Thank you, it's cool. Used for the first time because only then was the right drug. Very revealing detail: ordered Express shipping to get the order within 3 hours because didn't know how to get the order faster https://africarx.co.za/buy-levitra-south-africa.html The drug is authentic exactly. Consistent with the stated prices the Staff is knowledgeable.
Doi:10.1016/j.expneurol.2004.11.013
Experimental Neurology 192 (2005) 73 – 78
Continuous dopaminergic stimulation reduces risk of motor complications
Francesco Bibbiania, Lauren C. Costantinib, Raj Patelb, Thomas N. Chasea,*
aExperimental Therapeutic Branch, Building 10, Room 5C103, National Institute of Neurological Disorders and Stroke, NIH, Bethesda, MD 20892-1406, USA
bTitan Pharmaceuticals, Inc., South San Francisco, CA, USA
Received 12 August 2004; revised 5 November 2004; accepted 10 November 2004
Levodopa or short-acting dopamine (DA) agonist treatment of advanced parkinsonian patients exposes striatal DA receptors to non-
physiologic intermittent stimulation that contributes to the development of dyskinesias and other motor complications. To determine whethercontinuous dopaminergic stimulation can delay or prevent onset of motor complications, four MPTP-lesioned, levodopa-naive cynomolgusmonkeys were implanted subcutaneously with apomorphine containing ethylene vinyl acetate rods. Three other MPTP-lesioned monkeysreceived daily injections of apomorphine. Animals receiving apomorphine rods showed improved motor function (dONT state) within 1 day ofimplantation, and remained continually dONT for the duration of treatment (up to 6 months) without developing dyskinesias. Injected animalsalso showed similar improvement in motor function after each apomorphine injection. However, these primates remained dONT for only 90min and within 7–10 days all developed severe dyskinesias. Implanted monkeys evidenced local irritation, which was alleviated by steroidco-therapy. D 2004 Elsevier Inc. All rights reserved.
Keywords: Dopamine; Parkinson’s disease; Dyskinesia; Striatum; Nigra; Implant; Polymeric; Subcutaneous; Apomorphine; Ethylene-vinyl Acetate
parkinsonian monkeys, dyskinesias begin within 1–2 weeksof daily dopaminomimetic therapy (but
Alterations in the motor response to standard dopami-
do not appear when treated via continuous infusion for 27
nergic therapy constitute a major source of disability in
patients with later stage Parkinson’s disease (PD) (
in parkinsonian primates given levodopa (90 min half-life)
and Muenter, 2001; Martignoni et al., 2003; Miyawaki et
than in those treated with DA agonists (with half-lives
al., 1997). Increasing evidence suggests that the intermittent
exceeding 4 h) that provide relatively more constant
stimulation of striatal dopamine (DA) receptors contributes
dopaminergic stimulation (Similarly, motor
to the pathogenesis of these progressive complications
complications tend to subside in PD patients when
intermittent dopaminergic therapy is replaced by more
2000a,b; Olanow et al., 2000). In parkinsonian rats, 3
weeks of twice-daily levodopa alters motor responses in
Hadj Tahar et al., 2000; Mouradian et al., 1990). These
ways that mimic human motor fluctuations; these responses
observations suggest that the risk of motor response
do not occur if levodopa is administered by round-the-clock
complications may be reduced by therapeutic regimens that
provide steady and thus more physiologic DA replacementfor this normally tonically operating system (1989; Skirboll et al., 1990).
The only currently available means to constantly
* Corresponding author. Fax: +1 301 496 6609. E-mail address: TChase@ninds.nih.gov (T.N. Chase).
administer dopaminergic agents, by continuous infusion
0014-4886/$ - see front matter D 2004 Elsevier Inc. All rights reserved. doi:10.1016/j.expneurol.2004.11.013
F. Bibbiani et al. / Experimental Neurology 192 (2005) 73–78
has limited practicality. Recently, an ethylene vinyl acetate
period of 3 h and were performed separately from those in the
(EVA) copolymer system has been developed that enables
EVA implanted animals. The continuously infused monkeys
the continuous release of drugs at therapeutic levels over
were scored once daily. Parkinsonian severity was scored on
were assessed on an Abnormal Involuntary Movement Scale
effective DA agonist for the relief of parkinsonian symp-
choreiform and dystonic dyskinesias independently: occa-
Wenning, 2000; Wenning et al., 1999), these implants have
sional or mild = 1; intermittent or moderate = 2; continuous or
performed safely and reliably upon subcutaneous placement
severe = 3. Safety monitoring (for skin irritation) was
in pigs (IDB, Titan Pharmaceuticals). Here, we evaluated
performed by a different rater who was not blind to treatment.
