Ordered, immediately called back and the same day delivered the order.Very pleased with the work. Thank you for prompt and accurate work https://africarx.co.za/buy-cialis-south-africa.html great prices, delivered on the day of the order. Pleasant managers consult by phone.
834 115.119
International Clinical Psychopharmacology 2002, 17:115–119
Quetiapine augmentation in patients withtreatment resistant obsessive^compulsivedisorder: a single-blind, placebo-controlled study
M. Atmaca, M. Kuloglu, E. Tez can and O. Gecici
Firat University, Medical Faculty Hospital, Department of Psychiatry, Elazig, Turkey
Correspondence to Murad Atmaca, Firat (Euphrates) Universitesi, Firat T|p Merkezi, PsikiyatriAnabilim Dali, 23119 Elazig,TurkeyTel: +90 424 233 3555/2282 2300; fax: +90 424 2388096; e-mail: matmaca _ p@yahoo.com
Received 19 September 2001; accepted 21 February 2002
Recently, atypical antipsychotics have been used for the management of the patients with refractory obsessive–compulsive disorder(OCD). The aim of the present study was to evaluate the results of quetiapine augmentation to a serotonin reuptake inhibitor (SRI)in the patients with refractory OCD. Fifty-two patients with OCD according to DSM-IV entered 3 months of an open-label phasetreatment with a SRI with or without concomitant adjunctive treatment regimen. Of them, 27 patients were refractory OCD. Thesepatients were randomly divided into two groups, SRI plus quetiapine and SRI plus placebo, for an 8-week single-blind phase. Thecourse of OCD was evaluated by Yale–Brown Obsession–Compulsion (Y-BOCS) and Clinical Global Impression–Severity ofIllness and Improvement (CGI-SI and I) Scales every other week for 8 weeks. Of the 14 patients in group I, nine (64.4%) showedsignificant improvement with 60% or greater improvement on the Y-BOCS and one (7.1%) partial improvement with 30% orgreater improvement on the Y-BOCS, whereas no improvement was observed in group II. The addition of quetiapine to ongoing SRItherapy has been found to be effective and well-tolerated approach in patients with refractory OCD. Int Clin Psychopharmacol 17:115–119r 2002 Lippincott Williams & Wilkins
Keywords: augmentation,OCD,quetiapine,refractory,SRI
Young et al.,1994). The addition of risperidone orolanzapine to SRI has been shown to be considerably
Serotonin reuptake inhibitors (SRI) are used in the
beneficial (Saxena et al.,1996; Weiss et al.,1999). On
treatment of the patients with obsessive–compulsive
the one hand,to the best of our knowledge,there is no
disorder (OCD) as the first choice. However,approxi-
available information about using quetiapine (alone or
mately 40–60% of patients do not response to this
with a SRI),a new atypical antipsychotic derived
treatment and obsessive–compulsive symptoms persist
dibenzothiazepine,in the treatment of OCD. On the
(Goodman et al.,1989b). One of the approaches in
other hand,although they differ in some pharmacolo-
treatment of refractory OCD is to add to another
gic properties [e.g. quetiapine has high affinity for a1
group of drug to SRIs. Addition of central serotonin
adrenergic and histamine H1 receptors,lower affinity
(5-HT) enhancers such as lithium (McDougle et al.,
for a2 adrenergic and dopamine D1 receptors and no
1991) and buspirone (McDougle et al.,1993) plus SRI
muscarinic M1 activity (Saller and Salama,1993),
has not been found effective,whereas adding dopamine
olanzapine has high affinity for a1 adrenergic,hista-
receptor antagonists,such as pimozide and haloper-
mine H1,dopamine D1 receptors and muscarinic M1
idol,has been shown to be effective in the treatment of
activity (Bymaster et al.,1996) and risperidone’s
refractory OCD with comorbid schizotypal personality
pharmacologic profile demonstrates a somewhat lower
disorder or chronic tic disorder (McDougle et al.,1990;
affinity for a1 and a2 adrenergic and histamine H1
receptors (Leysen et al.,1988)],quetiapine has some
Atypical antipsychotics have also been tried in the
similarities with risperidone and olanzapine in regard
patients with treatment resistant OCD (Patil,1992;
to receptor binding profile,such as greater affinity for
0268-1315 r 2002 Lippincott Williams & Wilkins
International Clinical Psychopharmacology 2002,Vol 17 No 3
serotonin-2 (5-HT2) receptors than dopamine D2
of three of the authors (M.A.,M.K. and E.T.) that the
receptors. Therefore,we decided to evaluate the results
of quetiapine augmentation to SRI in the patients withtreatment resistant OCD.
