Ordered, immediately called back and the same day delivered the order.Very pleased with the work. Thank you for prompt and accurate work https://africarx.co.za/ great prices, delivered on the day of the order. Pleasant managers consult by phone.
Selective dorsal rhizotomy: meta-analysis of three randomized controlled trials
Cerebral palsy (CP) has an incidence and prevalence rate ofabout two per 1000 in children (Grether et al.1992, Yeargin-
Allsopp et al. 1992). Spasticity is a major clinical feature of over75% of cases of CP and is conventionally considered to be amajor cause of discomfort, gait abnormalities, and function-
al limitations for persons with CP. Many resources have beendirected at the treatment of spasticity and the current treat-
ment choices include oral medications, orthotics, orthopaedicsurgical procedures, electrical stimulation, intramuscular
injections, physiotherapy, ‘selective’ dorsal rhizotomy, con-tinuous intrathecal baclofen infusion, and a host of alterna-tive treatment methods.
Many of the treatments introduced for spasticity and other
aspects of CP were inadequately evaluated when first intro-
duced (McKenzie 1988) and have become enshrined in clini-
cal practice without benefit of acceptable evidence of efficacy
Nancy Temkin PhD, Children’s Hospital and Regional
and effectiveness. Over the last 15 years, the rigor of clinical
research methodology has advanced considerably (Spilker
Paul Steinbok MBBS FRCSC, Children’s and Women’s
1991). Valid and reliable outcome measures have been devel-
oped for many relevant aspects of CP ranging from electro-
Virginia Wright BSc (PT) MSc, Bloorview MacMillan Centre,
mechanical torque measures of spasticity (Price et al. 1991)
and instrumented gait analysis (Sutherland 1988, Gage
Ann Reiner BSR MA, Children’s and Women’s Health
1991, Perry 1992) to measures of functional ability (Russell
et al. 1989, Haley et al. 1991, Msall et al. 1997), and quality of
Theodore Roberts MD, Children’s Hospital and Regional
‘Selective’ dorsal rhizotomy (SDR) emerged as a popular
James Drake MBBCh, FRCSC, Hospital for Sick Children,
surgical intervention for spasticity in North America and else-
where since the early 1980s (Peacock and Staudt 1991, Park
Maureen O’Donnell MD, Children’s and Women’s Health
and Owen 1992, Abbott et al. 1993). History of the develop-
ment of this procedure, including the introduction of elec-
Peter Rosenbaum MD, Bloorview MacMillan Centre,
trophysiological criteria for ‘selecting’ dorsal root tissue for
transection, has been reviewed repeatedly in the literature
Jason Barber BS, University of Washington;
(Albright 1992, Park and Owen 1992, Hays et al. 1997). Many
Anne Ferrel BS, Children’s Hospital and Regional Medical
published results of open consecutive surgical series strongly
suggested that SDR reduced spasticity substantially, improvedfunction, and involved no unacceptable short-term risks when
*Correspondence to first author at Children’s Hospital and
carried out by experienced interdisciplinary clinical teams
Regional Medical Center, Mail Stop 47, 4800 Sand Point Way
(Peacock and Staudt 1991, Steinbok et al. 1992, McLaughlin et
al. 1994, Nishida et al. 1995). Enthusiasm was tempered by
concerns about long-term effects, questions about the validityof the root tissue selection process (Landau and Hunt 1990,Cohen and Webster 1991, Logigian et al. 1994, Steinbok et al. 1994, Hays et al. 1998), and recognition that uncontrolledclinical series are open to bias in favor of a positive outcome
This study is a comparative analysis and meta-analysis of three
(Neville 1988, McLaughlin et al. 1994).
randomized clinical trials. Children with spastic diplegia received
Three randomized clinical trials have been published:
either ‘selective’ dorsal rhizotomy (SDR) plus physiotherapy
Steinbok et al. 1997 (Vancouver), McLaughlin et al. 1998,
(SDR+PT) or PT without SDR (PT-only). Common outcome
(Seattle), and Wright et al. 1998 (Toronto). Main results of
measures were used for spasticity (Ashworth scale) and
these three studies are presented in Table I. All three studies
function (Gross Motor Function Measure [GMFM]). Baseline
confirmed that SDR consistently reduces or eliminates spastici-
and 9- to 12-month outcome data were pooled (n=90). At
ty. There is a difference in the functional outcome with two
baseline, 82 children were under 8 years old and 65 had Gross
studies showing a statistically significant advantage for SDR
Motor Function Classification System level II or III disability.
(Steinbok et al. 1997, Wright et al. 1998) and the third showing
Pooled Ashworth data analysis confirmed a reduction of
no advantage (McLaughlin et al. 1998). The major similarities
spasticity with SDR+PT (mean change score difference –1.2;
and differences regarding the design of these studies are out-
Wilcoxon p<0.001). Pooled GMFM data revealed greater
functional improvement with SDR+PT (difference in change
This paper presents a comparative analysis and meta-analy-
score +4.0, p=0.008). Multivariate analysis in the SDR+PT
sis of these three studies. The primary aim of these analyses
group revealed a direct relationship between percentage of dorsal
was to identify the factors responsible for the different out-
root tissue transected and functional improvement. SDR+PT is
comes of the studies and to clarify whether SDR makes a statis-
efficacious in reducing spasticity in children with spastic diplegia
tically significant contribution to the functional improvement
and has a small positive effect on gross motor function.
of children with spastic CP up to 1 year after the operation.
Developmental Medicine & Child Neurology 2002, 44: 17–25
Function Classification System (GMFCS) provides a means of
A search of Medline, the Cochrane Collaboration database,
rank-ordering the functional severity of cerebral palsy (CP)
recent scientific meeting abstracts, and contacts with other
based on age-adjusted clinical descriptors (Palisano et al.
researchers in the field did not reveal the existence of any
1997). A developmental pediatrician familiar with the GMFCS
other randomized clinical trials of SDR as of December 2000.
and masked with respect to participant identification andstudy group assignment, but not study site, retrospectively
reviewed selected clinical descriptions of all participants. Data
The senior study biostatistician reviewed the research proto-
from each child were assigned a GMFCS baseline score, which
cols from each site to compare details of the study designs
was entered into the multivariate analyses.