the hypothesis that the long-term continuous administrationof apomorphine will maintain antiparkinsonian efficacy but
not induce dyskinesias in previously untreated MPTPlesioned primates. In addition, the safety and tolerability
Apomorphine hydrochloride (Sigma, St Louis, MO) was
of these apomorphine-containing EVA rods administered by
used for both injection and implantation therapy. Dexame-
themselves and with steroid co-therapy was assessed in this
thasone (Sigma) (0.5 mg/kg i.m.) and Triamcinolone
acetonide (Kenacort A, Bristol-Myers Squibb, Anagni,Italy) (0.5 mg s.c. per injection site) were used for theprophylaxis of cutaneous inflammation.
Non-erodible EVA rods capable of prolonged zero order
Studies were conducted in accordance with the NIH
Guide for the Care and Use of Laboratory Animals in 7
Pharmaceuticals, Inc., South San Francisco, CA) were 26
adult male cynomolgus (Macaca fascicularis) primates
mm long and 2.4 mm in diameter; each contained
weighing 6.5–7.3 kg. All were housed individually, under
approximately 98 mg of apomorphine. Animals were
stable room conditions, with a 12-h light/dark cycle. Each
sedated with 0.3 ml ketamine and a small incision (0.5
received a standard biscuit diet twice daily supplemented
cm) was made between the shoulder blades. Implants were
with fruit and had free access to water. All primates were
positioned between the scapulae by means of a trocar, and a
rendered parkinsonian by the subcutaneous administration
stylet was used to slide the rod from the trocar into the
of 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP)
subcutaneous tissue. This technique allows rod placement
HCl (Research Biochemicals Intl., Natick, MA) once per
through a minimal incision. The first two implanted animals
week at 0.5–1 mg/kg until definite parkinsonian features,
received rods that were pre-washed for 8 h with saline prior
including tremor, appeared (scores of 4–5 points on the
to sterilization, while the third and fourth implanted animals
Laval Disability Scale, where the normal state extends from
received rods that had been pre-washed for 30 min with
0 to 2 points and maximum disability is 10 points) (
ethanol prior to sterilization to minimize any initial burst
et al., 2001). The average cumulative MPTP dose was 4.3
drug release. The implantation procedure took approxi-
mg/kg (range 2.5–7.5). Following observation for two
mately 15 min and produced no complications.
additional months to ensure stable disability, animals wereselected for equivalent parkinsonian severity (disability
score of 4.5–5 points). These animals, not previouslyexposed to dopaminergic agents, were randomly divided
Post-implant plasma apomorphine concentrations were
into two groups: the first (n = 3) received daily subcuta-
measured at hours 6, 12, 24, 36, 48, then daily until day 7,
neous injections of apomorphine (2 mg/kg, the minimally
weekly until week 4, and monthly for the remainder of study
effective dose to turn animals dONT, that is, reverse all
(6 months). Plasma apomorphine levels were determined by
parkinsonian signs) at rotating sites for 14 days (
extraction into an organic solvent (liquid–liquid extraction)
al., 2003); each primate in the second group (n = 4) was
followed by HPLC separation and MS/MS identification and
treated by implantation of three apomorphine-containing
quantification. Plasma samples were diluted with acetonitrile
containing a known amount of an internal standard (nor-apomorphine), extracted with hexane, and the solvent
evaporated. The resulting residue was reconstituted in 100AL water/acetonitrile (90:10) and injected onto an HPLC
All behavioral ratings were performed by the same blinded
column. The individual components were separated and
investigator. Evaluations in animals receiving daily injections
analyzed by MS/MS both for identity and amount by
(apomorphine or placebo) occurred every 30 min over a
comparison to the internal standard. Upon explantation, the
F. Bibbiani et al. / Experimental Neurology 192 (2005) 73–78
residual apomorphine content in each rod was determined by
injection was clinically similar (Laval scores: 0–1). How-
ever, within 7–10 days (mean 8.3 days), all animals treatedby daily apomorphine injection developed dyskinesias
(range 6–10 on the Involuntary Movement Scale). Incontrast, animals receiving apomorphine implants remained
Sections of skin surrounding the implant site were fixed
dONT for up to 6 months and never developed dyskinesias
in 10% formalin, embedded in paraffin, sectioned at 5-Am
(Once the EVA rods were removed, all animals were
intervals, and stained with hematoxylin and eosin.
dOFFT and oral levodopa therapy was initiated.
