Thank you, it's cool. Used for the first time because only then was the right drug. Very revealing detail: ordered Express shipping to get the order within 3 hours because didn't know how to get the order faster https://africarx.co.za/ The drug is authentic exactly. Consistent with the stated prices the Staff is knowledgeable.
08144v2_layout
A DOUBLE-BLIND, RANDOMIZED, PHASE 2 STUDY TO COMPARE THE SAFETY AND EFFICACY OF INTRAVENOUS CXA-101 (CXA) AND INTRAVENOUS CEFTAZIDIME (CTZ) IN COMPLICATED URINARY TRACT INFECTION (cUTI) O. UMEH1, D. CEBRIK2, I.R. FRIEDLAND1 1Cubist Pharmaceuticals, Inc., Lexington, MA ; 2Axistat, Inc., San Francisco, CA Background: CXA-101 is a novel parenteral broad-spectrum cephalosporin with excellent in vitro activity against
Primary Outcome: microbiological response at the TOC visit, Table 2
Pseudomonas aeruginosa and most Enterobacteriaceae.
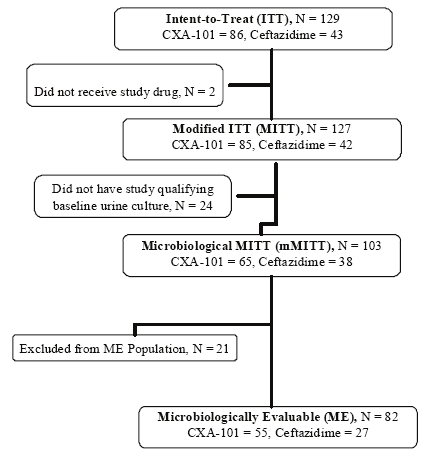
n In total, 129 subjects were enrolled; 86 in the CXA-101 group and 43 in the ceftazidime group, Figure 2
n In the mMITT population, microbiologic cure rates were 83.1% for CXA-101 and 76.3% for ceftazidime
Table 5. TEAEs Occurring in ≥3% of Subjects in Either Treatment Arm
Methods: This Phase 2 study compared the microbiological outcome and safety of CXA-101 vs. ceftazidime (2:1),
q 2 subjects (1 in each arm) were randomized but not treated
n In the ME population microbiologic cure rates were 85.5% for CXA-101 and 92.6% for ceftazidime
both 1g q8h IV for 7 to 10 days, in adult subjects with cUTI, including pyelonephritis. Eligibility for the micro intent-
BASELINE TREATMENT
to-treat (mITT) population required isolation of at least one (but no more than two) pathogen(s) at ≥ 105 CFU/mL
(6 to 9 Days After (21 to 28 Days After
n 103/129 (80%) subjects with a cUTI had qualifying urine culture
n Microbiological cure rates in the mMITT were slightly lower for cLUTI versus pyelonephritis, but were
(Day -2 to 1) (Days 1 to 10)
from a baseline urine culture. To be micro evaluable (ME), a urine culture obtained at the test-of-cure visit (6 - 9 days
82 subjects were microbiologically evaluable
post therapy) and adherence to the protocol were required.
Demographics and baseline characteristics for the MITT and ME populations are summarized in Table 1
Results: 129 subjects were enrolled (86 CXA-101, 43 ceftazidime); 103 had a qualifying urine culture (mITT), 82 were
Both treatments effectively achieved high clinical response rates at the TOC, Table 3
ME. The baseline characteristics were similar in the two treatment groups, 33% had pyelonephritis. Micro cure rates
q E.coli was the most frequently isolated pathogen (70/103 in the MITT Population)
in the mITT population at TOC were 83% and 76% in the CXA-101 and ceftazidime groups, respectively, and in the
n Eradication rates at the TOC in subjects with E. coli, the most common pathogen, were 91.7% in the
ME population were 86% and 93%, respectively. Eradication rates in subjects with E. coli, the most common
CXA-101 group and 94.7% in the ceftazidime group, Table 4
pathogen, were 92% and 95% in the CXA-101 and ceftazidime groups, respectively. Clinical response rates in the
n Sustained clinical cure rates at the late follow-up visit (3 to 4 weeks post therapy) were 98.0% for
mITT were 91% and 92% with CXA-101 and ceftazidime, respectively. Sustained clinical cure rates at the late follow-
Figure 2. Schematic of Analysis Populations and Distribution of Patients
up visit (3 to 4 weeks post therapy) were 98% for CXA-101 and 93% for ceftazidime. Both treatments were well
tolerated; there were no deaths and only 1 serious adverse event; recurrent pyelonephritis in the CXA-101 group. The
most common adverse events were constipation (9% vs 5%), sleep disorder (7% vs 5%), and diarrhea (4 vs 7%). The
Table 2. Microbiological Response (Cure) at the TOC Visit, n/N (%)
incidence and pattern of adverse events were similar in the 2 treatment groups; only 3% of adverse events were severe. Conclusions: CXA-101 showed high micro and clinical efficacy in adult subjects with cUTI, similar to ceftazidime.