(Tables III and IV). Common definitions were agreed uponfor key variables. The three studies all used the Ashworth
scale for spasticity (Bohannon and Smith 1987) and the
All three centers provided children in both the SDR with
Gross Motor Function Measure (GMFM; Russell et al. 1989)
physiotherapy (SDR+PT) groups and the PT without SDR
as major outcome variables. The 12-month data from Seattle
(PT-only) groups with physiotherapy programs of stretching,
and Toronto and the 9-month outcome data from Vancouver
strengthening, and training in functional movements intend-
ed to enhance mobility (Tables IV and Va and b). The greatest
The data were entered into SPSS software (version 7.5.3).
number of planned treatment hours for both groups was pro-
Complete data were obtained for all variables reported
vided in Seattle, and the fewest in Vancouver. Seattle and
except baseline ambulation status. No new data were collect-
Vancouver physiotherapy protocols stressed equivalency of
ed for the present report. The original three studies were
treatments for both groups. The Toronto protocol called for a
approved by the ethics committees of the respective institu-
stronger emphasis on strengthening and on postural control
for the SDR+PT group as compared with the PT-only group
The developers of the GMFM have published an improved
based on the rationale that the anticipated weakening effect
scaling method (GMFM-66) that addresses the linearity of
of the surgery would provide a negative bias. Treatment plan-
the individual items scores across the entire range of GMFM
ning for the PT-only group in Toronto was based on written
scores (Russell et al. 2000). In these analyses we calculated
goals set by community therapists before the randomized
group assignment. Postoperative protocols for the surgical
In the initial descriptions and single-center analyses, the
groups in all three centers varied in emphasis and timing
markers of severity were the initial diagnosis (spastic diple-
gia), qualitative descriptors (mild, moderate, or severe), ambu-latory status, and the baseline GMFM score. The Gross Motor
DATA ANALYSISCharacteristics of the three samples were compared usingKruskal–Wallis distribution-free analysis of variance (ANOVA)for continuous or ordered variables and χ2 or Fisher’s exact
Table I: Selective dorsal rhizotomy randomized clinical trials
tests for unordered categorical variables. For each outcome,
the change in the SDR+PT group was compared with that inthe PT-only group using two methods: blocked Wilcoxon’s
test (blocking on site; Marascuilo and McSweeney 1997) and
ANOVA including factors for treatment group, site, and atreatment by site interaction. To evaluate the effect of charac-
teristics or the effect of SDR on outcome as measured by
Ashworth, GMFM, and GMFM-66, separate multiple regres-
sion analyses were performed. These analyses used backward
selection and the following additional predictors: age, sex,
birthweight, ambulatory status, baseline GMFM-66, and base-
line lower-extremity Ashworth score. Regardless of signifi-
Vancouver, Steinbok et al. 1997; Toronto, Wright et al. 1998; Seattle,
cance, site was included in the models; all other variables
required a significance level of p<0.05 to be retained. Oncesignificant main effects were identified, two-way interactionsamong the included variables were evaluated. Effects of per-cent of root tissue transected were studied in the same fash-
Table II: Selective dorsal rhizotomy randomized clinical trials
ion, except site was not automatically retained as a factor.
A descriptive summary of the samples from the three studies
and the pooled data is presented in Table VI. The Seattle
study was the only one to include children (n=8) who were 8
years of age or older at baseline. The Vancouver study had an
unusual sex ratio (17/28 were female) for a sample of chil-
dren with CP. The three samples were similar with respect to
prematurity. The children in the Seattle sample were slightly
more heterogeneous with respect to intellectual function
Developmental Medicine & Child Neurology 2002, 44: 17–25
and cause of CP. At baseline, the children in the Toronto sam-
scores and had less dorsal root tissue transected (25%) than
ple had what appeared to be somewhat more severe CP as
was the case in the other two studies (41 and 45%). In each of
judged by the GMFCS, GMFM, and clinical rating of ambula-
the three original studies, there were no differences in base-
tory status, although the amount of spasticity as judged by
line characteristics between treatment groups so the corre-
the baseline Ashworth scale was not greater. The children in
sponding analysis is not presented here for the pooled data.
the Seattle sample had noticeably lower baseline Ashworth
The main results comparing the magnitude of change in
Table III: Selective dorsal rhizotomy study design comparison
2-sample t-test on change –4 measures,
2-sample t-test, Wilcoxon on change, χ2,
Fisher’s exact (both intent-to-treat and
aNote: first number is number of children in SDR+PT group, second number is number of children in PT-only group; bButler et al. 1984;cStokes et al. 1990. SDR, selective dorsal rhizotomy; PT, physiotherapy; OT, occupational therapy; ROM, range of motion.
Selective Dorsal Rhizotomy Meta-analysis John McLaughlin et al.
weaker direct correlation that remained statistically signifi-
and all differences among studies as we have endeavoured to
cant (p=0.02). The potential effects of outliers and of section-
do in this report. The strengths of this meta-analysis should
ing S2 root tissue were examined by eliminating relevant data
not be overlooked. Many meta-analyses are carried out by
from the analyses. No appreciable effects were identified.
investigators not involved in any of the original studies and
There was a consistent and statistically significant (p=0.0002)
who may not have clinical experience with either the disor-
inverse correlation between the baseline GMFM-66 score and
der or the intervention being studied. As a consequence, the
the percent of dorsal root tissue transected (Fig. 7), i.e. the
authors of a meta-analysis may have access only to published
lower the score, the more dorsal root tissue was cut, regard-
data, which are inevitably a summary of the raw data. This study
less of study site. Inclusion of baseline GMFM-66 score in the
is the product of close collaboration among the teams who
regression model did not change the relations of outcome
published the original results of all randomized trials of SDR
variables to per cent of dorsal root tissue transected.
conducted and published to date. Unpublished raw data werepooled and all data was available for reanalysis. It was possibleto ensure that all variables had common definitions across
studies and to recalculate variables when necessary. In short,
Meta-analysis is a well established, if still evolving, methodolo-
the circumstances of this meta-analysis assured that compara-
gy for synthesizing outcomes from existing studies of a single
ble data were pooled from the three studies. Many meta-analy-
research question (Moher et al. 1999). The procedure remains
ses suffer from diminished specificity of outcomes arising from
counter-intuitive for clinicians and suffers from both uncritical
the need to reduce disparate outcome variables across multi-
acceptance and categorical disregard. The applicability of a
ple studies to a common proxy variable. In this study, identical
given meta-analysis is best revealed by setting forth limitations
outcome variables were used in the three original studies for
Table VI: Selective dorsal rhizotomy study sample characteristics
Baseline lower extremity Ashworth scale (SD)
aInformation missing on one patient; binformation missing on three patients; c information missing on eightpatients (some of these were adoptions or other circumstances where we were unable to determine cause.