Plasma apomorphine concentrations were measured
periodically in all primates (Apomorphine levelsimmediately after implantation in animals receiving saline-
The primary outcome measure of this study was the
washed rods were initially high (Cmax of 10 and 27 ng/ml),
appearance of dyskinesias. This essentially ball-or-nothingQ
but declined to their ultimate steady state levels within a
phenomenon, taken together with the limited sample size
week. One of the monkeys receiving saline-washed implants
precluded formal statistical analysis.
showed signs of excessive dopaminergic stimulation (vom-iting, prostration) for 2 days following rod insertion, whichresolved as drug levels reached steady state. Use of ethanol-
washed rods in the remaining two monkeys, eliminated thisinitial burst release. Except as noted, apomorphine levels
All MPTP-lesioned monkeys given apomorphine by
remained stable in all rod-implanted animals throughout the
subcutaneously implanted rods showed essentially total
entire period with very little variability (0.66 F 0.08 ng/ml
remission of parkinsonian signs (fully dONT) within 6–12
at steady state). During this time, the release rate of
h after implantation, and continued to evidence stable motor
apomorphine from the implanted rods, calculated from the
benefit until explantation after 11 (first animal), 22 (second
drug remaining in the rod upon explantation, was approx-
animal) and 24 weeks (third and fourth animal) with no
imately 0.25 mg/day/rod. In animals receiving apomorphine
fluctuations in response (constant Disability Scale scores of
injections, plasma drug levels rose after 20 min to
0–1). Animals treated once daily by apomorphine injection
approximately 27 ng/ml, and declined to about 5 ng/ml by
(2.0 mg/kg) also turned fully dONT beginning immediately
80–90 min post-injection (at which point the animals had
after injection and lasting up to about 90 min. The dONT
returned to the dOFFT state). Plasma levels required to
state induced by apomorphine administered by rod or by
maintain the dONT state in implanted animals (0.19–1.1 ng/
Fig. 1. Dyskinesia scores in animals receiving daily apomorphine injections (2 mg/kg, s.c., open circles) versus apomorphine implants (filled squares). After amean of 8.3 days of daily apomorphine injections, all animals developed dyskinesias (range 6–10 on the Involuntary Movement Scale), whereas none of theimplanted animals developed dyskinesias over 6 months of study.
F. Bibbiani et al. / Experimental Neurology 192 (2005) 73–78
Fig. 2. Plasma drug concentration in animals receiving daily apomorphine injections (2 mg/kg s.c., open circles) versus apomorphine implants (filled squares). Peaks and troughs are observed with daily injections: plasma levels in animals receiving apomorphine injections peaked after 20 min at approximately 27 ng/ml,then declined to about 5 ng/ml by 80–90 min post-injection (at which point they returned to the dOFFT state). In all implanted animals, apomorphine levelsevidenced very little variability (0.66 F 0.08 ng/ml at steady state). Plasma levels required to maintain the dONT state in implanted animals (0.19–1.1 ng/ml) weresignificantly lower than those required in injected animals (5.0 ng/ml).
ml) were substantially lower than those required in injected
apomorphine concentrations required for optimal motor
improvement in the injected animals were an order of
Local irritation was observed clinically in the first 2
magnitude higher than those required in the rod implanted
implanted primates. The first implanted monkey manifested
primates. Conceivably, higher agonist levels may be
signs of irritation within 2 days that continued until
required with intermittent stimulation to prolong the time
explantation at 11 weeks. Histological examination of the
DA receptors are exposed to suprathreshold stimulation. It is
implant sites revealed a dermal zone of necrosis surrounded
also possible that that postsynaptic DA receptors in a system
by viable and degenerated neutrophils, macrophages, multi-
that normally functions tonically, respond more efficiently
nucleate giant cells, and plasma cells. The second implanted
to stable physiologic-range stimulation than to intermittent
animal was pretreated systemically with dexamethasone (0.5
pulsatile activation, possibly owing to restore changes
mg/kg i.m.) 1 day before implantation, on the day of
occurring within or downstream from striatal dopaminocep-
implantation, and 2, 4, and 6 days thereafter. This primate
showed no irritation until 22 weeks when the implants were
The present results further suggest that the continuous
removed. The third and fourth implanted animals were also
administration of dopaminomimetics, at doses sufficient to
pretreated systemically with dexamethasone and, in addi-
ameliorate parkinsonian signs can substantially reduce the
tion, received local triamcinolone acetonide (0.5 mg
risk of inducing dyskinesias. All apomorphine-injected
injection s.c. per implant site) at 2, 4, and 6 months after
primates developed dyskinesias within 1–2 weeks of treat-
insertion. No clinical signs of irritation were evident in these
ment initiation, consistent with the findings of earlier
animals that were explanted at 6 months, as per protocol.
investigations in which DA agonists were intermittently
Microscopic examination, however, revealed a mild inflam-
matory response immediately surrounding each implant.
