Ordered, immediately called back and the same day delivered the order.Very pleased with the work. Thank you for prompt and accurate work https://africarx.co.za/ great prices, delivered on the day of the order. Pleasant managers consult by phone.
Editinfotech.in
Lanning B. KLine, MD anD RoD FoRoozan, MDI. AnAtomIcAl consIderAtIons (FIgure 12-1)
The trigeminal nerve is a mixed nerve 1.
Motor—ipsilateral muscles of mastication (masseter, temporalis, ptery-goids)
Sensory portion of trigeminal nerve extends from the midbrain to the upper cervical cord
Mesencephalic (rostral) nucleus—proprioception and deep sensation from tendons and muscles of mastication
Extends from pons to upper cervical cord
Divided into segments that correspond to dermatomes that are concentric around the mouth
The trigeminal nerve supplies sensation to the ipsilateral side of the face via three branchesa. V1—Ophthalmic division: frontal, lacrimal, and nasociliary b. V2—Maxillary division: cheek and lower eyelid c. V3—Mandibular division: area of mandible (but not angle of
Motor nucleus lies in pons medially to main sensory nucleus and axons travel with mandibular (V3) division
Figure 12-1. Figure caption will come Please provide figure caption
Three divisions of trigeminal nerve converge at trigeminal (gasserian) gan-glion, which lies in Meckel’s cave of temporal bone
Fibers then travel through main sensory root to brainstem
II. oculoFAcIAl hypesthesIA (see FIgure 12-1)
Distribution of facial numbness or paresthesias helps determine central or peripheral origin 1.
Concentric perioral numbness/paresthesia—central (nuclear) origin (eg, isch-emia, demyelination)
Band of numbness/paresthesia—peripheral origin (ie, V1, V2, V3)
Such somatotopic hypesthesia (eg, V1 only, or V2 and V3 with sparing of V1) suggests that the lesion is more likely to be in the middle cranial fossa (cavern-ous sinus) or orbit
B. Differential diagnosis of diminished sensation in the trigeminal distribution
Perineural spread of skin carcinoma (see Chapter 12, III, B, 5)
Neoplasm, foremen rotundum, sphenopterygoid fossa
Involvement of mental nerve (terminal branch of inferior alveolar nerve)
Frequently due to systemic cancer: breast, lymphoproliferative disorders
iii. Contrast—enhanced imaging (computed tomography [CT] or
magnetic resonance imaging [MRI]) of head including skull base and mandible
Brainstem lesions (dissociated sensory loss)
III. oculoFAcIAl pAIn
Differential diagnosis of relatively common entities associated with ocular and facial pain on the basis of clinical findings 1.
Most commonly with an abnormal anterior segment examination i.
Chronic ocular hypoxia, carotid occlusive disease
Often with a normal anterior segment examinationi.
Glaucoma, including intermittent angle-closure glaucoma
Can occur with or without ophthalmic findings a.
Primary headaches syndromes including migraine and cluster headaches
Herpes zoster—nasociliary nerve involvement indicated by vesicular eruption on side or tip of nose (Hutchison’s sign)
May be followed by postherpetic neuralgia
Referred (dural) pain, including occipital infarction
Cavernous sinus syndromes (see Chapter 7)i. Tumorsii.
m. Elevated intracranial pressure and idiopathic intracranial hypertensionn.
Pain with medullary lesions (eg, Wallenberg syndrome)
Occipital neuralgia can sometimes be confused with other causes of head and facial pain
Any intracranial process irritating the dural sensory fibers, which may be supplied by recurrent branches of V nerve
Neck pain (eg, from osteoarthritis in the cervical spine) may be referred to the eye because of the cervical sensory fibers traveling with the trigeminal fibers of the spinal tract of V, which extends to C-2 level
Trigeminal neuralgia (tic douloureux) a.
