Thank you, it's cool. Used for the first time because only then was the right drug. Very revealing detail: ordered Express shipping to get the order within 3 hours because didn't know how to get the order faster https://africarx.co.za/ The drug is authentic exactly. Consistent with the stated prices the Staff is knowledgeable.
Eprints2008.lib.hokudai.ac.jp
Coexistence of a systemic lupus erythematosus and porphyria cutanea tarda: case successfully improved by avoidance of sun exposure
Junko Murata, Tadamichi Shimizu, Yasuyuki Tateishi, Riichiro Abe and
Department of Dermatology, Hokkaido University Graduate School of
Medicine, Kita-ku, Sapporo 060-8638, Japan.
Reprint requests to: Tadamichi Shimizu, Department of Dermatology,
Hokkaido University Graduate School of Medicine, Kita-ku, Sapporo
Keywords: systemic lupus erythematosus, porphyria cutanea tarda
A 46-year-old Japanese woman presented with vesicles on her nose and
the dosal aspect of her hands since 3 months. Physical examination
revealed tense blisters and atrophic erythematous plaques on her arms and
the dosal side of her hands (Fig. 1a). Erosions were also scattered on the
face (Fig. 1b). She also had hypertrichosis on her face. The patient was first
diagnosed as having systemic lupus erythematosus (SLE) in 1997 at the
age of 41 years, when she presented with alopecia, fever, arthralgia,
Raynaud’s phenomenon, hemolytic anemia and lymphadenopathy. Liver
transamirase levels were slightly elevated. She had no sign of hepatitis
including autoimmune hepatitis, drug-related hepatotoxity, alcoholic hepatitis,
or viral infection. Systemic lupus eryhtematosus was well-controlled with a
At age of 43 years she developed erythematous plaques with scaling on
the back of her hands. Clinically the skin erupution at that time appeared to
be discoid lupus erythematodes. She was treated with a steroid ointment
and her eruptions gradually improved, but new skin lesions repeatedly
Laboratory investigations at age 46 years while taking PSL 5mg
disclosed the following results: white cell count 3.9
10 9/l. Liver function profile included total bilirubin was
1.7 mg/dl, GOT 46 IU/l, GPT 82 IU/l, γ-GTP 142 IU/l and alkaline
phosphatase 456 IU/l. Renal function and electrolytes were normal.
Antinuclear antibody (ANA) titers were positive at a dilution of 1/80 (normal
value,1/40) with a homogeneous pattern. Histopathological examination of
the back of the hands demonstrated a subepidermal blister with slight
inflammatory infiltrate. No eosinophilic deposit around the vessels and little
edematous change was present in the dermis. (Fig. 2). Direct
immunofluorescence revealed a granular fashion at the dermoepidermal
junction (DEJ) with IgG, IgM, and C3. Deposition of C3 around the blood
vessels and several clusters of colloid bodies associated with IgM were also
observed in the upper dermis. Laboratory value of fractionated porphyrins in
her urine revealed the following: uroporphyrin 1080 µg/l (normal:<20),
coproporophrin 110 µg/l (normal <100), porphobironogen 1.3 mg/l (normal
<2), and δ-aminolevulinic acid 3.5 mg/dl. The value of porphyrins in her
serum was within the normal range, confirming the diagnosis of PCT.
Subsequently, she was treated with topical steroid ointment, and avoidance
of sun exposure was implemented. Three months later the value of
uroporphyrin and coproporphirin in her urine was almost normal and no
Since the association of SLE and PCT was first described by Linden in
1954 (1), approximately 50 cases of LE (all variants) have been described in
association with PCT, including 15 cases reported by Gibson and McEvoy
(2). PCT results from decreased activity of uroporphyrinogen decarboxylase
(UROD). Alcohol, oral contraceptives, polychlorinated hydrocarbons,
disturbances of iron metabolism, hepatitis C and infection with HIV are
recognized as precipitant factors for PCT (3). Approximately 80 % of PCT
patients have the sporadic form in which UROD deficiency is restricted to
the liver and the remainder has the familial type in which mutations in the
UROD gene are inherited in an autosomal dominant pattern (4).
It is not known whether the association between PCT and LE is
coincidental or represents some common link. Harris et al. have suggested
possible explanations for the coexistence of LE and porphyria: a common
genetic abnormality, porphyria triggering an autoimmune response,
preexisting LE resulting in an acquired metabolic fault leading to porphyria,
and LE precipitating a genetically determined metabolic fault resulting in
porphyria (5). It is interesting that the gene for UROD is located on
chromosome 1 (6), and that the 1q41-q42 region of that chromosome is
Our patient did not drink much alcohol, take oral contraceptives, nor had
any blood transfusions. She did not have HCV or HIV infections. Her liver
function test was abnormal, and therefore dysfunction of her liver caused by
SLE may have been a factor in precipitating the PCT. She has suffered from
hemolytic anemia since 1997, so an overload of iron may have caused liver
dysfunction and could also have precipitated the PCT. The histological
findings of the subepidermal blistering are compatible with PCT, and positive
immunofuluorescence staining at the DEJ may have been caused by the
Association of SLE and PCT is not common, and this combination
usually poses practical problems and occasionally therapeutic dilemmas.