2003; Smith et al., 2003). In contrast, no apomorphine
There were no systemic adverse reactions to the implants or
implanted animal developed dyskinesias over treatment
to the anti-inflammatory treatments.
intervals lasting up to 6 months. Previous studies ofcontinuous dopaminergic administration in rodent andprimate models of PD (
1994) showed protective results for up to 4 weeks. Since noother therapeutic regimen has been reported capable of
Results from this study indicate that subcutaneous
maintaining a similar degree of dyskinesia-free antiparkin-
implanted EVA rods can stably release apomorphine for
sonian efficacy over such an extended period, findings from
up to 6 months, allowing continuous dONT time in MPTP-
this study provide additional evidence in support of the
lesioned primates without the appearance of dyskinesias.
hypothesis that the intermittent and thus, non-physiologic
Apomorphine injections produced equivalent, although
stimulation of striatal dopaminergic receptors contributes to
transient improvement in parkinsonian signs, but lead to
the onset of dyskinesias and related motor response
the development of dyskinesias within 7–10 days. Plasma
complications (The nonphysiologic stimula-
F. Bibbiani et al. / Experimental Neurology 192 (2005) 73–78
tion of dopamine receptors on medium-sized spiny neurons,
Baronti, F., Mouradian, M.M., Davis, T.L., Giuffra, M., Brughitta, G.,
first due to the progressive denervation caused by nigro-
Conant, K.E., Chase, T.N., 1992. Continuous lisuride effects on centraldopaminergic mechanisms in Parkinson’s disease. Ann. Neurol. 6,
striatal system degeneration and subsequently due to the
intermittent high-intensity stimulation associated with dop-
Bezard, E., Brotchie, J.M., Gross, C.E., 2001. Pathophysiology of
aminomimetic treatment, has been shown to activate
levodopa-induced dyskinesia: potential for new therapies. Nat. Rev.,
signaling cascades that regulate the phosphorylation state
of coexpressed ionotropic glutamatergic receptor subunits
Bibbiani, F., Oh, J.D., Chase, T.N., 2001. Serotonin 5-HT1A agonist
improves motor complications in rodent and primate parkinsonian
models. Neurology 10, 1829 – 1834.
receptor sensitization modifies cortical excitatory input to
Bibbiani, F., Oh, J.D., Petzer, J.P., Castagnoli, N., Chen, J-F., Schwarzchild,
these spiny efferent neurons, thus altering striatal output in
M.A., Chase, T.N., 2003. A2A antagonist prevents dopamine agonist-
induced motor complications in animal models of PD. Exp. Neurol. 1,
Bravi, D., Mouradian, M.M., Roberts, J.W., Davis, T.L., Sohn, Y.H., Chase,
EVA rods of the type used here produced no clinical or
T.N., 1994. Wearing-off fluctuations in Parkinson’s disease: contribu-
histological evidence of tissue reaction in animals or in
tion of postsynaptic mechanisms. Ann. Neurol. 1, 27 – 31.
patients when loaded with various other drugs (
Chase, T.N., 2004. Striatal plasticity and extrapyramidal motor dysfunction.
2003). The adverse tissue response observed in two of the
Parkinsonism Relat. Disord. 5, 305 – 313 (Review).
apomorphine implanted animals thus appears attributable to
Chase, T.N., Oh, J.D., 2000a. Striatal mechanisms and pathogenesis of
parkinsonian signs and motor complications. Ann. Neurol. 4,
apomorphine itself rather than to the polymeric matrix.
Apomorphine is known to induce cutaneous nodules when
Chase, T.N., Oh, J.D., 2000b. Striatal dopamine- and glutamate-mediated
dysregulation in experimental parkinsonism. Trends Neurosci. 10,
1995; Ostergaard et al., 1995). On the other hand, steroidal
co-therapy at doses low enough to preclude systemic effects
Chase, T.N., Baronti, F., Fabbrini, G., Heuser, I.J., Juncos, J.L., Mouradian,
M.M., 1989. Rationale for continuous dopaminomimetic therapy of
appeared to largely suppress this reaction. In the two
Parkinson’s disease. Review. Neurology 39 (Suppl. 2), 7 – 10.
primates receiving both local and systemically administered
Dewey Jr., R.B., Maraganore, D.M., Ahlskog, J.E., Matsumoto, J.Y., 1996.
