Thank you, it's cool. Used for the first time because only then was the right drug. Very revealing detail: ordered Express shipping to get the order within 3 hours because didn't know how to get the order faster https://africarx.co.za/ The drug is authentic exactly. Consistent with the stated prices the Staff is knowledgeable.
Pii: s0015-0282(02)04574-0
FERTILITY AND STERILITY
Copyright 2003 American Society for Reproductive Medicine
Printed on acid-free paper in U.S.A. Coordination of early antral follicles by luteal estradiol administration provides a basis for alternative controlled ovarian hyperstimulation regimens Renato Fanchin, M.D.,a Joa˜o Sabino Cunha-Filho, M.D.,a Luca Maria Schona¨uer, M.D.,aIsaac Jacques Kadoch, M.D.,a Paul Cohen-Bacri, M.D.,b and Rene´ Frydman, M.D.a
Hoˆpital Antoine Be´cle`re, Clamart, and Laboratoire d’Eylau, Paris, FranceObjective: To investigate whether luteal E administration reduces size discrepancies of early antral follicles. Design: Prospective, crossover study. Setting: ART unit, Clamart, France. Patient(s): Sixty women and 120 cycles. Intervention(s): On cycle day 3 (baseline day 3), all women underwent measurements of early antral follicles by ultrasound and serum FSH and ovarian hormones. From day 20 until the next cycle day 2, 30 of them received oral 17-E , whereas the remaining women served as controls. The day after E discontinuation (E
day 3) or on subsequent cycle day 3 (control day 3), participants were reevaluated as on baseline day 3. Main Outcome Measure(s): Magnitude of follicular size discrepancies. Result(s): Follicular size discrepancies and follicular diameters were significantly attenuated on E day 3 (3.7
Ϯ 0.5 mm) as compared with baseline day 3 (4.9 Ϯ 1.0 mm), but not in controls (5.0 Ϯ 0.8 vs. 4.9 Ϯ 0.8 mm). FSH (4.3 Ϯ 1.9 vs. 7.3 Ϯ 3.3 mIU/mL) and inhibin B (34 Ϯ 28 vs. 71 Ϯ 32 pg/mL) levels were consistentlylower on E day 3 than on baseline day 3 but remained unchanged in controls. Conclusion(s): Luteal E administration reduces the size and improves the homogeneity of early antral
follicles on day 3. This approach may be instrumental in synchronizing follicular development duringcontrolled ovarian hyperstimulation. (Fertil Steril 2003;79:316 –21. 2003 by American Society for Repro-ductive Medicine.)