Paroxysmal pain in the distribution of one or more of the divisions of V (V3 > V2 > V1)
Recurring, lancinating, “lightning” hemifacial pain lasting 20 to 30 seconds
Pain may be so intense that the facial muscles contract and distort the face during an attack. Frequently “triggered” by touching certain areas of the face or scalp; asymptomatic or mild headache between episodes
No neurologic deficits (including normal corneal reflex)
Neuralgia of more persistent nature and associated with neurologic deficits may resolve from compressive, demyelinative, or inflammatory lesion of the V nerve
Anticonvulsants carbamazepine and gabapentin
Microvascular decompression of aberrant vessel at V nerve root entry zone
Trigeminal ganglion destruction or stereotactic radiosurgery
Pain of herpes zoster is described as severe, burning, aching in quality
Pain occurs over distribution of a dermatome of cranial nerve, usually V1, although it may involve the facial nerve (external ear) with ipsilateral facial palsy (Ramsay Hunt syndrome)
Pain often precedes onset of typical rash by 4 to 7 days
Pain usually regresses within 1 to 2 weeks, but may persist for months or years: post-herpetic neuralgia
Patients typically describe dysesthesias as “crawling” and “prickly” sensations
Treatment frequently is difficult but may includei. Gabapentinii. Pregabaliniii. Tricyclic antidepressantsiv.
Treatment of herpes zoster with antiviral therapy may decrease the risk of postherpetic neuralgia
A vaccine for herpes zoster has been helpful in limiting the morbidity of postherpetic neuralgia
V nerve distribution pain with ipsilateral Horner’s syndrome
Almost exclusively in middle-aged or elderly male patients
May be caused by migrainous dilation of the internal carotid artery with compression of the V nerve and sympathetic plexus in the middle cranial fossa
If the pain is persistent (not of migrainous episodic nature) or if associated with cranial nerve palsy, then suspect a middle fossa tumor, aneurysm, or internal carotid artery dissection
Initial involvement often limited to single nerve branch (especially infra-orbital) but proximal spread leads to cavernous sinus involvement
Often signals recurrence of previously treated tumor, the treatment of which may be forgotten by the patient
Frequently due to squamous cell carcinoma of the face or oropharyngeal mucosa
Diagnosis established with contrast-enhanced MRI
BookMongini F. Headache and Facial Pain. Stuttgart, Germany: Thieme; 1999.
Chapters Glaser JS. Neuro-Ophthalmology. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 1999:64-70. Liu GT. The trigeminal nerve and its central connections. In: Miller NR, Newman NJ, eds. Walsh and Hoyt’s Clinical Neuro-Ophthalmology. 6th ed. Vol 1. Philadelphia, PA: Lippincott Williams & Wilkins; 2005:1233-1274.
Martin TJ, Corbett JJ. Neuro-Ophthalmology—The Requisites. St Louis, MO: Mosby; 2000:223-232. Van Stavern GP. Headache and facial pain. In: Miller NR, Newman NJ, eds. Walsh and Hoyt’s Clinical Neuro-Ophthalmology. 6th ed. Vol 1. Philadelphia, PA: Lippincott Williams & Wilkins; 2005:12751311.
Articles Biousse V, Toubol PJ, D’Anglejan–Chatillon J, et al. Ophthalmologic manifestation of internal carotid
artery dissection. Am J Ophthalmol. 1998;126:565-577.
Clouston PD, Sharpe DM, Corbett AJ, et al. Perineural spread of cutaneous head and neck cancer: its orbital
and central neurologic complications. Arch Neurol. 1990;47:73-77.
Fazzone HE, Lefton DR, Kupersmith MJ. Optic neuritis, correlation of pain and magnetic resoance imag-
ing. Ophthalmology. 2003;110:1646-1649.
Harooni H, Golnik KC, Geddie B, et al. Diagnostic yield for neuroimaging in patients with unilateral eye
or facial pain. Can J Ophthalmol. 2005;40:759-763.
Lee AG, Beaver HA, Brazis PW. Painful ophthalmologic disorders and eye pain for the neurologist. Neurol
Levin LA, Lessell S. Pain: a neuro-ophthalmic perspective. Arch Ophthalmol. 2003;121:1633. Pavan-Langston D. Herpes zoster: antivirals and pain management. Ophthalmology. 2008;115(2
Prasad S, Galetta S. Trigeminal neuralgia; historical notes and current concepts. Neurologist. 2009;15:87-94. Ringeisen AL, Harrison AR, Lee MS. Ocular and orbital pain for the headache specialist. Curr Neurol Neurosci Rep. 2011;11:156-163.