steroid co-therapy, the apomorphine was well tolerated for
Intranasal apomorphine rescue therapy for parkinsonian boffQ periods.
up to 5–6 months. Histological examination of tissues from
Clin. Neuropharmacol. 3, 193 – 201.
both these animals showed inflammation similar in charac-
Hadj Tahar, A., Gregoire, L., Bangassoro, E., Bedard, P.J., 2000. Sustained
cabergoline treatment reverses levodopa-induced dyskinesias in parkin-
ter but considerably diminished in severity compared to that
sonian monkeys. Clin. Neuropharmacol. 4, 195 – 202.
observed in the two animals that received no or only
Jenner, P, 2000. Pathophysiology and biochemistry of dyskinesia: clues for
systemic steroids and manifested signs of local irritation.
the development of non-dopaminergic treatments. J. Neurol. 247,
Thus, the combination of systemically administered dex-
amethasone at the time of implantation and locally injected
Juncos, J.L., Engber, T.M., Raisman, R., Susel, Z., Thibaut, F., Ploska, A.,
Agid, Y., Chase, T.N., 1989. Continuous and intermittent levodopa
triamcinolone every 2 months thereafter appears capable of
differentially affect basal ganglia function. Ann. Neurol. 5, 473 – 478.
preventing a clinically significant tissue reaction.
Langer, R., Folkman, J., 1976. Polymers for the sustained release of
The continuous delivery of dopaminergic agents to the
proteins and other macromolecules. Nature 263, 797 – 800.
human striatum remains a major challenge for the treatment
Lesser, G.J., Grossman, S.A., Leong, K.W., Lo, H., Eller, S., 1996. In vitro
of patients with PD. None of the previously utilized
and in vivo studies of subcutaneous hydromorphone implants designedfor the treatment of cancer pain. Pain 2–3, 265 – 272.
cutaneous, intravenous, intranasal, sublingual, duodenal, or
LeWitt, P.A., 2004. Subcutaneously administered apomorphine: pharma-
rectal routes of administration have documented long-term
cokinetics and metabolism. Neurology 62 (Suppl. 4), S8 – S11.
success due to inconvenience, adverse effects, or limited
Manson, A.J., Hanagasi, H., Turner, K., Patsalos, P.N., Carey, P.,
Ratnaraj, N., Lees, A.J., 2001. Intravenous apomorphine therapy in
and van Laar, 1999; Pollak et al., 1993). Apomorphine is an
Parkinson’s disease: clinical and pharmacokinetic observations. Brain124, 331 – 340.
attractive candidate for use in continuous administration
Manson, A.J., Turner, K., Lees, A.J., 2002. Apomorphine monotherapy in
paradigms to parkinsonian patients due to its proven
the treatment of refractory motor complications of Parkinson’s disease.
efficacy, high potency, solubility, and comparatively well-
Investigator’s Drug Brochure, Mov. Disord. vol. 6. Titan Pharmaceu-
balanced D1 and D2 DA receptor agonist properties
Martignoni, E., Riboldazzi, G., Calandrella, D., 2003. Riva N. motor
complications of Parkinson’s disease. Neurol. Sci. 24, S27 – S29.
the one used in this study may constitute an important
Miyawaki, E., Lyons, K., Pahwa, R., Troster, A.I., Hubble, J., Smith, D.,
advance in our ability to constantly deliver dopaminergic
Busenbark, K., McGuire, D., Michalek, D., Koller, W.C., 1997. Motor
agents to PD patients and thus warrant further evaluation.
complications of chronic levodopa therapy in Parkinson’s disease. Clin. Neuropharmacol. 6, 523 – 530.
Montastruc, J.L., Rascol, O., Senard, J.M., Houin, G., Rascol, A., 1995.
Sublingual apomorphine: a new pharmacological approach in Parkin-son’s disease? J. Neural Transm., Suppl. 45, 157 – 161.
Ahlskog, J.E., Muenter, M.D., 2001. Frequency of levodopa-related
Morissette, M., Goulet, M., Soghomonian, J.J., Blanchet, P.J., Calon, F.,
dyskinesias and motor fluctuations as estimated from the cumulative
Bedard, P.J., Di Paolo, T., 1997. Preproenkephalin mRNA expression in
literature. Mov. Disord. 3, 448 – 458.
the caudate-putamen of MPTP primates after chronic treatment with the
F. Bibbiani et al. / Experimental Neurology 192 (2005) 73–78
D2 agonist U91356A in continuous or intermittent mode of admin-
Poewe, W., Wenning, G.K., 2000. Apomorphine: an underutilized therapy
istration: comparison with L-DOPA therapy. Brain Res. Mol. Brain Res.
for Parkinson’s disease. Mov. Disord. 5, 789 – 794.