Table VII: Selective dorsal rhizotomy multivariate analysis: main results
Developmental Medicine & Child Neurology 2002, 44: 17–25
the SDR+PT versus PT-only groups for the pooled three-
weak inverse correlation (p=0.03) between percent of dorsal
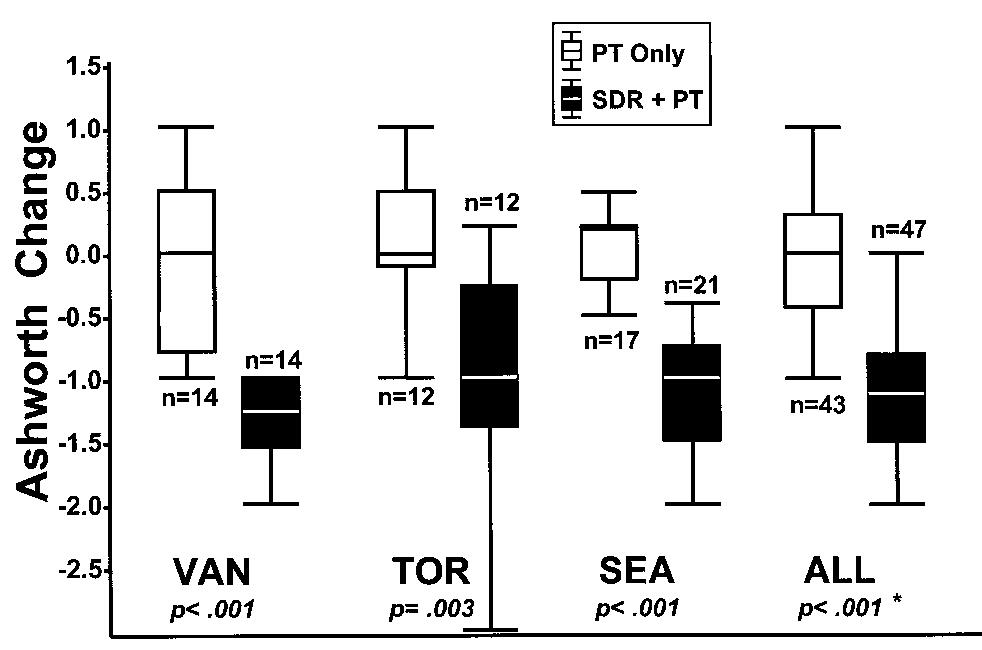
study sample are presented in Figures 1, 2, and 3. Ashworth
root tissue transected and change in Ashworth scores (Fig. 4).
scale change scores were clinically robust and similar across
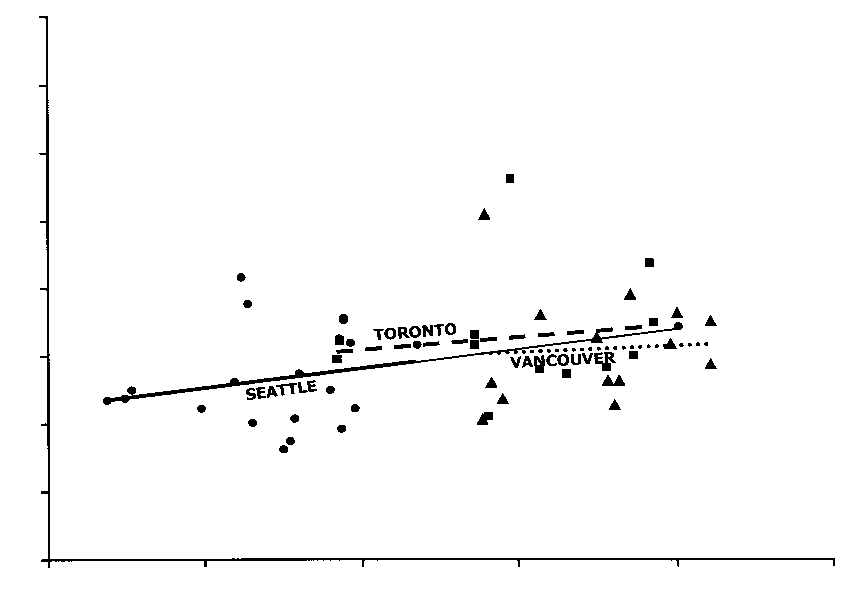
There was a statistically significant direct relation (p<0.001)
all three studies with a mean difference in change between
between GMFM change score and percent of dorsal root tis-
groups of –1.2 points which was statistically significant using
sue transected (Fig. 5). The regression lines for the individual
the Wilcoxon’s blocked on site (p<0.001). Mean difference
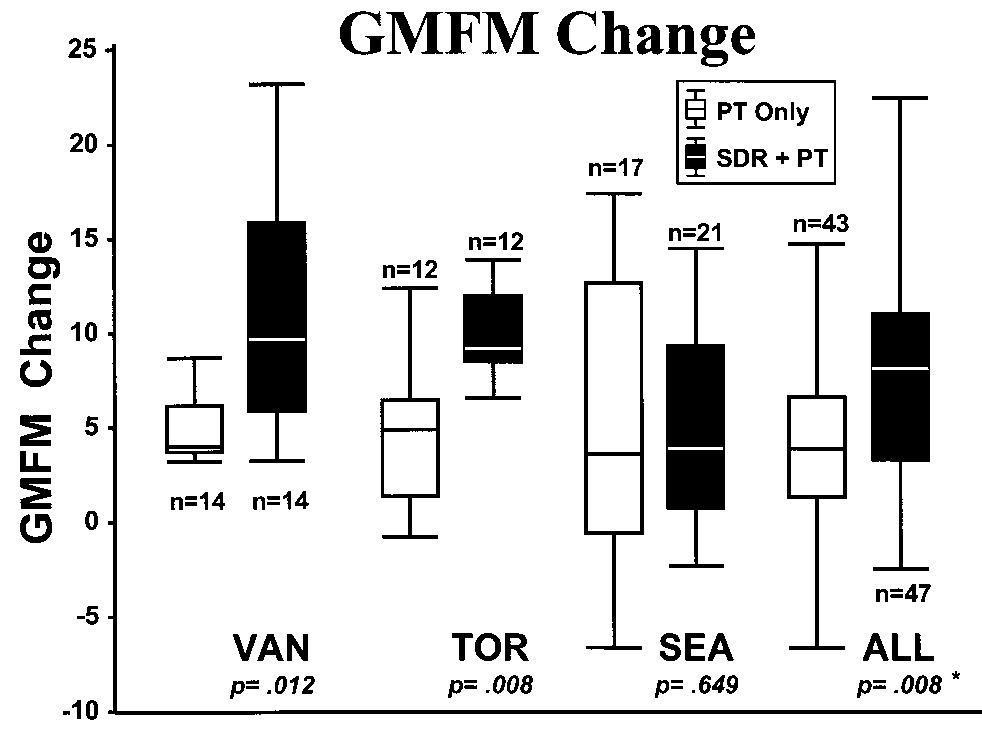
sites appear to be very similar. There was an apparent direct
in change score in the GMFM (4.0) was statistically significant
effect of site (p=0.005) that disappeared after adjustment for
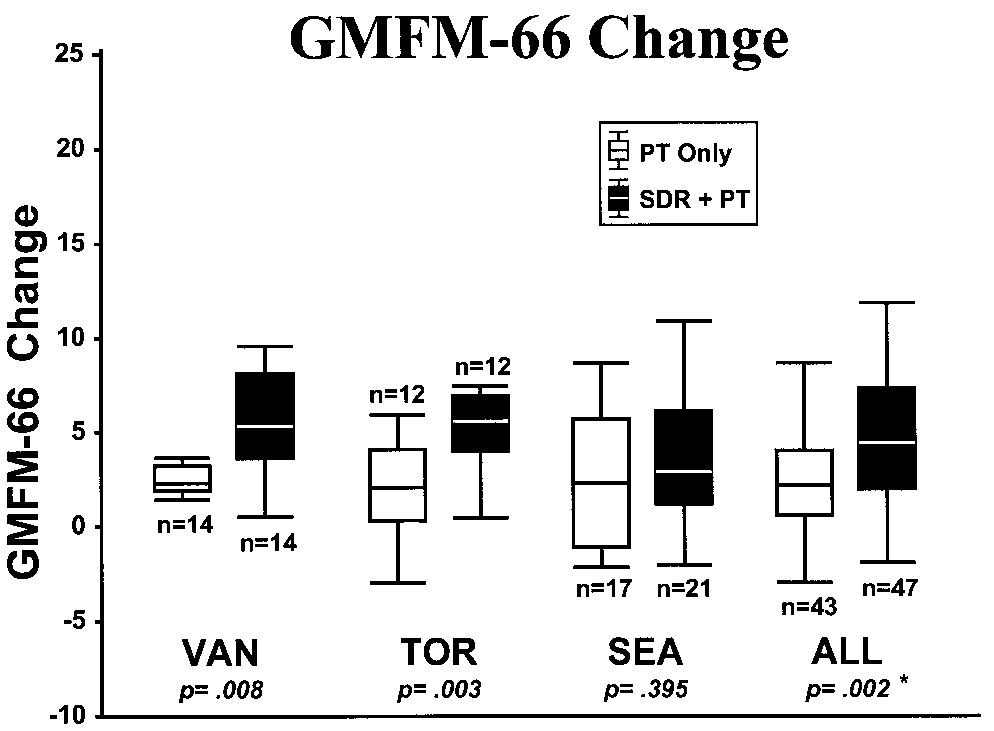
(p=0.008) by Wilcoxon’s blocked on site. When the GMFM-
percent of dorsal root tissue transected (p=0.6). There was
66 scores were used, the mean difference in change score for
no interaction effect with study site. The same analysis was
the pooled data was smaller (2.6) and remained statistically