Diablo Blue October, 2002 The Monthly Newsletter of the Diablo Valley PC User’s Group October 3, 2002 Meeting Announcement Ask Dr. Tech and HP Do you have problems with your computer? Your software? Your hardware? Don’t know which? Do you wonder how you can get those problems solved? Well, Ask Dr. Tech may be the right choice for solving your problems. William Lam, preside
Consider Japan : there’s a country that deliberately protected itself from history during three centuries ; it put a barrier between history and itself, so well that it perhaps permits us to foresee our own future . Now, what Japan teaches us, is that one can democratise snobbery . Next to the Japanese, English high society is a bunch of drunken sailors (Kojève, 1968, see Nichols, 200
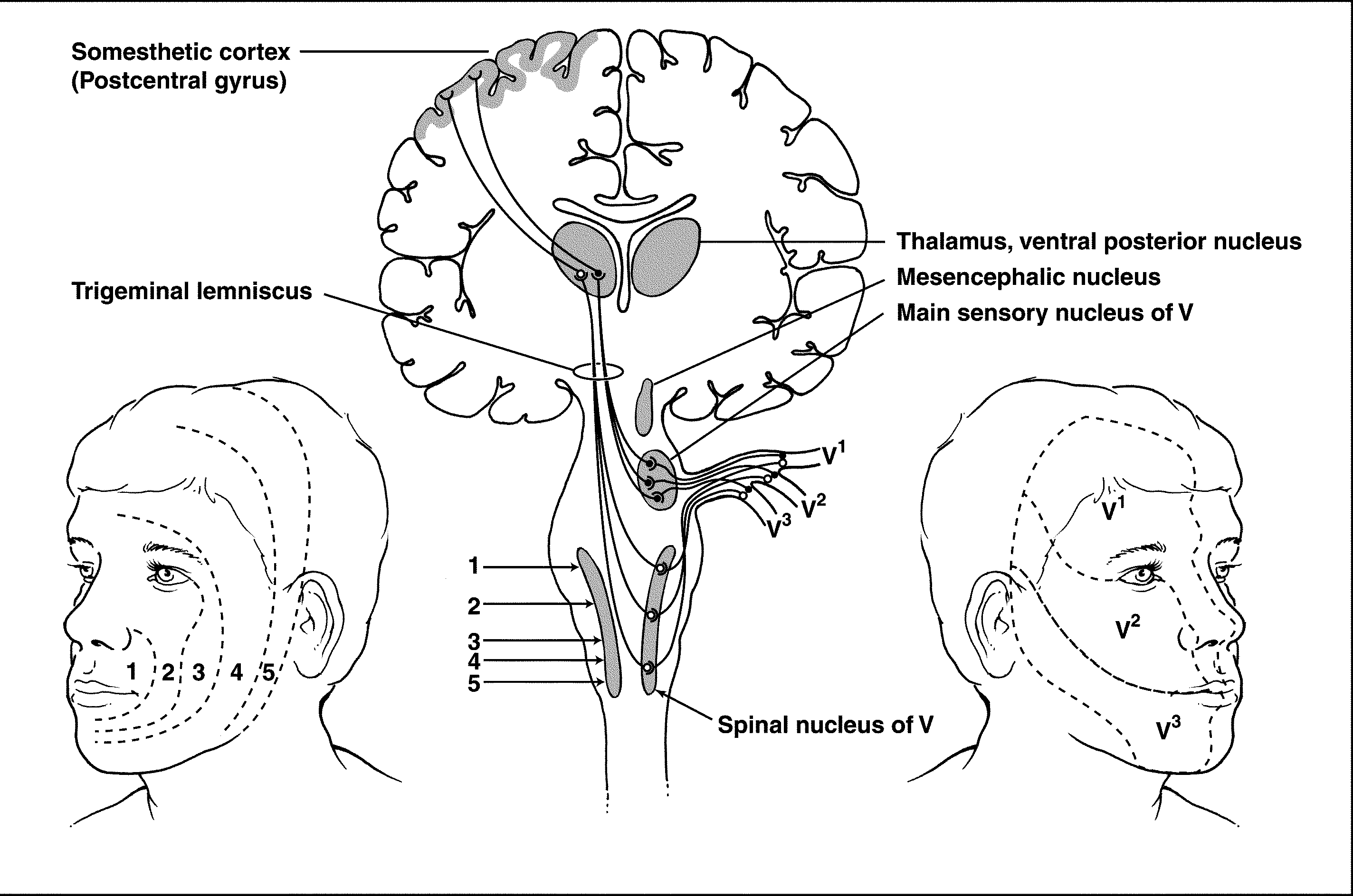 Figure 12-1. Figure caption will come
Figure 12-1. Figure caption will come