Pollak, P., Benabid, A.L., Limousin, P., Gervason, C.L., Jeanneau-Nicolle,
Mouradian, M.M., Heuser, I.J., Baronti, F., Chase, T.N., 1990. Modification
E., 1993. External and implanted pumps for apomorphine infusion in
of central dopaminergic mechanisms by continuous levodopa therapy
parkinsonism. Acta Neurochir., Suppl. 58, 48 – 52.
for advanced Parkinson’s disease. Ann. Neurol. 1, 18 – 23.
Raasch, W., Slotty, C., Dominiak, P., 2000. In vitro and in vivo long term
Muguet, D., Broussolle, E., Chazot, G., 1995. Apomorphine in patients
release of apomorphine from polymer matrices. Jpn. J. Pharmacol. 1,
with Parkinson’s disease. Biomed. Pharmacother. 4, 197 – 209.
Neef, C., van Laar, T., 1999. Pharmacokinetic–pharmacodynamic relation-
Skirboll, S., Wang, J., Mefford, I., Hsiao, J., Bankiewicz, K.S., 1990. In
ships of apomorphine in patients with Parkinson’s disease. Clin.
vivo changes of catecholamines in hemiparkinsonian monkeys meas-
ured by microdialysis. Exp. Neurol. 2, 187 – 193.
Olanow, W., Schapira, A.H., Rascol, O., 2000. Continuous dopamine-
Smith, L.A., Jackson, M.J., Hansard, M.J., Maratos, E., Jenner, P., 2003.
receptor stimulation in early Parkinson’s disease. Trends Neurosci. 23,
Effect of pulsatile administration of levodopa on dyskinesia induction in
drug-naive MPTP-treated common marmosets: effect of dose, frequency
Ostergaard, L., Werdelin, L., Odin, P., Lindvall, O., Dupont, E.,
of administration, and brain exposure. Mov. Disord. 5, 487 – 495.
Christensen, P.B., Boisen, E., Jensen, N.B., Ingwersen, S.H., Schmie-
Wenning, G.K., Bosch, S., Luginger, E., Wagner, M., Poewe, W., 1999.
gelow, M., 1995. Pen injected apomorphine against off phenomena
Effects of long-term, continuous subcutaneous apomorphine infusions
in late Parkinson’s disease: a double blind, placebo controlled study.
on motor complications in advanced Parkinson’s disease. Adv. Neurol.
J. Neurol. Neurosurg. Psychiatry 6, 681 – 687.
Papa, S.M., Engber, T.M., Kask, A.M., Chase, T.N., 1994. Motor
White, J., 2003. Probuphine for the Treatment of Opiate Addiction—
fluctuations in levodopa treated parkinsonian rats: relation to lesion
Preliminary Results. International Society of Addiction Medicine
extent and treatment duration. Brain Res. 662, 69 – 74.
Patient information from the BMJ Group Stomach ulcers If the lining of your stomach or bowels gets damaged, it can cause an ulcer. Stomach ulcers are sometimes called peptic ulcers. They can be very painful, but there are treatments that can help. We've brought together the best and most up-to-date research about stomach ulcers to see what treatments work. You can use our information t
 Experimental Neurology 192 (2005) 73 – 78
Continuous dopaminergic stimulation reduces risk of motor complications
Francesco Bibbiania, Lauren C. Costantinib, Raj Patelb, Thomas N. Chasea,*
aExperimental Therapeutic Branch, Building 10, Room 5C103, National Institute of Neurological Disorders and Stroke, NIH, Bethesda, MD 20892-1406, USA
bTitan Pharmaceuticals, Inc., South San Francisco, CA, USA
Received 12 August 2004; revised 5 November 2004; accepted 10 November 2004
Levodopa or short-acting dopamine (DA) agonist treatment of advanced parkinsonian patients exposes striatal DA receptors to non-
physiologic intermittent stimulation that contributes to the development of dyskinesias and other motor complications. To determine whethercontinuous dopaminergic stimulation can delay or prevent onset of motor complications, four MPTP-lesioned, levodopa-naive cynomolgusmonkeys were implanted subcutaneously with apomorphine containing ethylene vinyl acetate rods. Three other MPTP-lesioned monkeysreceived daily injections of apomorphine. Animals receiving apomorphine rods showed improved motor function (dONT state) within 1 day ofimplantation, and remained continually dONT for the duration of treatment (up to 6 months) without developing dyskinesias. Injected animalsalso showed similar improvement in motor function after each apomorphine injection. However, these primates remained dONT for only 90min and within 7–10 days all developed severe dyskinesias. Implanted monkeys evidenced local irritation, which was alleviated by steroidco-therapy.