Dose and procedureThe subjects were randomly assigned to two groups:SRI plus quetiapine (group I) (n ¼ 14,seven femalesand seven males) and SRI plus placebo (group II)
(n ¼ 13,six females and seven males). The randomassignment was single-blind. Quetiapine (50 mg/day)
or placebo was added to SRI at the beginning of the
Of the patients who had applied to Firat University
study. Quetiapine was increased to a dose of 25 mg/day
Medical Faculty Department of Psychiatry,and who
in each 2-week period,if the Y-BOCS score did not
were diagnosed with OCD without psychotic features
decrease by 2 or more. Placebo remained stable
according to DSM-IV (APA,1994) between September
throughout the study period. SRI doses were stabilized
and December 2000,52 gave their written informed
(fluoxetine 40 mg/day in five patients in both group I
consent to take part after receiving a complete
and II; fluvoxamine 200 mg/day in five patients in
description of the study. The study protocol was
group I and in four patients in group II; and
approved by the Firat University School of Medicine
clomipramine 150 mg/day in four patients in group I
and in four patients in group II). No other drugs and
First,52 patients entered 3 months of an open-label
formal behaviour therapy were given. The course of
screening phase. All patients received at least one
OCD was evaluated by Y-BOCS and CGI every other
adequate SRI trial before this phase. The SRI
week for 8 weeks. The instruments were administered
treatment was started at the dose of 37.5 mg/day for
by the same rater (M.A.) throughout the study.
clomipramine,50 mg/day for fluvoxamine or 20 mg/day for fluoxetine,and titrated up to 300 mg/day forclomipramine,300 mg/day for fluvoxamine and 80 mg/
day for fluoxetine according to clinical response and
Data were evaluated by the SPSS Statistical Package,
experienced side-effects [fluoxetine (maximum 80 mg/
version 9.05. (SPSS,Chicago,IL,USA). Comparisons
day,mean 46.6 mg),fluvoxamine (maximum 300 mg/
were performed using the chi-square test and Student’s
day,mean 140.8 mg) and clomipramine (maximum
300 mg/day,mean 185.5 mg)]. In some patients,eithera combination of SRI and anxiolytic (clonazepam intwo patients and alprazolam in one patient),pimozide
(in one patient) or lithium carbonate (in two patients)was given. Nineteen patients responded to this treat-
Fourteen patients were randomized to quetiapine and
ment regimen. Four patients dropped out of the study
13 patients to placebo administered group. The mean
due to treatment incompliance and two were excluded
age of the patients was 28.6 years (SD 8.5; range 18–
from the study due to intolerance. Therefore,27
44 years) and 28.1 years (SD 8.7; range 20–49 years) in
patients entered the 8-week,single-blind and placebo-
groups I and II,respectively (P40.05). The mean age
at onset was 21.3 years (SD 5.2) and 22.1 years (SD
Refractoriness to treatment were accepted when all
4.7) in groups I and II,respectively (P40.05). The
following criteria were met: (i) still having a Yale–
mean previous failed adequate SRI trial was 1.9 (SD
0.7; range 1–3) in group I and 2.1 (SD 0.6; range 1–3)
(Goodman et al.,1989a) score of 18 or greater
in group II before starting open-label phase (P40.05).
(Goodman et al.,1989b); (ii) the agreement of three
Eight patients from group I and six from group II had
of the authors (M.A.,M.K. and E.T.) that the patient
failed trials of behaviour therapy. The most frequent
was not enough improved; and (iii) minimal improve-
obsession and compulsion were dirt contamination
ment on Clinical Global Impression–Improvement
(n ¼ 13) and washing (n ¼ 12) for entire sample.