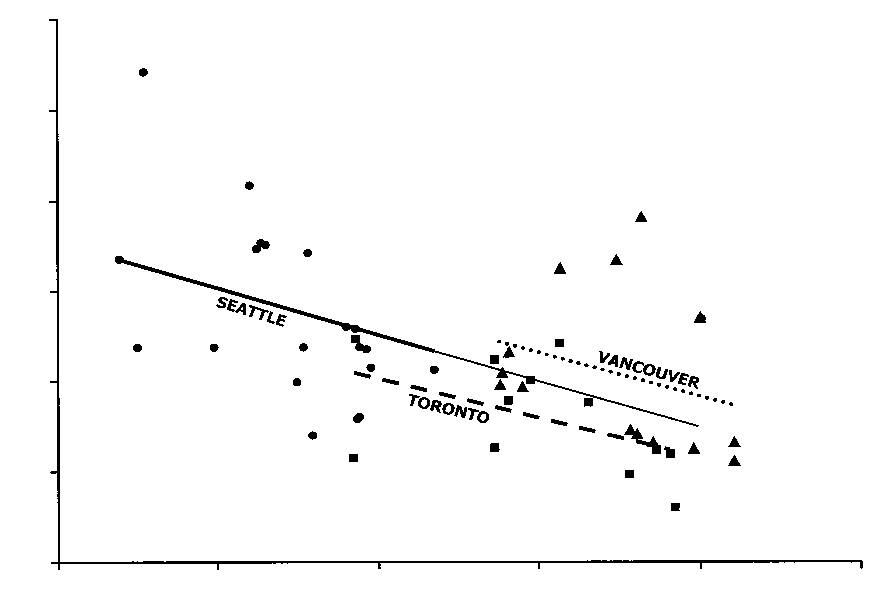
performed for GMFM-66 change score (Fig. 6) and revealed a
significant (p=0.002) by Wilcoxon’s blocked on site.
Multivariate analysis was carried out to detect effects
attributable to site-related differences in baseline variablespresented in Table VI and to look for interactions suggesting
Table IV: Physiotherapy by treatment group
subgroup effects (e.g. younger versus older participants).
Baseline characteristics were chosen as clinically plausiblecandidate variables. The analyses were done with and with-
out the data for the eight children from the Seattle study, who
were 8 years of age or more at baseline. No differences in
results were seen, and age was not a significant covariate.
Subsequent analysis excluded these older children. As shown
in Table VII, the effect of SDR was significant on all outcomes.
There was no evidence that this effect differed by baseline
characteristics or by study site (i.e. there was no significant
treatment by site interaction). Based on the lack of interac-tional effects in the multivariate model, no subgroup defined
by baseline characteristics was identified for which SDR is
particularly effective. This was confirmed by looking at mean
effects within and across sites in subgroups defined posthoc(analysis not presented). Retrospective GMFCS classification
of baseline severity was not related to outcome.