Experimental Neurology 192 (2005) 73 – 78
Continuous dopaminergic stimulation reduces risk of motor complications
Francesco Bibbiania, Lauren C. Costantinib, Raj Patelb, Thomas N. Chasea,*
aExperimental Therapeutic Branch, Building 10, Room 5C103, National Institute of Neurological Disorders and Stroke, NIH, Bethesda, MD 20892-1406, USA
bTitan Pharmaceuticals, Inc., South San Francisco, CA, USA
Received 12 August 2004; revised 5 November 2004; accepted 10 November 2004
Levodopa or short-acting dopamine (DA) agonist treatment of advanced parkinsonian patients exposes striatal DA receptors to non-
physiologic intermittent stimulation that contributes to the development of dyskinesias and other motor complications. To determine whethercontinuous dopaminergic stimulation can delay or prevent onset of motor complications, four MPTP-lesioned, levodopa-naive cynomolgusmonkeys were implanted subcutaneously with apomorphine containing ethylene vinyl acetate rods. Three other MPTP-lesioned monkeysreceived daily injections of apomorphine. Animals receiving apomorphine rods showed improved motor function (dONT state) within 1 day ofimplantation, and remained continually dONT for the duration of treatment (up to 6 months) without developing dyskinesias. Injected animalsalso showed similar improvement in motor function after each apomorphine injection. However, these primates remained dONT for only 90min and within 7–10 days all developed severe dyskinesias. Implanted monkeys evidenced local irritation, which was alleviated by steroidco-therapy.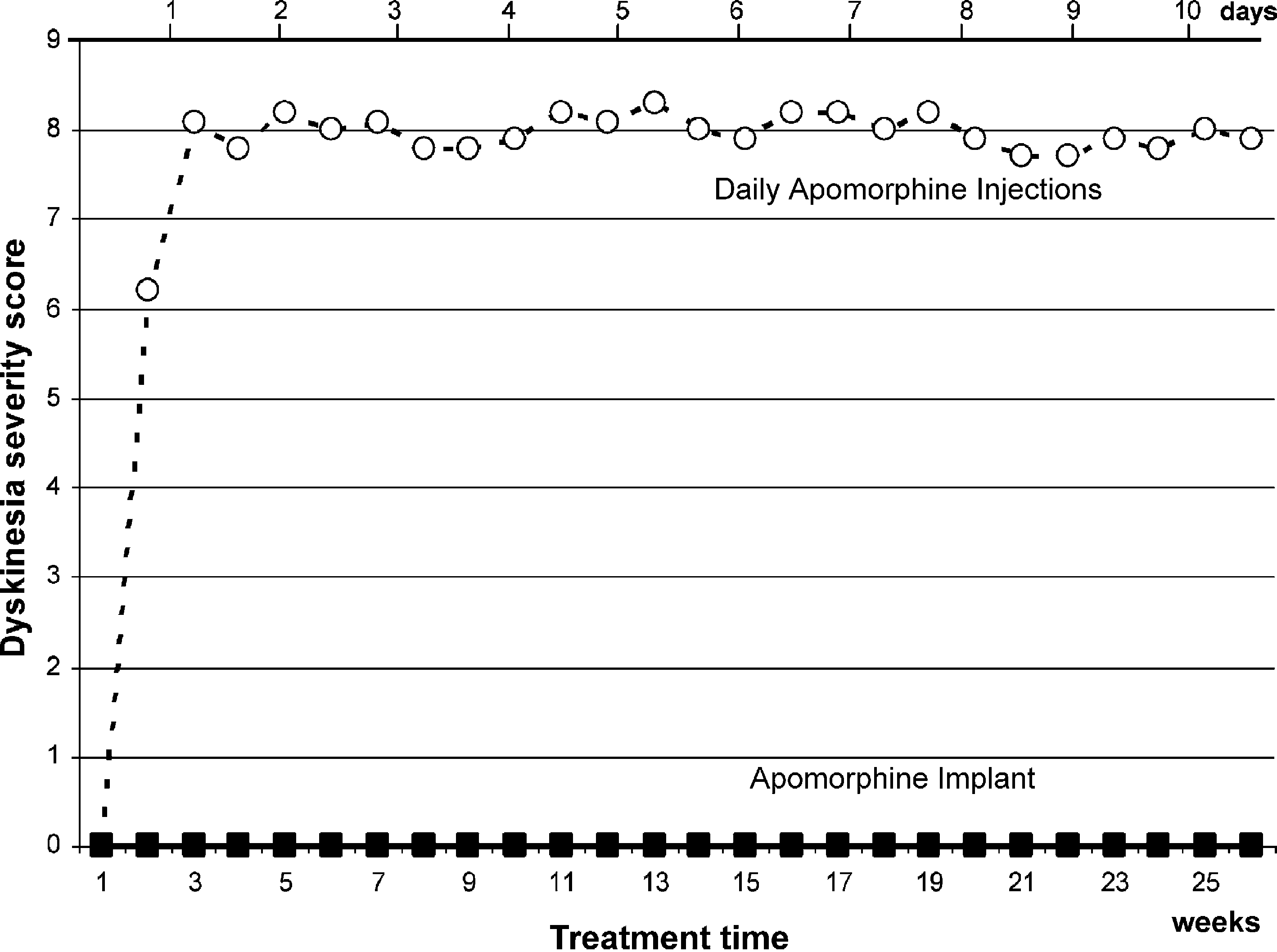 F. Bibbiani et al. / Experimental Neurology 192 (2005) 73–78
residual apomorphine content in each rod was determined by