Key Words: FSH, estradiol, early antral follicles, controlled ovarian hyperstimulation
The foremost objective of controlled ovar-
dissimilar sizes, which range from 2 to 8 mm in
ian hyperstimulation (COH) is to ensure the
adequate functional and morphologic matura-
both of these interrelated phenomena may be
tion of early antral follicles to increase the
instrumental in the establishment of the follic-
Fanchin, M.D., Departmentof Obstetrics and
number of viable oocytes and the probability of
ular dominance. Indeed, although it is conceiv-
conception. One of the key points of such a
able that complex intrafollicular mechanisms
procedure is the achievement of adequate syn-
concur to determine follicular sensitivity to
Hoˆpital Antoine Be´cle`re,157 Rue de la Porte de
chronization of follicular growth so that ovu-
lation can be triggered when most follicles
larger follicles are more responsive to this hor-
have reached concomitant maturation. How-
4980; E-mail: renato. fanchin@abc.ap-hop-
ever, to attain satisfactory follicular coordina-
mechanisms underlying the heterogeneity of
tion during COH, the physiological heteroge-
early antral follicles sizes during the early fol-
neity of selectable follicles observed during the
early follicular phase should probably be over-
A possible explanation for this phenomenon
involves the exposure of early antral follicles to
During the first days of the follicular phase
gradient FSH levels during the late luteal
in the menstrual cycle, early antral follicles are
phase. During the ultimate phase of the men-
0015-0282/03/$30.00PII S0015-0282(02)04574-0
discrepantly sensitive to FSH and exhibit
strual cycle, up to 5 days before the onset of
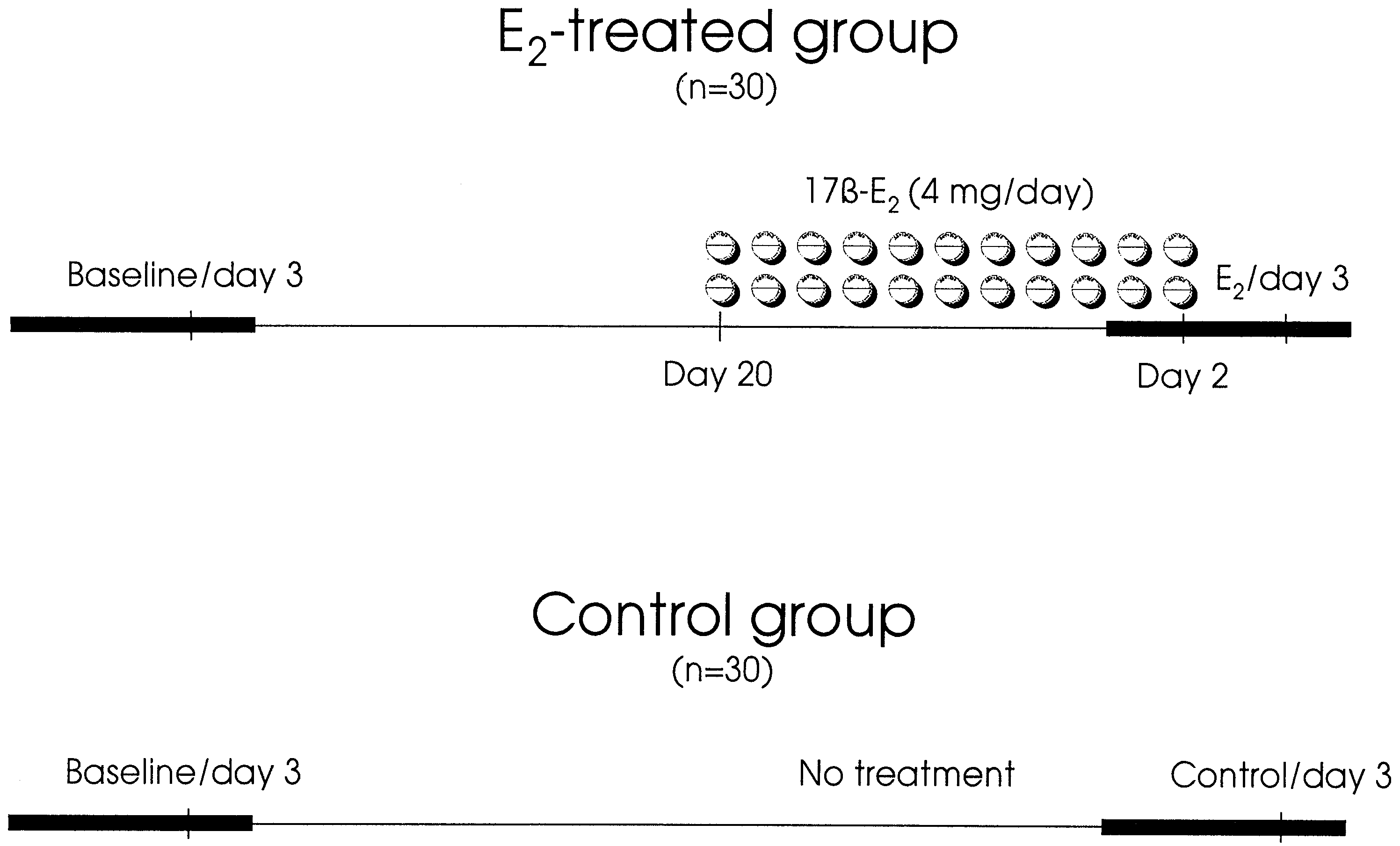
Study protocol. Horizontal black bars represent menstrual bleeding. On baseline/day 3, E /day 3, and control/day 3, hormonal
and ultrasound measurements were performed. Fanchin. Coordination of early antral follicles. Fertil Steril 2003.
menstrual bleeding paralleling the corpus luteum
clearance, or excretion; [4] body mass indexes ranging from
demise, FSH levels increase progressively to preserve antral
18 to 27 kg/m2; [5] no current hormone therapy; [6] adequate
follicles from atresia and ensure subsequent growth
visualization of ovaries in transvaginal ultrasound scans.
