Ordered, immediately called back and the same day delivered the order.Very pleased with the work. Thank you for prompt and accurate work https://africarx.co.za/ great prices, delivered on the day of the order. Pleasant managers consult by phone.
Mm00188 (00) asd case study - hijazi lrg secundum:layout 1.qxd
Closure of Large Secundum-Type ASD with theAMPLATZER Septal Occluder
Ziyad M. Hijazi, MD George M. Eisenberg Professor Department of Pediatrics and Medicine Section of Pediatric Cardiology The University of Chicago Hospital Chicago, IL U.S.A. Patient History
the connecting waist was deployed in the left atrium)
A 67-year old female was diagnosed at the age of
resulted in successful closure. Correct device
57 to have an atrial septal defect. Primary symptoms
position was verified by TEE and by pulling and
were shortness of breath and easy fatigability. Her
pushing on the delivery cable to confirm secure
anchoring of the device (“Minnesota Wiggle”). The
considered to be in NYHA functional class III-IV due
device was released by counterclockwise rotation of
to severe right heart failure. She developed
the pin vise. Repeat TEE evaluation revealed
significant atrial dysrhythmias for which she was
complete closure of the defect (Figure 3). An
maintained on amiodarone, digoxin and Coumadin.
She was referred for the possibility of catheter
catheterization laboratory failed due to heart failure
closure. She was also maintained on lasix and
and pulmonary edema. Therefore, the patient was
allowed to recover in the Cardiac Care Unit. Shewas discharged home one week later on her above
Dianostic Findings
medications. The fluoroscopic time was 30 minutes
A transesophageal echocardiogram (TEE) was
and total procedure time was 115 minutes. On
performed and revealed the presence of a large,
follow-up, her symptoms improved significantly and
secundum type ASD measuring 23mm with large
she is now in NYHA functional class I-II. Repeat
right atrium and ventricle (Figure 1).
TEE after 4 months revealed complete closure withdecrease in the right atrium and ventricle size
Procedure Description
Under general endotracheal anesthesia andcontinuous TEE monitoring, routine right and left
Discussion
heart catheterization was performed. The pulmonary
This case illustrates the major benefits of device
artery pressure was 38/16 (24) mm Hg with
closure in this high surgical risk patient. The risk of
descending aortic pressure of 83/43 (56) mm Hg.
surgery would have been significantly increased due
The Qp/Qs ratio was 2.2:1 The balloon diameter of
to her heart failure, pulmonary edema and atrial
the defect was measured to be 27mm (Figure 2). An
arrhythmia. Her defect size was big with a stop-flow
8 Fr sheath (AGA Medical Corp.) was passed over
diameter of 27mm. Conventionally, we would have
the guidewire into the left upper pulmonary vein. A
liked the device size to be equal or 1mm larger than
26mm AMPLATZER Septal Occluder was attached
the stop-flow diameter of the defect. However,
to the delivery cable, compressed into the loader
because of her condition, we decided to implant the
and introduced into the sheath. An initial attempt at
largest device available at the time, a 26mm
deploying the device resulted in pulling of the device
AMPLATZER Septal Occluder. The fact that the
across the thin septum into the right atrium.
device is easily recapturable and repositionable after
Therefore, the device was recaptured and a repeat
deployment of both discs increased our confidence
attempt with modification of the deployment (part of
in attempting the implantation which resulted incomplete closure of the defect.
Figure 1: Longitudinal TEE view revealing a 23mm secundum type ASD with left-to-right shunt and RA enlargement priorto closure. Note the thin inferior septum (arrow).
Figure 2: 4-chamber view TEE image during balloon sizing of the defect, the stop-flow diameter is 27mm.
Figure 3: Longitudinal TEE image with color after closure using a 26mm AMPLATZER Septal Occluder revealing gooddevice position and no residual shunt.
Longitudinal TEE images without (figure 4) and with color (figure 5) four months after device closure, revealing gooddevice position and no residual shunt. Note the change in the profile of the device.
Refer to Instructions for Use for a complete listing of indications and usage, contraindications, warnings, andprecautions. AMPLATZER is a registered trademark of AGA Medical Corporation. AGA Medical Corporation,2006. Not in any way connected with medical gas or equipment sold under the “AGA” brand by AGA AB orits successors. This device may not be available in all markets. Contact AGA Medical Corporation for availability.
Diabete di tipo 2, parità metformina-acarbose nella riduzione della glicata Stando ai risultati di uno studio randomizzato condotto su una popolazione cinese, lo studio MATCH, acarbose e metformina hanno un’efficacia simile nel controllo glicemico nei pazienti con diabete di tipo 2 (DT2) di nuova diagnosi. Un’implicazione dello studio, appena pubblicato su Lancet, è che acarbose potrebb
must contact Horizon directly. This will enable Horizon to better answer your questions and service you in the event that you may need any assistance. For questions or assistance, please direct your email to productsupport@horizonhobby.com, or call 877.504.0233 toll free to speak to a service technician. Inspection or Repairs If this Product needs to be inspected or repaired, please call for a
 Closure of Large Secundum-Type ASD with theAMPLATZER Septal Occluder
Ziyad M. Hijazi, MD
Closure of Large Secundum-Type ASD with theAMPLATZER Septal Occluder
Ziyad M. Hijazi, MD
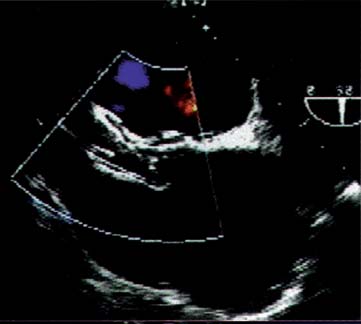
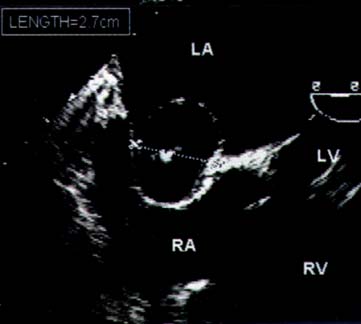
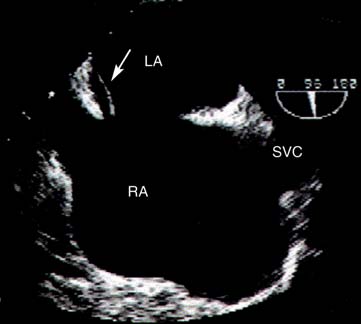

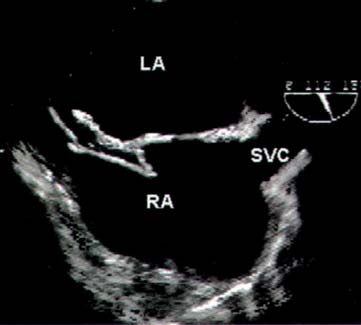 Figure 1: Longitudinal TEE view revealing a 23mm secundum type ASD with left-to-right shunt and RA enlargement priorto closure. Note the thin inferior septum (arrow).
Figure 1: Longitudinal TEE view revealing a 23mm secundum type ASD with left-to-right shunt and RA enlargement priorto closure. Note the thin inferior septum (arrow).