perform this service by any person employed by the Rutherford County School System, the undersigned parent or guardian hereby understands and agrees that the Rutherford County School System and its personnel shall not be liable for any injury resulting from the reasonable and prudent assistance in the reasonable performance of health care procedures, including the administration of medication (T.C.A. § 49-5-415). This information may be shared with the appropriate staff. I understand that I am responsible for furnishing the EpiPen®. By signing, parent indicates agreement with the plan action as described above. Parent/Guardian Signature _______________________________________Phone #1 ___________________ #2_____________________ TRAINED STAFF MEMBERS
1) ________________________________________________
6) _______________________________________________
2) ________________________________________________
7) _______________________________________________
3) ________________________________________________
8) _______________________________________________
4) ________________________________________________
9) _______________________________________________
5) ________________________________________________ 10) _______________________________________________
Once EpiPen® or Twinject™ is used, call 911. Send the used unit with student to the Emergency Room. Observation at the Emergency Room may last at least 4 hours. For children with multiple food allergies, consider providing separate Action Plans for different foods. **Medication checklist adapted from the Authorization of Emergency Treatment form developed by the Mount Sinai School of Medicine. Used with permission.
Bisphosphonates in Bone Disease: From the Laboratory to the Patient, Herbert Fleisch, Academic Press, 2000,0122603702, 9780122603709, 212 pages. This book is an essential handbook on bisphosphonates, the mostwidely used new class of drugs for osteoporosis therapy. It reviews basic physiology in addition to theindications and adverse reactions of these drugs. Bisphosphonates in Bone Disease, 4E,
Infectious Diseases Society of America Guidelinesfor the Diagnosis and Treatment of AsymptomaticBacteriuria in Adults Lindsay E. Nicolle,1 Suzanne Bradley,2 Richard Colgan,3 James C. Rice,4 Anthony Schaeffer,5 and Thomas M. Hooton6 1University of Manitoba, Winnipeg, Canada; 2University of Michigan, Ann Arbor; 3University of Maryland, Baltimore; 4University of Texas,Galveston; 5Northwestern Univ
 TRAINED STAFF MEMBERS
TRAINED STAFF MEMBERS