According to their inherent sensitivity to FSH, it is possible
Informed consent was obtained from all women, and this
that some early antral follicles are able to respond to lower
investigation received the approval of our internal Institu-
amounts of FSH than others and, therefore, to start their
tional Review Board. For personal reasons (n ϭ 4) or major
development during the late luteal phase This premature,
protocol violation (n ϭ 2), six women did not complete the
gradual exposure of follicles to FSH may accelerate the
two subsequent observation cycles required by the protocol
development of more sensitive follicles and accentuate size
and had to be excluded from the analysis. Therefore, the
discrepancies observed during the first days of the subse-
population studied was limited to 60 participants undergoing
Hence, we decided to challenge the hypothesis that size
discrepancies among early antral follicles result, at least in
Study Protocol
part, from their early and progressive exposure to FSH. For
The study protocol is summarized in On day 3
this we elected to artificially lower endogenous FSH secre-
of their menstrual cycles (baseline/day 3), all 60 women
tion during the luteal phase by administering E and
underwent blood sampling for serum FSH, inhibin B, and E
to measure follicular and hormonal profiles on day 3 in two
measurements at approximately 9:00 A.M. Later in the morn-
consecutive menstrual cycles that were either preceded or
ing, ultrasound scans of their ovaries were performed. Sub-
not preceded by luteal E administration.
sequently, women were randomized to receive luteal E2treatment or to serve as controls. As shown in
MATERIALS AND METHODS
participants who were included in the E -treated group (n ϭ
Subjects
30) received micronized 17-E oral tablets (4 mg/day;
We prospectively studied 66 female volunteers, 20 – 41
Provame`s, Cassenne Laboratories, Puteaux, France) in the
years of age. All participants met the following inclusion
evening at 8:00 P.M. from day 20 of the same cycle until day
criteria: [1] regular, ovulatory menstrual cycles every 25–35
2 of their next cycle. We chose the 4 mg/day dose for E p.o.
days; [2] both ovaries present; [3] no current or past diseases
administration because of its reported efficacy in reducing
affecting ovaries or gonadotropin or sex steroid secretion,
endogenous FSH and in preventing early follicular growth
FERTILITY & STERILITY
Participants who were included in the control group (n
Statistics
The measure of central tendency used was the mean and
the measure of the variability was the SD. Because of the
pairwise design of this study, data from each participant on
women (E /day 3) or on day 3 of the subsequent cycle in
E day 3 or on control day 3 were compared with corre-
control women (control/day 3), hormonal and ultrasound
sponding data for the same participant on baseline day 3 by
measurements similar to the preceding cycle (baseline/day 3)
using the paired Student’s t-test. To evaluate the magnitude
were performed. In addition, participants were asked to
of follicular size discrepancies from baseline day 3 to E day
compute their baseline and subsequent menstrual cycle
3 and from baseline day 3 to control day 3, we tested the
lengths and to report possible subjective changes in men-
homogeneity of variances by using the Levene test for equal
strual bleeding characteristics. In E -treated women, compli-
variances This test is less sensitive than F-tests to
ance of treatment was monitored to detect any protocol
departures from normality and allows a comparison of the
dispersion of data around the mean independent of meanvalues. In addition, SD:mean ratios for follicular sizes were
Ultrasound Measurements
also calculated. The present crossover study was powered to
Ultrasound scans were performed using a 4.5–7.2 MHz
detect anticipated differences of 0.5 mm for follicular sizes
multifrequency transvaginal probe (Siemens Elegra, Sie-
and 2 mm for ovarian volume calculation at Ͼ80% power at
mens S.A.S., Saint-Denis, France) by one single operator
a 0.5 significance level. PϽ.05 was considered statistically
(J.S.C.F.), who was not aware of the treatment schedule or
the hormonal results. The objective of the ultrasound exam-inations was to evaluate the number and sizes of early antralfollicles and to calculate the mean ovarian volume. We
considered all follicles that measured 2–12 mm in meandiameter (mean of 2 orthogonal diameters). The choice of
Ultrasound Results
not excluding follicles measuring 9 –12 mm was based on
Follicular and ovarian measurement results are summa-
the fact that, according to our own experience, some women
rized in As expected, the number of antral follicles
display marked acceleration of follicular development.