Phlebotomy is one treatment for PCT, but it is not advisable in LE patients
who have anemia. Antimalarials are used for the treatment of LE and PCT.
Severe toxicity can result from using high dose of chloroquine(8), and
hydroxichloroquine may also be associated with abdominal crises in some
cases. (9). However, low-dose chloroquine therapy has been shown to be
effective without causing serious hepatotoxicity(10). Therefore, it is
important to avoid high-dose chloroquine therapy in cases of joint LE and
Our patient’s skin lesion and the quantity of porphyrines in her urine have
been improved since she started the avoidance of sun exposure together
with the topical steroid ointment treatment. Strict total sun protection should
be recommended to patients with PCT and SLE because both conditions
can be activated by long wavelength light bound in sunlight.
REFERENCES
1. Linden IH, Steffen CG, Newcomer VD, et al. Development of porphyria
during chloroquine therapy for choronic discoid lupus erythmatosus. Calif
2. Gibson GE, McEvoy MT. Coexistence of lupus erythematosus and
porphyria cutanea tarda in fifteen patients. J Am Acad Dermatol
3 O’Connor WJ, Murphy GM, Darby C, et al. Porphyrin abnormalities in
acquired immunodeficiency syndrome. Arch Dermatol 1996;132:1443-1447
4. Elder GH. Porphyriacutanea tarda. Semin Liver Dis 1998;18:67-75
5. Harrris MY, Mills GC, Levin WC. Coexistent systemic lupus
erythematosus and porphria. Arch Intern Med 1966;117:425-428
6. Wu C, Xu W, Kozack CA, et al. Mouse uroporphyrinogen
decarboxylase: cDNA cloning, expression, and mapping. Mamm
7. Tsao BP, Cantor RM, Kalunion KC et al. Evidence for linkage of a
candidate chromosome I region for human systemic lupus
erythematosus. J Clin Invest 1997;99:725-731
8. Felsher BF, Redeker AG. Effect of chloroquine on hepatic uroporphrin
metabolism in patients with porphyria cutanea tarda. Medicine
9. Koranda FC. Antimalarials. J Am Acad Dermatol 1981,4: 650-655
10. Taljaard JJF, Shanley BC, Stewart-Wynne EG, et al.
Studies on low dose choloroquine therapy and the action of chloroquine
in symptomatic porphria.Br J Dermatol 1972;87:261-269
LEGENDS FOR FIGURES Fig 1. (a) Right hand with a tense blister, erosions and several pigmented
lesions. (b) Numerous erosions on the face. Fig 2. Subepidermal blister with slight inflammatory infiltrate. No
eosinophilic deposit are observed around the vessels and few edematous
change were present in the dermis.(H&E
Murata et al. Murata et al.
(C) Tax Analysts 2010. All rights reserved. Tax Analysts does not claim copyright in any public domain or third party content. It’s Not Just Academic: The OECD Should ReevaluateTransfer Pricing Lawsby Michael C. DurstMichael C. Durst is a tax lawyer practicing in Washington, and during the mid-1990s served as director ofthe Advance Pricing Agreement Program, the Internal Revenue Service adv
VISION & MISSION STATEMENT VISITATION TO SCHOOL AND CLASSROOMS GENERAL EQUAL OPPORTUNITY & NONDISCRIMINATION STATEMENT ARRIVAL TIMES FOR CHILDREN ARRIVAL/DISMISSAL INSTRUCTIONS TARDINESS ATTENDANCE VISITS AFTERNOON DISMISSAL BAD WEATHER DAYS: COLLABORATION SCHEDULE PARKING AREAS FOR PARENTS / VISITORS CHILDREN LEAVING SCHOOL DURING SCHOOL HOURS

 Murata et al.
Murata et al.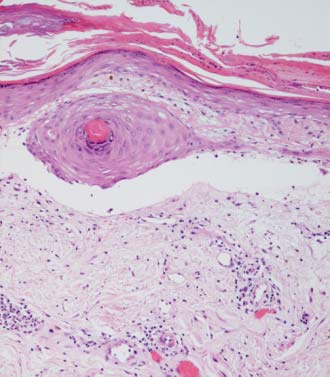 Murata et al.
Murata et al.