Regression analysis of the outcomes for the SDR+PT
groups at the three study sites and the pooled data reveal a
Table Va: Comparison of postoperative physiotherapy protocols: timing of intervention
Start transition movements (to sit, side-sit, all fours,
Table Vb: Comparison of physiotherapy protocols: muscle groups treated
Hip adductors, flexors, hamstrings, and heel-cords
Hip adductors, flexors, hamstrings, and heel-cords
Hip adductors, flexors, hamstrings, and heel-cords
Hip adductors, flexors, hamstrings, and heel-cords
Hip adductors, flexors, hamstrings, and heel-cords
Lower extremity muscle groups, abdominals, and trunk extensors
Strengthening through functional activities
Selective Dorsal Rhizotomy Metaanalysis John McLaughlin et al.
both spasticity and functional outcomes. The only loss of
statistically significant advantage to SDR+PT compared with
rigor is that the Ashworth scale measurements were not col-
PT-only that is independent of any site-specific differences
lected by masked observers in two of the studies. The critical-
among the studies. It is difficult to know the clinical impor-
ly important functional outcomes were measured by masked
tance of a mean difference in change score of 4 percentage
assessment of GMFM scores in all participants.
points on the GMFM. It was not possible to identify any sub-
The primary conclusion supported by the meta-analysis is
groups of children with specific characteristics who benefit-
that the pooled results of the three studies show a small but
ed more than others included in the studies.
It was expected that the multivariate analysis would iden-
tify a specific reason for the difference in outcome among thethree studies. Several of the differences in the studies seemedlikely to explain the divergent outcomes. The most obvious
difference is the surgical technique. The Seattle study used
the electrophysiological monitoring technique and criteria
for transecting dorsal root tissue popularized by Peacock
(Staudt et al. 1995) and other clinicians. The Vancouver
study utilized similar criteria for root tissue assessment, but
the primary basis for root tissue transection was preopera-
tive clinical assessment. The Toronto study used electrophys-
iological monitoring only to differentiate dorsal from ventral
roots. The amount of dorsal root tissue transected was 25%
in the Seattle study and was 41% and 45% respectively in the
other two studies. If these apparently major differences were
responsible for the difference in outcome, one would expect
the study site by treatment interaction variable to be statisti-cally significant in the multivariate analysis model. No such
Ashworth change score. PT Only and SDR+PT
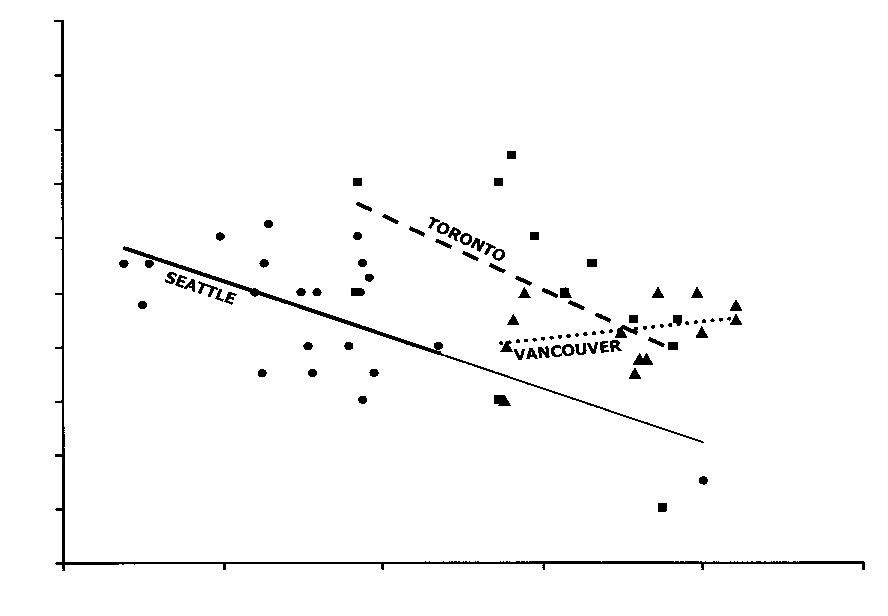
The regression analysis of outcome change scores on per-
group data for individual studies and pooled meta-
cent dorsal root tissue transected (Figs 4 to 6) of the SDR+PT
analysis. Interval is from baseline to 12 months after
group data provides further insight. Patients who had a larg-
beginning treatment (9 months for Vancouver). Boxes
er amount of dorsal root tissue transected had more improve-
represent the 25th, 50th, and 75th centiles. Whiskers
ment on GMFM (p<0.001), GMFM-66 (p=0.02), and Ashworth
represent minimum and maximum values excluding
score (p=0.03). As seen in the figures, the effect is modest
outliers beyond 1.5 times the interquartile range.
for GMFM, smaller for GMFM-66, and perhaps inconsistent
*p values are based on Wilcoxon’s tests, with blocking on
across sites for the Ashworth scale. Adjustment for per cent
Figure 2: Gross Motor Function Measure (GMFM) change
Figure 3: GMFM-66 change score. PT Only and SDR+PTscore. PT Only and SDR+PT group data for individual studiesgroup data for individual studies and pooled meta-analysis.and pooled meta-analysis. Interval is from baseline to 12Interval is from baseline to 12 months after beginningmonths after beginning treatment (9 months for Vancouver).treatment (9 months for Vancouver). Boxes represent 25th,Boxes represent 25th, 50th, and 75th centiles. Whiskers50th, and 75th centiles. Whiskers represent the minimumrepresent minimum and maximum values excluding outliersand maximum values excluding outliers beyond 1.5 timesbeyond 1.5 times the interquartile range. *p values are basedthe interquartile range. *p values are based on Wilcoxon’son Wilcoxon’s tests, with blocking on site for combined test.tests, with blocking on site for combined test.Developmental Medicine & Child Neurology 2002, 44: 17–25
of dorsal root tissue eliminated evidence of site effect (see
the biggest mean percent of dorsal root tissue transected
Fig. 5) on GMFM change in the SDR+PT pooled data (p=0.6
(45%) but was not dramatically different from the Toronto
after adjustment). The per cent of dorsal root tissue transect-
study (41%). The Seattle study (25%) was clearly different
ed is related to baseline GMFM-66 (Fig. 7, p<0.001) which
from the other two in this regard. There are at least two pos-
suggests that the initial functional level may have influenced
sible interpretations. First, the Ashworth scale is not known
the extent of transection. Including baseline GMFM-66 score
to have good interrater or test–retest reliability, so perhaps it
in the regression did not change the models substantially.