did not change significantly from one cycle to another inE -treated women and in controls. In contrast, we observed
In an attempt to optimize the reliability of ovarian follic-
a significant reduction of mean follicular sizes in E -treated
ular assessment, the ultrasound scanner that was used was
women from baseline/day 3 to E /day 3 but not in controls.
equipped with a tissue harmonic imaging system which
In agreement with this, mean ovarian volume decreased
allowed improved image resolution and adequate recogni-
significantly in women treated with E and remained un-
tion of follicular borders. Ovarian volumes, calculated ac-
changed in controls. In addition, we observed a remarkable
cording to the formula for an ellipsoid (0.526 ϫ length ϫ
attenuation of follicular size discrepancies on E day 3 as
height ϫ width) were the mean volume for both ova-
compared with baseline day 3 (PϽ.0001). This was not
ries. Intra-analysis coefficients of variation (CVs) for follic-
noticed between baseline day 3 and control day 3. Consis-
ular and ovarian measurements were Ͻ5%, and their lower
tently, SD:mean ratios for follicular sizes were significantly
lower on E /day 3 than on baseline/day 3 but not on control/
day 3 as compared with baseline/day 3, which confirms the
Hormonal Measurements
improvement in follicular size homogeneity observed in
All blood samples were obtained by venipuncture, and
E -treated women. Incidentally, it is noteworthy that ultra-
serum was separated and frozen in aliquots at Ϫ20°C for
sound measurements made on baseline/day 3 were strictly
subsequent centralized analysis. Serum FSH was measured
similar in women included in the E -treated and control
by an immunometric technique using an Amerlite kit (Ortho
Clinical Diagnostics, Strasbourg, France). Intra-assay andinterassay CVs were, respectively, 5% and 7%, and lower
Hormonal Results
limit detection was 0.1 mIU/mL for FSH. Serum inhibin B
Hormonal results are also presented in In women
was determined by double antibody enzyme-linked immu-
who were administered E during the luteal phase, serum
nosorbent assay (Serotec, Varilhes, France) as described
inhibin B levels were significantly lower on E /day 3 as
elsewhere Lower limit detection was 10 pg/mL, and
compared with baseline day 3, whereas no significant lon-
intra-assay and interassay CVs were Ͻ6% and Ͻ9%, respec-
gitudinal change in inhibin B levels was noted in controls.
tively, for inhibin B. Serum E was determined by an im-
As expected, E administration raised serum E to levels
munoometric technique using an Estradiol-60 Amerlite kit
comparable to those observed during the late follicular phase
(Ortho Clinical Diagnostics). Lower limit detection was 14
of the menstrual cycle (114 Ϯ 57 pg/mL on E day 3). Serum
pg/mL, and intra-assay and interassay CVs were 8% and 9%,
E levels did not vary significantly in controls from baseline/
day 3 to control/day 3. Administration of E lowered serum
Fanchin et al.
Ultrasound and hormonal results during two consecutive menstrual cycles in women receiving E during the luteal
Fanchin. Coordination of early antral follicles. Fertil Steril 2003.
FSH levels on E /day 3 as compared with baseline/day 3.
stringent methodological parameters such as population se-
However, in women who did not receive E treatment, serum
lection, randomized crossover design, accurate ultrasound
FSH levels remained steady from one cycle to the other. CVs
technology, and independent data analysis.
for FSH from the first to the second cycle were significantly
Our results indicated that E administration during the
higher in E -treated women than in controls (40% vs. 17%,
luteal phase effectively reduced both the size discrepancies
PϽ.01). As for ultrasound measurements, hormonal results
and the mean diameter of early antral follicles, consistent
obtained on baseline/day 3 were closely similar in women
with a decrease in mean ovarian volume. The observation of
receiving E as compared with those who served as controls.
a subtle but significant lengthening of menstrual cycle dura-
Clinical Results
tion in women pretreated with E is in keeping with this
As anticipated, the E -treated and the control groups were
effect. Indeed, although ovulation has not been monitored in
comparable with regard to ages of women (33.3 Ϯ 0.6 vs.