Of the patients,14(51.9%) had comorbid axis I
In order to determine the response to 8-week
disorder. These comorbid disorders were major de-
treatment,the following criteria were used: (i) 60%
pressive disorder (n ¼ 8),social phobia (n ¼ 2),hypo-
or greater improvement on the Y-BOCS (significant
chondriasis (n ¼ 2) and panic disorder (n ¼ 2). There is
improvement); (ii) 30% or greater improvement on Y-
no statistically significant difference between treatment
BOCS (partial improvement); and (iii) the agreement
groups with respect to the distribution of comorbid
116 International Clinical Psychopharmacology 2002,Vol 17 No 3
Table1. Comparison of scale scores (mean7SD) both at baseline and endpoint of the quetiapine or placebo addition phaseand that of responders at endpoint
aStudent’s t-test. bChi-square test. Y-BOCS, Yale^Brown Obsession^Compulsion Scale; CGI-I, Clinical Global Impression^
diagnoses (P40.05). No patient had comorbid tic
ence between treatment groups with respect to
treatment response (Po0.0001) (Table 1).
At the beginning of the 3-month period before the
The quetiapine doses received in group I were:
addition of quetiapine or placebo,the mean Y-BOCS
50 mg/day in three patients (21.5%); 75 mg/day in five
score for total patients in groups I and II was 28.475.2
patients (35.7%); 100 mg/day in four patients (28.6%);
whereas it was 23.974.6 at the end of this period,with
150 mg/day in one patient (7.1%) and 200 mg/day in
a mean Y-BOCS score of 24.174.9 in group I and
23.874.1 in group II (P40.05). The comparisons of
Nine of the patients (64.4%) in group I complained
Y-BOCS and Clinical Global Impression–Severity of
of side-effects. The most frequent side-effect was
Illness (CGI-SI) scores both at baseline and endpoint is
nausea (n ¼ 6),followed by sedation (n ¼ 3) and
summarized in Table 1. In addition,the mean Y-BOCS
dizziness (n ¼ 1). In group I,the mean weight gain
scores at each evaluation point are presented in Fig. 1.
from baseline to endpoint in the 8-week phase was
Of the group I patients,nine (64.3%) exhibited
significant improvement and one (7.1%) partial
Four of the patients (30.7%) in group II reported
improvement. In the patients with significant improve-
side-effects,including sedation (n ¼ 2),headache (n ¼ 1)
ment,the mean Y-BOCS score was 24.2(SD 5.3) and
and nervousness (n ¼ 1). The mean weight gain was
12.2 (SD 4.8) before and after the addition of
quetiapine,respectively. Of them,five were considered
No patient dropped out of the study in the 8-week
as very much improved and four much improved by
quetiapine or placebo addition phase.
CGI-I. In the patient with ‘partial’ improvement,themean Y-BOCS score was 22 and 14 before and afterquetiapine addition,respectively. This patient was
evaluated as much improved by CGI-I. None of thegroup II patients showed partial or significant im-
Our results reveal that quetiapine augmentation is
provement. There was a statistically significant differ-
effective and well-tolerated in the treatment of patientswith refractory OCD. Of the patients,71.4% (64.3%significant and 7.1% partial) demonstrated improve-ment. Antipsychotic drugs at low doses have been usedin the treatment of refractory OCD as adjunctivetreatment (McDougle et al.,1990). Therefore,atypicalantipsychotics such as clozapine,risperidone andolanzapine,have recently been tried in the patientswith refractory OCD. In a case reported by Younget al. (1994),the patient with primary OCD,unrespon-siveness to multiple drugs,ECT and psychosurgery,showed partial response to clozapine treatment. How-ever,it has been reported that patients with schizo-phrenia
obsessive–compulsive symptoms (Baker et al.,1992;
(Y-BOCS) Scores at 2, 4, 6 and 8 weeks in groups I and
Patil,1992; Patel and Tandon,1993). In addition,it
II. aP40.05, bP40.05, cPo0.05, dPo0.05.
has been reported that risperidone,when used alone,
International Clinical Psychopharmacology 2002,Vol 17 No 3
exacerbated obsessive and compulsive symptoms in the
In conclusion,the results of the present study
patient with comorbid bipolar disorder and OCD
suggest that quetiapine augmentation to a SRI may
(Remington and Adams,1994) or with comorbid OCD
be effective and well-tolerated in patients with treat-
and schizophrenia (Kopala and Honer,1994). When
ment resistant OCD. However,further double-blind
risperidone was combined with a SRI,the complaints
studies involving a large group of patients are needed.
considerably improved in the latter case. As can beseen,the descriptions of exacerbation in obsessive–compulsive symptoms occurred in patients with
primary psychotic disorder or comorbid OCD andpsychotic or bipolar disorder rather than primary
American Psychiatric Association (1994) Diagnostic and
OCD. Weiss et al. (1999) added olanzapine to SSRI in
Statistical Manual of Mental Disorders,4th edn. Wa-shington,DC: American Psychiatric Association Press.