is simply a problem of measurement. Using a quantitative
Although the relation of percentage of dorsal root tissue
electromechanical torque measure of spasticity in a larger
transected to outcome has biological plausibility, caution is
group of children undergoing SDR, no relation could be
essential in ascribing a causal effect to a factor that was not
demonstrated between spasticity and the percent of dorsal
assigned at random. It is not possible to rule out a chance dif-
root tissue transected (Hays et al. 1998). Second, perhaps it
ference in functional outcome or some other undetected
takes a smaller amount of dorsal root transection to abolish
deep tendon reflexes, clonus, and clinically detectable spastic-
The inverse relation of Ashworth score to percent of dor-
ity than it does to influence function. Perhaps the Vancouver
sal root tissue transected is statistically significant (p=0.03,
investigators performed sufficiently extensive rhizotomies to
see Fig. 4). However, the interaction with site showed a trend
get beyond a range of reduction in spasticity that would be
(p=0.08) and inspection of the individual regression lines in
expected to have a dose-response curve while the other two
Figure 4 suggests that the Vancouver data are different from
studies still show such a response. The amount of functional
the other two in this respect. The Vancouver study reported
change may still show a strong dose–response correlation in
Figure 4: Regression analyses of Ashworth change score by
Figure 6: Regression analyses of GMFM-66 change score by% dorsal root tissue transected. Linear regression analysis% dorsal root tissue transected. Linear regression analysis(p=0.03). "––, Seattle; #– –, Toronto; $---, Vancouver.(p=0.02). "––, Seattle; #– –, Toronto; $---, Vancouver.
Figure 5: Regression analyses of GMFM change score by %
Figure 7: Regression analyses of baseline GMFM-66 by %dorsal root tissue transected. Linear regression analysisdorsal root tissue transected. Linear regression analysis(p<0.001). "––, Seattle; #– –, Toronto; $---, Vancouver.(p<0.001). "––, Seattle; #– –, Toronto; $---, Vancouver.
Selective Dorsal Rhizotomy Meta-analysis John McLaughlin et al.
the range of tissue transection described in the Toronto and
ed primarily ambulatory children with spastic diplegia and
excluded those with dystonia, athetosis, and ataxia. Children
The severity of CP was retrospectively reclassified accord-
with severe visual impairment were excluded. All the chil-
ing to the GMFCS system from baseline clinical data. The
dren undergoing SDR in these studies had access to peri-
amount and quality of clinical data available differed across
operative and postoperative care at a regional children’s
studies, which limits the ability to make inferences based on
hospital in affluent societies, and access to expert pediatric
GMFCS scores in the pooled sample. Changes in GMFCS
physiotherapists for postoperative rehabilitation. Regular
classification determined prospectively might be another
follow up by an experienced clinical team may have mitigat-
method for capturing global changes in response to specific
ed adverse events and motivated families in ways that were
not measured. The effects of SDR on spasticity can probablybe safely extrapolated to most children with spasticity, but
this meta-analysis provides no comparison to other available
This meta-analysis of the 9- to 12-month outcomes of three
effective treatments. The effects of SDR on function are mod-
randomized clinical trials confirms a clinically important
change in spasticity. With regard to function, a small but sta-
Based on clinical experience in addition to these data,
tistically significant advantage to SDR+PT (additional mean
we speculate that SDR might be most effective for a child
GMFM change of 4 percentage points) was shown when
between 3 and 8 years of age whose functional level falls into
compared with PT-only. There appears to be a direct relation
GMFCS levels III and IV. Children in this age range are easy to
between the percent of dorsal root tissue transected and the
assess, tolerate the physiotherapy regimens, and have acade-
magnitude of gain in function. The sectioning rate was not
mic and social demands that can accommodate an intensive
randomized and the sectioning technique varied across stud-
intervention. Children with more severe CP may have more
ies. This statistical correlation may not reflect a true cause
potential gain from an invasive procedure.
and effect relation. There are no detectable subgroups thatbenefit more than others. The three original studies did notreport any worrisome problems with adverse events. These
Accepted for publication 17th August 2001.
are short-term outcomes applicable to a child who meets thecriteria used for enrollment in these studies.
These results suggest that the decision whether or not to
Funding was generously provided by the United Cerebral PalsyResearch & Educational Foundation. Funding for the original
perform SDR on a similar child partly rests on whether or not
studies was provided by the National Institute for Neurological
an anticipated mean GMFM change score increment of 4 per-
Disease and Stroke, RO1-NS27867 (Seattle), the British Columbia
centage points above the amount of change with non-invasive
Health Care Research Foundation (Vancouver), and the Easter Seal
care justifies the time, effort, and risk involved. While an addi-
Research Institute of Canada and the United Cerebral Palsy
tional change of 4 percentage points over a year might be
Research & Educational Foundation (Toronto). No author has afinancial interest in any aspect of this study. Elaine Smith provided
twice the change expected with non-invasive care, it is still a
invaluable assistance with the manuscript. The authors gratefully
relatively small amount of change compared with some of the
acknowledge the assistance of colleagues at each of the three
claims in uncontrolled studies (Peacock and Staudt 1991,
centers and the cooperation of the families.
Park and Owen 1992, Abbott et al. 1993, Nishida et al. 1995). These modest improvements in gross motor function aresomewhat disappointing, but it should be noted that these
results are short term and do not take into account other pos-
Abbott R, Johann-Murphy M, Shiminski-Maher T, Quartermain D,
sible positive and negative long-term outcomes. In addition to
Forem SL, Gold JT, Epstein FJ. (1993) Selective dorsal rhizotomy:
improving ambulation, an effective surgical treatment for
outcome and complications in treating spastic cerebral palsy.
spastic diplegia should have beneficial long-term effects on
gait parameters, pain reduction, and rate of acquired muscu-
Albright AL. (1992) Neurosurgical treatment of spasticity: selective
posterior rhizotomy and intrathecal baclofen. Stereotactic and
loskeletal deformity, function, participation, and quality of
Functional Neurosurgery 58: 3–13.
life. As was the case in these studies, there should be a low rate
Bohannon RW, Smith MB. (1987) Interrater reliability of a modified
of serious adverse events attributable to the intervention.
Ashworth scale of muscle spasticity. Physical Therapy 67: 206–7.
Answers to these important questions will not become avail-
Butler P, Engelbrecht M, Major RE, Tait JH, Stallard J, Patrick JH.