the present study, menstrual cycle lengthening after E treat-
33.3 Ϯ 0.5 years) and body mass index (21.8 Ϯ 0.4 and 21.8
ment may be attributed to a longer growth course of smaller
Ϯ 0.3 kg/m2). A significant lengthening of mean menstrual
antral follicles to ovulation. Furthermore, these results are in
cycle duration was observed in participants receiving E
accordance with data from previous experiments conducted
(29.4 Ϯ 1.3 days, PϽ.0001) as compared with their baseline
cycles (27.8 Ϯ 1.2 days). This phenomenon was not ob-
Earlier studies have shown that administration of physi-
served in controls (28.0 Ϯ 1.1 vs. 27.9 Ϯ 0.8 days, respec-
ological E doses effectively prevents and postpones the
tively). Moreover, E treatment did not alter the baseline
intercycle FSH elevation In line with this, the
cycle length in E -treated patients (27.8 Ϯ 1.2 days) as
present investigation showed lower FSH levels (Ͻ4.5 mIU/
compared with controls (27.9 Ϯ 0.8 days). Participants did
mL) on the day after E discontinuation as compared with
not indicate any significant change in their menstrual bleed-
baseline (Ͼ7 mIU/mL). This phenomenon may not be at-
ing characteristics in E -treated as compared with baseline
tributable to physiological intercycle FSH fluctuations be-
cause it was not duplicated in the control group. In addition,the intercycle CV for FSH observed in E -treated patients
DISCUSSION
(40%) significantly exceeded the intercycle CVs in controls
The present study was designed to investigate whether E
(17%) and the CVs for FSH measured in the early follicular
administration during the luteal phase could affect the degree
phase as reported by other investigators (Ͻ18%)
of development of early antral follicles during the first days
Therefore, both the reduction of follicular size and heter-
of the subsequent follicular phase. We wanted to challenge
ogeneity observed by the present study lead us to hypothe-
the hypothesis that developmental asynchrony of early antral
size that, after E administration, serum FSH levels might
follicles possibly results from the gradual FSH elevation that
have remained beneath the putative FSH threshold for early
occurs during the late luteal phase. This phenomenon may
antral follicular development Indeed, during the late
promote asynchronous growth of follicles because of their
luteal phase of the menstrual cycle, spontaneous demise of
intrinsic dissimilar sensitivity to FSH Hence,
the corpus luteum leads to a progressive rise in FSH that
through its putative suppressive effect on FSH secretion
starts approximately 5 days before menses and reaches se-
E administration might attenuate follicular size
rum levels Ͼ7 mIU/mL as early as 3 days before the onset
heterogeneity. To address this issue, our investigation set
of menstrual bleeding It is possible that the obtained
FERTILITY & STERILITY
reduction of FSH secretion might have altered the pace of
References
early follicular development during the intercycle transition.
1. McNatty KP, Hillier SG, van den Boogaard AM, Trimbos-Kemper TC,
Reichert LE Jr, van Hall EV. Follicular development during the luteal
phase of the human menstrual cycle. J Clin Endocrinol Metab 1983;
marked decrease in serum inhibin B levels as compared with
2. Fauser BC, Van Heusden AM. Manipulation of human ovarian func-
baseline. Although the mechanisms implicated in this phe-
tion: physiological concepts and clinical consequences. Endocrinol Rev1997;18:71–106.
nomenon are unclear, it is conceivable that the E -induced
3. Gougeon A, Lefevre B. Evolution of the diameters of the largest
reduction of mean follicular size and the decreased FSH
healthy and atretic follicles during the human menstrual cycle. J ReprodFertil 1983;69:497–502.
secretion acted together to lower serum inhibin B to levels
4. Gougeon A. Regulation of ovarian follicular development in primates:
similar to those described during the luteal phase of the
facts and hypotheses. Endocrinol Rev 1996;17:121–55.
5. Hillier SG, van den Boogaard AM, Reichert LE Jr, van Hall EV.
Intraovarian sex steroid hormone interactions and the regulation offollicular maturation: aromatization of androgens by human granulose
The coordination of early antral follicles achieved by
cells in vitro. J Clin Endocrinol Metab 1980;50:640 –7.