10 patients with refractory OCD. Of these,70% of
Baker RW,Chengappa KNR,Baird JW,Steingard S,
patients (40% almost full responder) responded to this
Christ MA,Schooler NR (1992) Emergence of obsessive
treatment regimen. In another study performed by
compulsive symptoms during treatment with clozapine. J
Saxena et al. (1996),87% of the patients with SRI
refractory OCD showed clinically significant improve-
Bymaster FP,Calligaro DO,Falcone JF,Marsh RD,
ment after risperidone augmentation to SRI treatment.
binding profile of the atypical antipsychotic olanzapine.
McDougle et al. (2000) reported that 50% of patients
Goodman WK,Price LH,Rasmussen SA,Mazure C,
with refractory OCD who were given risperidone plus
Fleischmann RL,Hill CL,et al. (1989a) The Yale–
SRI,and none of the patients given placebo plus SRI,
Brown Obsessive Compulsive Scale I: development,useand reliability. Arch Gen Psychiatry 46:1006.
responded. In general,the response rate of our study is
Goodman WK,Price LH,Rasmussen SA,Delgado PL,
comparable with open-label studies (Saxena et al.,
Heninger GR,Charney D (1989b) Efficacy of fluvox-
1996; Weiss et al.,1999) but higher than double-blind
amine in obsessive-compulsive disorder: a double-blind
design studies (McDougle et al.,1994,2000). This
comparison with placebo. Arch Gen Psychiatry 46:36–43.
situation suggests that the study design itself may affect
obsessive-compulsive symptoms (OCS): a case report and
review of atypical antipsychotic induced OCS. J Psy-
We have only been able to identify one case report
regarding the relation between quetiapine and obses-
Kopala L,Honer WG (1994) Risperidone,serotonergic
sive–compulsive symptoms in the literature. Khullar et
mechanisms,and obsessive-compulsive symptoms in
al. (2001) reported quetiapine to exacerbate obsessive
schizophrenia (letter). Am J Psychiatry 151:1714–1715.
Leysen JE (1992) 5-HT2 receptors: location,pharmacolo-
and compulsive symptoms in a case who had OCD and
gical,pathological,and physiological role. In: Serotonin
comorbid delusional disorder. Quetiapine,similar to
Receptors: Pharmacologic Significance and Clinical Im-
risperidone,has strong antagonist effects on 5-HT1C
plication. (Lanser SZ,Brunello N,Racagni G,et al.,
2 receptors. Therefore,it might be expected
to increase obsessions and compulsions. However,the
courcelles D,Stoof JC,Janssen PAJ (1988) Biochemical
existence of a complex relationship between obsessive–
profile of risperidone,a new antipsychotic. J Pharmacol
compulsive symptoms and atypical antipsychotics has
been noted (Kopala and Honer,1994). Moreover,the
McDougle CJ,Goodman WK,Price LH,Delgado PL,
fact that atypical antipsychotics,including quetiapine
addition to an SRI,are effective in patients refractory
Neuroleptic addition in fluvoxamine-refractory obses-sive-compulsive disorder. Am J Psychiatry 147:652–654.
to a combination of SRI and typical neuroleptics might
McDougle CJ,Prive LH,Goodman WK,Charney DS,
be explained by their strong antagonistic effects on
many serotonin receptor subtypes (5-HT2A,5-HT2C,
augmentation in fluvoxamine-refractory obsessive com-
pulsive disorder: lack of efficacy. J Clin Psychopharmacol
1A,5-HT1D and 5-HT7). These receptors are down-
regulated by chronic SRI use and,consequently,the
McDougle CJ,Goodman WK,Leckman JF,Holzer JC,
blockade of serotonin receptors by atypical antipsycho-
tics,including quetiapine,can result in increased action
therapeutic effect of addition of buspirone in fluvox-
of an SRI (Leysen,1992; Richelson,1994).
amine-refractory obsessive-compulsive disorder. Am J
Several limitations should be taken into considera-
tion when interpreting our results. The main limitation
McDougle CJ,Goodman WK,Leckman JF,Lee NC,
Heninger GR,Price LH (1994) Haloperidol addition in
of our study was the single-blind design. In addition,
fluvoxamine-refractory obsessive compulsive disorder: a
because of the small sample size,our results could be
double-blind,placebo-controlled study in patients with
and without tics. Arch Gen Psychiatry 51:302–308.