n Hospitalized male or non pregnant female subjects, 18 to 90 years inclusive
Both drugs were well tolerated. The results support the further development of CXA-101 for serious gram negative
n Demonstrated clinical signs and/or symptoms of cUTI (including pyelonephritis)
Creatinine clearance (CrCl) ≥ 50 mL/min
n Availability of a study qualifying pre-treatment urine specimen within 48 hours prior to receipt of 1st dose
n Receipt of any amount of potentially therapeutic antibacterial therapy after collection of the pretreatment
baseline urine culture and before the 1st first dose of study drug
Table 3. Clinical Response (Cure) at the TOC Visit, n/N (%)
Urinary tract infections (UTIs) are prevalent in society and their financial burden is significant. In the United
n Receipt of >1 dose of a potentially therapeutic antibacterial agent for the treatment of the current cUTI
States, UTIs account for more than 100,000 hospital admissions annually and up to 40% of all hospital-
within 96 hours before obtaining the study-qualifying pretreatment baseline urine
acquired infections [1]. Complicated UTIs (cUTIs) and pyelonephritis are defined as clinical syndromes in
n Moderate or severe impairment of renal function (CrCl < 50 mL/min, requirement for peritoneal dialysis,
n This is the first clinical study of CXA-101 conducted in a patient population
men or women characterized by the development of the systemic and local signs and symptoms of fever,
hemodialysis or hemofiltration, or oliguria)
n Overall, the demographics and baseline characteristics of the study population were generally similar
chills, malaise, flank pain, back pain, and costo-vertebral angle pain or tenderness, occurring in the
presence of an abnormality of the urinary tract or in the presence of catheterization [2]. Gram-negative
organisms account for approximately 60 to 80% of complicated and nosocomially acquired UTIs [3].
Microbiological outcome at the Test-of-Cure Visit
n The results showed that CXA-101 was therapeutically effective and its activity comparable to ceftazidime
across different analysis sets, regions, and in both cUTI diagnosis groups (cLUTI and pyelonephritis)
CXA-101 is a novel parenteral cephalosporin, being developed for the treatment of serious bacterial infections.
CXA-101 displays potent antibacterial activity in-vitro against common gram-negative and selected gram-
• A urine culture at TOC shows all uropathogens found at baseline at ≥ 105 CFU/mL are reduced to
n Although not considered clinically significant, the disparity in cure rates between treatment groups in the
positive organisms. Its anti-pseudomonal activity is the most potent among all currently available beta-
ME population are likely due to the uneven distribution of some variables despite randomization e.g.
lactams, including the cephalosporins and carbapenems. CXA-101 has broad-spectrum antibacterial
Table 4. Per-Pathogen Microbiologic Eradication Rate (ME Population)
coverage against beta-lactam-resistant Enterobacteriaceae and multi-drug resistant P. aeruginosa.
q 6 subjects in CXA-101 group compared with none in the ceftazidime group had P. aeruginosa –
• A urine culture, taken any time after the completion of therapy, with ≥ 104 CFU/mL of the
(a pathogen known to confer a higher risk for adverse clinical and microbiologic outcomes in cUTI)
n No clinically important unexpected safety signals were observed in this study.
• No interpretable urine culture at the TOC visit and the pathogen was not already classified as
Table 1. Demographics and Baseline Characteristics
Primary objective was to determine the microbiological response 6-9 days after treatment with CXA-101,
n Clinical outcome at the End of Therapy and Test-of-Cure Visits
Resolution of, marked improvement in, or return to pre-infection signs and symptoms and no use
n Secondary objectives included: evaluating the safety of CXA-101 in subjects with cUTI, evaluating the clinical
of additional antimicrobial therapy for the treatment of the cUTI
response at the TOC visit, and determining the pharmacokinetic profile of CXA 101 in subjects with cUTI.