6. Roseff SJ, Bangah ML, Kettel LM, Vale W, Rivier J, Burger HG, et al.
luteal E administration may provide a basis for new thera-
Dynamic changes in circulating inhibin levels during the luteal-follic-
peutic perspectives. During COH, the variability in size of
ular transition of the human menstrual cycle. J Clin Endocrinol Metab1989;69:1033–9.
growing follicles may be counterproductive. In IVF-ET,
7. Mais V, Cetel NS, Muse KN, Quigley ME, Reid RL, Yen SS. Hor-
because of the discordant maturation of follicular-oocyte
monal dynamics during luteal-follicular transition. J Clin EndocrinolMetab 1987;64:1109 –14.
complexes, the precise timing for hCG administration is hard
8. Chun SY, Eisenhauer KM, Minami S, Billig H, Perlas E, Hsueh AJ.
to determine for all follicles at once. This leads to fewer
Hormonal regulation of apoptosis in early antral follicles: follicle-stimulating hormone as a major survival factor. Endocrinology 1996;
mature oocytes and fewer available embryos, a factor that
limits embryo selection for ET. Indeed, the large number of
9. Klein NA, Battaglia DE, Fujimoto VY, Davis GS, Bremner WJ, Soules
MR. Reproductive aging: accelerated ovarian follicular development
available embryos constitutes an important prognostic factor
associated with a monotropic follicle-stimulating hormone rise in nor-
of IVF-ET outcome, possibly by increasing the probability
mal older women. J Clin Endocrinol Metab 1996;81:1038 –45.
10. Zeleznik AJ. Premature elevation of systemic estradiol reduces serum
that at least one good-quality embryo will be selected for ET
levels of follicle-stimulating hormone and lengthens the follicular phase
of the menstrual cycle in rhesus monkeys. Endocrinology 1981;109:352–5.
In addition, our present data provide a possible explana-
11. de Ziegler D, Jaaskelainen AS, Brioschi PA, Fanchin R, Bulletti C.
Synchronization of endogenous and exogenous FSH stimuli in con-
tion for the larger number of follicles, oocytes, and embryos
trolled ovarian hyperstimulation (COH). Hum Reprod 1998;13:561–4.
reported with COH protocols preceded by GnRH agonist or
12. Thomas JD, Rubin DN. Tissue harmonic imaging: why does it work?
J Am Soc Echocardiogr 1998;11:803–8.
oral contraceptive administration as compared with COH
13. Sharara FI, McClamrock HD. The effect of aging on ovarian volume
measurements in infertile women. Obstet Gynecol 1999;94:57–60.
protocols without luteal FSH control These differ-
14. Groome NP, Illingworth PJ, O’Brien M, Pai R, Rodger FE, Mather JP,
ences are possibly due to improved synchronization of fol-
et al. Measurement of dimeric inhibin B throughout the human men-strual cycle. J Clin Endocrinol Metab 1996;81:1401–5.
licular development achieved after luteal FSH suppression as
15. Levene H. Contributions to probability and statistics: Essays in honor of
a result of GnRH agonist or oral contraceptive pretreatment.
Harold Hotelling. In: Olkin I, et al, eds. Stanford: Stanford UniversityPress, 1960:278 –92.
Yet studies comparing the characteristics of early antral
16. Brown JB. Pituitary control of ovarian function— concepts derived
follicles after pituitary desensitization by GnRH agonists or
from gonadotrophin therapy. Aust N Z J Obstet Gynaecol 1978;18:46 –54.
oral contraceptive administration with those observed after
17. le Nestour E, Marraoui J, Lahlou N, Roger M, de Ziegler D, Bouchard
luteal E administration are needed to verify this assumption.
P. Role of estradiol in the rise in follicle-stimulating hormone levels
during the luteal-follicular transition. J Clin Endocrinol Metab 1993;
Similarly, the faster follicular growth, the reduced number of
oocytes and available embryos, and the remarkable trend to
18. Zeleznik AJ. Premature elevation of systemic estradiol reduces serum
levels of follicle-stimulating hormone and lengthens the follicular phase
poorer IVF-ET outcome observed in GnRH antagonist, as
of the menstrual cycle in rhesus monkeys. Endocrinology 1981;109:
compared with long GnRH agonist protocols are con-
19. van Weissenbruch MM, Schoemaker HC, Drexhage HA, Schoemaker
sistent with this hypothesis. Hence, the possible improve-
J. Pharmaco-dynamics of human menopausal gonadotrophin (HMG)
ment of GnRH antagonist protocol outcome by E pretreat-
and follicle-stimulating hormone (FSH). The importance of the FSH
concentration in initiating follicular growth in polycystic ovary-like
disease. Hum Reprod 1993;8:813–21.
20. Brown JR, Liu HC, Sewitch KF, Rosenwaks Z, Berkeley AS. Variabil-
In conclusion, luteal E administration reduces size dis-
ity of day 3 follicle-stimulating hormone levels in eumenorrheic
crepancies of early antral follicles during the early follicular
women. J Reprod Med 1995;40:620 –4.