118 International Clinical Psychopharmacology 2002,Vol 17 No 3
McDougle CJ,Epperson CN,Pelton GH,Wasylink S,
LH (2000) A double-blind,placebo-controlled
study of risperidone addition in serotonin reuptake
inhibitor-refractory obsessive compulsive disorder. Arch
Saxena S,Wang D,Bystritsky A,Baxter LRJ (1996)
Risperidone augmentation of SRI treatment for refrac-
tory obsessive-compulsive disorder. J Clin Psychiatry
compulsive symptoms during clozapine treatment (let-
Weiss EL,Potenza MN,McDougle CJ,Epperson CN
VJ (1992) Development of transient obsessive-
(1999) Olanzapine addition in obsessive-compulsive
compulsive symptoms during the treatment with cloza-
disorder refractory to selective serotonin reuptake
pine (letter). Am J Psychiatry 149:272.
inhibitors. J Clin Psychiatry 60:524–527.
Young CR,Bostic JQ,McDonald CL (1994) Clozapine
and refractory obsessive-compulsive disorder: a case
report (letter). J Clin Psychopharmacol 14:209–210.
Richelson E (1994) Preclinical pharmacology of antipsy-
chotic drugs: relationship to efficacy and side effects. JClin Psychiatry Monograph 12:13–17.
International Clinical Psychopharmacology 2002,Vol 17 No 3
• ABSTRACTS PRESENTED IN NATIONAL OR INTERNATIONAL MEETING AND WORKSHOPS 1- Mohsen I. Afouna, Ibrahim S. Khattab and Indra K. Reddy. Demeclocycline Liposomal Formulations: Preparation, Characterization and Assessment of their Intra-ocular Pressure Lowering Effects using rabbit model, The 9th International Pharmaceutical Sciences Meeting and Exposition, Dec. (2005). 2- Mohsen I. Afouna,
Sida 1 av 24 Jag skall nu försöka att berätta något fruktansvärt som hänt vår familj, vår äldsta dotter Jeanette har varit med om en trafikolycka i söndagskväll 2009-11-22, en lastbil körde på hennes bil i sidan och träffade rakt på förar dörren där Jeanette satt. Jeanette blev medvetslös vid kollisionen och hade ett stort sår i huvudet. Efter flera timmars väntan
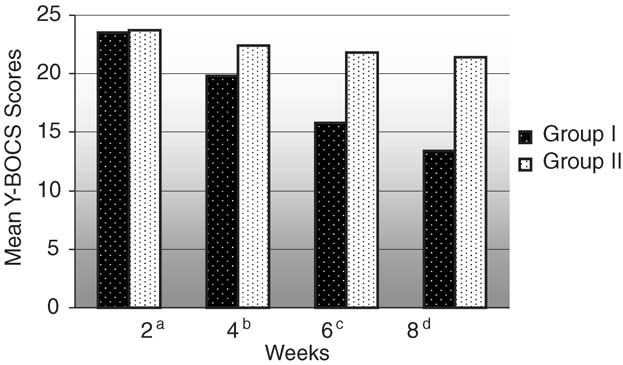 Table1. Comparison of scale scores (mean7SD) both at baseline and endpoint of the quetiapine or placebo addition phaseand that of responders at endpoint
aStudent’s t-test. bChi-square test. Y-BOCS, Yale^Brown Obsession^Compulsion Scale; CGI-I, Clinical Global Impression^
diagnoses (P40.05). No patient had comorbid tic
ence between treatment groups with respect to
treatment response (Po0.0001) (Table 1).
Table1. Comparison of scale scores (mean7SD) both at baseline and endpoint of the quetiapine or placebo addition phaseand that of responders at endpoint
aStudent’s t-test. bChi-square test. Y-BOCS, Yale^Brown Obsession^Compulsion Scale; CGI-I, Clinical Global Impression^
diagnoses (P40.05). No patient had comorbid tic
ence between treatment groups with respect to
treatment response (Po0.0001) (Table 1).