• Persistence of one or more sign or symptom of infection or reappearance of signs and symptoms
n CXA-101 showed high microbiologic and clinical efficacy versus ceftazidime
that requires additional or alternative antimicrobial therapy for the current cUTI (or)
n CXA-101 appeared safe and well tolerated in this group of adult subjects with cUTI
• Adverse event leading to study drug discontinuation and the subject requires alternative
antimicrobial therapy for the current cUTI
n These results support the further development of CXA for serious gram negative infections
MSSA = Methicillin-susceptible Staphylococcus aureus
• Study data are not available for the evaluation of clinical outcome for any reason or the outcome
n This was a Phase 2, multicenter, prospective, randomized, double-blind, efficacy and safety study
comparing intravenous CXA-101 (1000 mg q8h) and intravenous ceftazidime (1000 mg q8h)
n Treatment-emergent adverse events (TEAEs) occurred in 47.1% (40/85) of subjects receiving CXA-101
and 38.1% (16/42) of subjects receiving ceftazidime
n The study sample size was 120 subjects, randomized 2:1 to CXA-101 or ceftazidime
n Inferential statistical analyses were not conducted
n Subjects were stratified by baseline diagnosis: either complicated lower UTI (cLUTI) or pyelonephritis
q Of these, only 1 was considered serious; recurrent pyelonephritis in a CXA-treated subject
q Intent-to-Treat (ITT) Population: all randomized subjects
n The incidence and pattern of AEs were generally similar in the 2 treatment groups, Table 5
Modified-ITT (MITT) Population: all randomized subjects who receive any amount of study drug (safety
n Four subjects (2 in each treatment group) had TEAEs assessed as severe including abdominal pain and
n The study design is outlined in Figure 1
worsening anemia in the CXA-101 group and chest pain and aggression in the ceftazidime group
Wagenlehner FME, Naber KG. Treatment of bacterial urinary tract infections: presence and future. Eur
n A study-qualifying pretreatment baseline urine culture was required within 48 hours before the start of
q Microbiological-MITT (mMITT) Population: subjects in the MITT Population who had at least one
All severe events were assessed as unrelated to study treatment
administration of the 1st dose of study drug,
acceptable causative pathogen from a study-qualifying pretreatment baseline urine specimen
n Two subjects discontinued study drug due to AEs, one subject in the CXA-101 group whose CrCl
Food and Drug Administration. Complicated Urinary Tract Infections and Pyelonephritis - Developing
n No oral antibiotic therapy was permitted
q Microbiologically Evaluable (ME) Population: subjects in the mMITT Population who met the minimal
decreased to <50 mL/min on Day 3, and one in the ceftazidime group who discontinued because of
Antimicrobial Drugs for Treatment, Draft Guidance for Industry. July 1998.
disease criteria, had no protocol deviation likely to impact the microbiological outcome, received an
n Microbiological and clinical response was assessed at the EOT, TOC & LFU visits
Wagenlehner FME, Pilatz A, Naber KG, Perletti G, Wagenlehner CM, Weidner W. Anti-infective treatment
appropriate duration of study drug therapy, had an interpretable urine culture at the TOC visit, and
n Safety was monitored through the review of vital signs, laboratory and physical examinations and the
of bacterial urinary tract infections. Curr Med Chem 2008;15:1412-27.
attended the TOC visit (or was classified as a microbiological failure before the TOC visit)
This study was funded by Cubist Pharmaceuticals.
50th Interscience Conference on Antimicrobial Agents and Chemotherapy
September 12 −15, 2010, Boston, MA, USA
Virginia School Diabetes Medical Management Forms Student ___________________________ School ____________________ Effective Date _______________ Date of Birth ________________ Grade __________ Homeroom Teacher ____________________________ Instructions: 1. Part 1 - Contact Information and Diabetes Medical History . To be completed by parent/guardian and returned to school nurse (p
Mersey & Warrington Guidelines on Prescribing Responsibility for “Red – Amber” Drugs Version 5.0 February 2013 This list is intended to apply across Merseyside and Warrington. However there may be individual differences in some localities and these are noted in the following tables. AIM: It is important for patient care that there is a clear understanding of where cli
 A DOUBLE-BLIND, RANDOMIZED, PHASE 2 STUDY TO COMPARE THE SAFETY AND EFFICACY OF INTRAVENOUS CXA-101 (CXA)
A DOUBLE-BLIND, RANDOMIZED, PHASE 2 STUDY TO COMPARE THE SAFETY AND EFFICACY OF INTRAVENOUS CXA-101 (CXA)