injection was clinically similar (Laval scores: 0–1). How-
ever, within 7–10 days (mean 8.3 days), all animals treatedby daily apomorphine injection developed dyskinesias
(range 6–10 on the Involuntary Movement Scale). Incontrast, animals receiving apomorphine implants remained
Sections of skin surrounding the implant site were fixed
dONT for up to 6 months and never developed dyskinesias
in 10% formalin, embedded in paraffin, sectioned at 5-Am
(Once the EVA rods were removed, all animals were
intervals, and stained with hematoxylin and eosin.
F. Bibbiani et al. / Experimental Neurology 192 (2005) 73–78
residual apomorphine content in each rod was determined by
injection was clinically similar (Laval scores: 0–1). How-
ever, within 7–10 days (mean 8.3 days), all animals treatedby daily apomorphine injection developed dyskinesias
(range 6–10 on the Involuntary Movement Scale). Incontrast, animals receiving apomorphine implants remained
Sections of skin surrounding the implant site were fixed
dONT for up to 6 months and never developed dyskinesias
in 10% formalin, embedded in paraffin, sectioned at 5-Am
(Once the EVA rods were removed, all animals were
intervals, and stained with hematoxylin and eosin.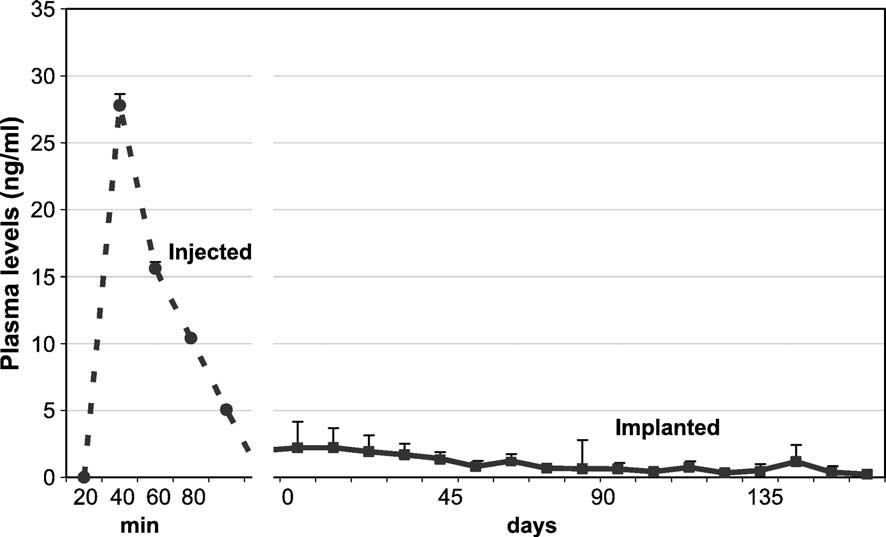 F. Bibbiani et al. / Experimental Neurology 192 (2005) 73–78
Fig. 2. Plasma drug concentration in animals receiving daily apomorphine injections (2 mg/kg s.c., open circles) versus apomorphine implants (filled squares).
F. Bibbiani et al. / Experimental Neurology 192 (2005) 73–78
Fig. 2. Plasma drug concentration in animals receiving daily apomorphine injections (2 mg/kg s.c., open circles) versus apomorphine implants (filled squares).