(1984) Physiologic cost index of walking for normal children and
able until a sizable well-studied cohort of individuals with
its use as an indicator of physical handicap. Developmental
spastic diplegia is followed to adulthood. There is serious
Medicine & Child Neurology 26: 607–12.
doubt regarding the validity of the electrophysiological moni-
Cohen AR, Webster HC. (1991) How selective is selective posterior
toring criteria that formed the basis for the ‘selectivity’ of dor-
rhizotomy? Surgical Neurology 35: 267–72.
sal rhizotomy (Cohen and Webster 1991, Steinbok et al. 1994,
Gage JR. (1991) Gait Analysis in Cerebral Palsy. London: Mac Keith
Logigian et al. 1996, Hays et al. 1998), yet this meta-analysis
Grether JK, Cummins SK, Nelson KB. (1992) The California
suggests that the percent of dorsal root tissue transected may
Cerebral Palsy Project. Paediatric Perinatal Epidemiology
be important. The correct method to determine where and
how much dorsal root tissue to transect must be elucidated by
Haley SM, Coster WJ, Faas RM. (1991) A content validity study of the
Pediatric Evaluation of Disability Inventory. Pediatric Physical
Clinicians are faced with the practical problem of deciding
Hays RM, McLaughlin JF, Bjornson KB, Stephens K, Roberts TS,
whether or not to recommend treatments such as SDR for
Price R. (1998) Electrophysiologic monitoring during selective
individual children. The results of this meta-analysis should
dorsal rhizotomy, and spasticity and GMFM performance.
be used with care in the clinical setting. These studies includ-
Developmental Medicine & Child Neurology 40: 233–8. Developmental Medicine & Child Neurology 2002, 44: 17–25
Hays RM, McLaughlin JF, Geiduschek JM, Bjornson KF, Graubert CS.
— Keyes R, Langill L, Cochrane DD. (1994) The validity of
(1997) Evaluation of the effects of selective dorsal rhizotomy.
electrophysiological criteria used in selective functional
Mental Retardation and Developmental Disabilities Research
posterior rhizotomy for treatment of spastic cerebral palsy. Journal of Neurosurgery 81: 354–61.
Landau WM, Hunt CC. (1990) Dorsal rhizotomy, a treatment of
— Reiner AM, Beauchamp RD, Armstrong RW, Cochrane DD, Kestle
unproven efficacy. Journal of Child Neurology 5: 174–8.
J. (1997) A randomized clinical trial to compare selective
Landgraf J, Abetz L. (1996) Measuring health outcomes in pediatric
posterior rhizotomy plus physiotherapy with physiotherapy
populations: issues in psychometrics and application. In: Spilker
alone in children with spastic diplegic cerebral palsy.
B, editor. Quality of Life and Pharmacoeconomics in ClinicalDevelopmental Medicine & Child Neurology 39: 178–84. Trials. Philadelphia: Lippincott-Raven. p 793–802.
Stokes NA, Dietz JR, Crowe TW. (1990) The Peabody Developmental
Logigian EL, Wolinsky JS, Soriano SG, Madsen JR, Scott RM. (1994)
Fine Motor Scale: an interrater reliability study. American
H reflex studies in cerebral palsy patients undergoing partial
Journal of Occupational Therapy 44: 334–40.
dorsal rhizotomy. Muscle and Nerve 17: 539–49.
Sutherland D, Olshen R, Biden E, Wyatt M. (1988) The Development
— Shefner JM, Goumnerova L, Scott RM, Soriano SG, Madsen J. of Mature Walking. Clinics in Developmental Medicine Nos
(1996) The critical importance of stimulus intensity in
104/5. London: Mac Keith Press.
intraoperative monitoring for partial dorsal rhizotomy. Muscle
Wright FV, Sheil EM, Drake JM, Wedge JH, Naumann S. (1998)
Evaluation of selective dorsal rhizotomy for the reduction of
Marascuilo LA, McSweeney M. (1997) Nonparametric and
spasticity in cerebral palsy: a randomized controlled trial. Distribution Free Methods for the Social Sciences. Monterey, CA:
Developmental Medicine & Child Neurology 40: 239–47.
Yeargin-Allsopp M, Murphy CC, Oakley GP. (1992) A multiple-source
McKenzie S. (1988) Clinical trials, statistics, and dilemmas. Archives
method for studying the prevalence of developmental disabilities
of Disease in Childhood 63: 231–4.
in children: the Metropolitan Atlanta Developmental Disabilities
McLaughlin JF, Bjornson KF, Astley SJ, Hays RM, Hoffinger SA,
Study. Pediatrics 89: 624–30.
Armantrout EA, Roberts TS. (1994) The role of selective dorsalrhizotomy in cerebral palsy: critical evaluation of a prospectiveclinical series. Developmental Medicine & Child Neurology36: 755–69.
— — — Graubert C, Hays RM, Roberts TS, Price R, Temkin N. (1998)
Selective dorsal rhizotomy: efficacy and safety in an investigator-masked randomized clinical trial. Developmental Medicine &Child Neurology 40: 220–32.
Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF.
(1999) Improving the quality of reports of meta-analyses ofrandomised controlled trials: the QUOROM statement. Lancet354: 1896–900.
Msall ME, Rogers BT, Ripstein H, Lyon N, Wilczenski F. (1997)
Measurements of functional outcomes in children with cerebralpalsy. Mental Retardation and Developmental DisabilitiesResearch Reviews 3: 194–203.
Neville BG. (1988) Selective dorsal rhizotomy for spastic cerebral
palsy. Developmental Medicine & Child Neurology 30: 395–8.
Nishida T, Thatcher SW, Marty GR. (1995) Selective posterior
rhizotomy for children with cerebral palsy: a 7-year experience. Childs Nervous System 11: 374–80.
Palisano R, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B.
(1997) Development and reliability of a system to classify grossmotor function in children with cerebral palsy. DevelopmentalMedicine & Child Neurology 39: 214–23.
Park TS, Owen JH. (1992) Surgical management of spastic diplegia
in cerebral palsy. New England Journal of Medicine 326: 745–9.
Peacock WJ, Staudt LA. (1991) Functional outcomes following
selective posterior rhizotomy in children with cerebral palsy. Journal of Neurosurgery 74: 380–5.
Perry J. (1992) Gait Analysis: Normal and Pathological Function.
Price R, Bjornson KF, Lehmann JF, McLaughlin JF, Hays RM. (1991)
Quantitative measurement of spasticity in children withcerebral palsy. Developmental Medicine & Child Neurology 33: 585–95.
Russell D, Rosenbaum P, Cadman D, Gowland C, Hardy S, Jarvis S.
(1989) The Gross Motor Function Measure: a means to evaluatethe effects of physical therapy. Developmental Medicine & ChildNeurology 31: 341–52.