21. Devreker F, Pogonici E, De Maertelaer V, Revelard P, Van den Bergh
phase. This approach may constitute a simple and promising
M, Englert Y. Selection of good embryos for transfer depends on
method to foster follicular growth synchronization during
embryo cohort size: implications for the ‘mild ovarian stimulation’debate. Hum Reprod 1999;14:3002–8.
COH. If these results are confirmed, luteal E administration
22. Opsahl MS, Blauer KL, Black SH, Lincoln SR, Thorsell L, Sherins RJ.
represents a potential, more physiological alternative to
The number of embryos available for transfer predicts successful preg-nancy outcome in women over 39 years with normal ovarian hormonal
GnRH agonist or oral contraceptive pretreatment. Yet, fur-
reserve testing. J Assist Reprod Genet 2001;18:551–6.
ther studies are needed to investigate whether the coordina-
23. MacLachlan V, Besanko M, O’Shea F, Wade H, Wood C, Trounson A,
et al. A controlled study of luteinizing hormone-releasing hormone
tion of selectable follicles induced by E
agonist (buserelin) for the induction of folliculogenesis before in vitro
during the luteal phase improves the results of short GnRH
fertilization. N Engl J Med 1989;320:1233–7.
24. Tan SL, Kingsland C, Campbell S, Mills C, Bradfield J, Alexander N,
agonist or antagonist protocols and IVF-ET outcome.
et al. The long protocol of administration of gonadotropin-releasing
Fanchin et al.
hormone agonist is superior to the short protocol for ovarian stimulation
contraceptives before in vitro fertilization. Fertil Steril 1990;53:282–7.
for in vitro fertilization. Fertil Steril 1992;57:810 –4.
27. Borm G, Mannaerts B. Treatment with the gonadotrophin-releasing
25. Cramer DW, Powers DR, Oskowitz SP, Liberman RF, Hornstein MD,
hormone antagonist ganirelix in women undergoing ovarian stimu-
McShane PM, et al. Gonadotropin-releasing hormone agonist use in
lation with recombinant follicle stimulating hormone is effective,
assisted reproduction cycles: the influence of long and short regimens
safe and convenient: results of a controlled, randomized, multicentre
on pregnancy rates. Fertil Steril 1999;72:83–9.
trial. The European Orgalutran Study Group. Hum Reprod 2000;15:
26. Gonen Y, Jacobson W, Casper RF. Gonadotropin suppression with oral
FERTILITY & STERILITY
Reinhold Schmitt, Gründer von «www.isa-casinos.de» Wie kommt man dazu ein Internet- Por tal für das Geldspiel zu eröffnen? Millionenfach wurde die isa-Casinos bereits angeklickt. Kostenlos. Ha ben leer ist. ISA gibt die Realität weiter und Sie als Spieler genug Geld verdient um sich ein solch aufwendiges Hob- by leisten zu können? Also ehrlich, haben Sie einen
FOR IMMEDIATE RELEASE Contact: Jacqueline Trost May 17, 2006 313-576-8629 International Collaboration to Benefit Cancer Patients in Turkey The Barbara Ann Karmanos Cancer Institute and Metropolitan Florence Nightingale Hospital and Cancer Center in Istanbul Enter One-of-a-Kind Agreement DETROIT, MI - Today, the Barbara Ann Karmanos Cancer Institute and the Metropolitan Florence Nightingale Hospita

 Study protocol. Horizontal black bars represent menstrual bleeding. On baseline/day 3, E /day 3, and control/day 3, hormonal
and ultrasound measurements were performed.
Study protocol. Horizontal black bars represent menstrual bleeding. On baseline/day 3, E /day 3, and control/day 3, hormonal
and ultrasound measurements were performed. Ultrasound and hormonal results during two consecutive menstrual cycles in women receiving E during the luteal
Fanchin. Coordination of early antral follicles. Fertil Steril 2003.
FSH levels on E /day 3 as compared with baseline/day 3.
Ultrasound and hormonal results during two consecutive menstrual cycles in women receiving E during the luteal
Fanchin. Coordination of early antral follicles. Fertil Steril 2003.
FSH levels on E /day 3 as compared with baseline/day 3.