Russell DJ, Avery LM, Rosenbaum PL, Raina PS, Walter SD, Palisano
RJ. (2000) Improved scaling of the Gross Motor FunctionMeasure for children with cerebral palsy: evidence of reliabilityand validity. Physical Therapy 80: 873–85.
Spilker B. (1991) Guide to Clinical Trials. New York: Raven Press. Staudt LA, Nuwer MR, Peacock WJ. (1995) Intraoperative
monitoring during selective posterior rhizotomy: technique andpatient outcome. Electroencephalography and ClinicalNeurophysiology 97: 296–309.
Steinbok P, Reiner AM, Beauchamp RD, Cochrane DD, Keyes R.
(1992) Selective functional posterior rhizotomy for treatment ofspastic cerebral palsy in children. Review of 50 consecutive cases. Pediatric Neurosurgery 18: 34–42.
Selective Dorsal Rhizotomy Meta-analysis John McLaughlin et al.
ALLERGENIC EXTRACT STANDARDIZED SHORT RAGWEED Final container label would reflect AU/ml For Physicians Use Only WARNING: This product should be diluted prior to use. WARNINGS Standardized Short Ragweed allergenic extract is intended for use by, or under the guidance of, physicians who are experienced in the administration of allergenic extracts for diagnosis and/or
VIEW ONLY PCSK9 mAbs or even vaccines – the new statins? LONDON, UK----18th March 2013----ExpertREACT. Novel PCSK9 (proprotein convertases subtilisin/kexin type 9) inhibitors, such as Sanofi’s anti-PCSK9 monoclonal antibody SAR236553, have impressive LDL-C reducing efficacy. PCSK9 vaccines may represent an alternative strategy to the monoclonal antibody approach, taking
 both spasticity and functional outcomes. The only loss of
statistically significant advantage to SDR+PT compared with
rigor is that the Ashworth scale measurements were not col-
PT-only that is independent of any site-specific differences
lected by masked observers in two of the studies. The critical-
among the studies. It is difficult to know the clinical impor-
ly important functional outcomes were measured by masked
tance of a mean difference in change score of 4 percentage
assessment of GMFM scores in all participants.
points on the GMFM. It was not possible to identify any sub-
The primary conclusion supported by the meta-analysis is
groups of children with specific characteristics who benefit-
that the pooled results of the three studies show a small but
ed more than others included in the studies.
both spasticity and functional outcomes. The only loss of
statistically significant advantage to SDR+PT compared with
rigor is that the Ashworth scale measurements were not col-
PT-only that is independent of any site-specific differences
lected by masked observers in two of the studies. The critical-
among the studies. It is difficult to know the clinical impor-
ly important functional outcomes were measured by masked
tance of a mean difference in change score of 4 percentage
assessment of GMFM scores in all participants.
points on the GMFM. It was not possible to identify any sub-
The primary conclusion supported by the meta-analysis is
groups of children with specific characteristics who benefit-
that the pooled results of the three studies show a small but
ed more than others included in the studies.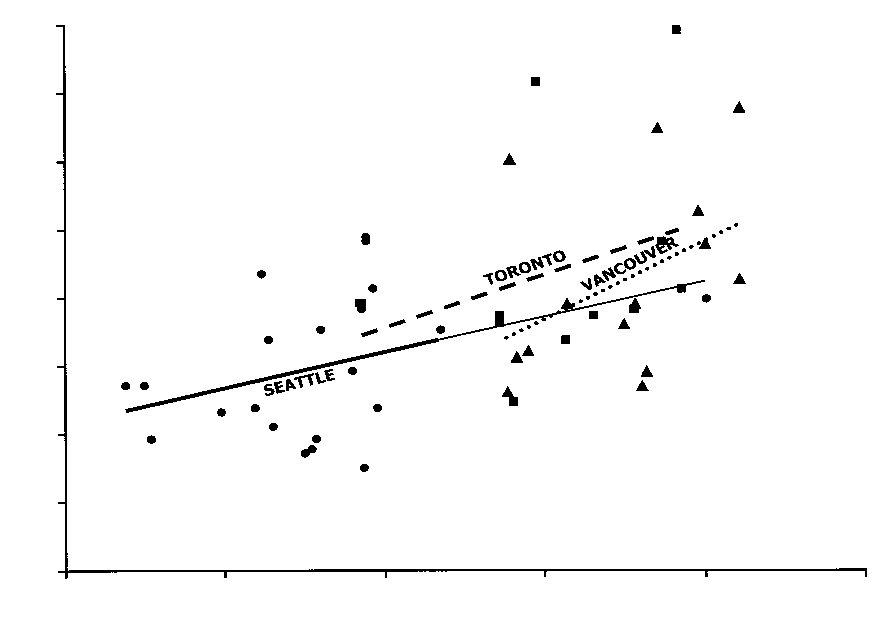
 of dorsal root tissue eliminated evidence of site effect (see
the biggest mean percent of dorsal root tissue transected
Fig. 5) on GMFM change in the SDR+PT pooled data (p=0.6
(45%) but was not dramatically different from the Toronto
after adjustment). The per cent of dorsal root tissue transect-
study (41%). The Seattle study (25%) was clearly different
ed is related to baseline GMFM-66 (Fig. 7, p<0.001) which
from the other two in this regard. There are at least two pos-
suggests that the initial functional level may have influenced
sible interpretations. First, the Ashworth scale is not known
the extent of transection. Including baseline GMFM-66 score
to have good interrater or test–retest reliability, so perhaps it
in the regression did not change the models substantially.
of dorsal root tissue eliminated evidence of site effect (see
the biggest mean percent of dorsal root tissue transected
Fig. 5) on GMFM change in the SDR+PT pooled data (p=0.6
(45%) but was not dramatically different from the Toronto
after adjustment). The per cent of dorsal root tissue transect-
study (41%). The Seattle study (25%) was clearly different
ed is related to baseline GMFM-66 (Fig. 7, p<0.001) which
from the other two in this regard. There are at least two pos-
suggests that the initial functional level may have influenced
sible interpretations. First, the Ashworth scale is not known
the extent of transection. Including baseline GMFM-66 score
to have good interrater or test–retest reliability, so perhaps it
in the regression did not change the models substantially.











 Hays RM, McLaughlin JF, Geiduschek JM, Bjornson KF, Graubert CS.
Hays RM, McLaughlin JF, Geiduschek JM, Bjornson KF, Graubert CS.