Thank you, it's cool. Used for the first time because only then was the right drug. Very revealing detail: ordered Express shipping to get the order within 3 hours because didn't know how to get the order faster https://africarx.co.za/buy-levitra-south-africa.html The drug is authentic exactly. Consistent with the stated prices the Staff is knowledgeable.
Gastric electrical stimulation
G a s t r i c E l e c t r i c a l S t i m u l a t i o n What is Gastric Electrical
conservative therapies are candidates for GES. Stimulation (Enterra™
Many of these patients have difficulty eating
DIGESTIVE Therapy)?
and experience severe, chronic vomiting and nausea. Some patients may even require tube
DISEASE CENTER
Gastric electrical stimulation (GES) utilizes an
feeding to ensure adequate nutrition. There are
electrical device, Enterra™ Therapy, called a
a number of causes for gastroparesis including
GASTROINTESTINAL
gastric pacemaker, to provide mild electrical
diabetes mellitus, anorexia and bulimia, lupus,
stimulation to the lower stomach nerves. MOTILITY
and brain disorders. However, nearly 60% of
Transmitted through a neurostimulator, these
the cases have an unknown origin. GES is used
SERVICES
mild electrical pulses encourage the stomach
only when medication is not effective in
to contract and help to relieve nausea and
controlling symptoms that can be serious,
vomiting. Utilizing minimally invasive surgical
including malnutrition and severe dehydration.
techniques, the gastric pacemaker is placed
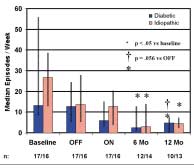
In clinical studies, GES reduced vomiting
At California Pacific
frequency by up to 81% from baseline at 12
Medical Center we are
abdomen. Two intramuscular lead wires with
electrodes are implanted into the stomach
committed to bringing
muscle wall to deliver mild electrical pulses for
new and advanced Vomiting frequency
symptom control. This therapy is reversible and
diagnostic tools, medical
can be turned off at any time by the motility
treatments and surgical options to the physicians we serve and the patients they care for. Through this procedure profile, our physicians illustrate actual medical situations that provide you with a window into their practice of diagnosis, treatment Gastric emptying and patient follow-up.
The Enterra™ Therapy system was designatedas a Humanitarian Use Device by the FDA inthe fall of 1999. Humanitarian Use Devices aremedical devices specially designated by theFDA for use in treatment of rare medical con-ditions with an incidence of less than 4000patients per year. Why does a patient need GES?
Patients diagnosed with gastroparesis, a
For patient referrals: (888) 637–2762
stomach more slowly than normal, who have
www.cpmc.org case studies 1. Diabetic Gastroparesis/ Sarcoidodis Case Overview
A 31 year-old female was referred to theComplex Digestive Disease Center presenting with extensive nausea andvomiting which required seven hospital-izations in the last eight months. Thepatient has been treated unsuccessfullywith Zofran, Reglan and erytromycian onprior admissions in an attempt to controlher symptoms. The diagnostic gastro-intestinal motility study showed absenceof phase 3 contractions in the stomach. Esophagogastroduodenoscopy identifiedno obstructions of the stomach. Thepatient continued to experience vomit-ing, nausea with epigastric discomfort
Laparoscopic image of electrodes attached to stomach wall.Treatment 2. Idiopathic Gastroparesis/ Gastric Reflux/
laparoscopic gastric pacemaker insertion. Hiatal Hernia Case Overview
with a five-year history of severe uncon-
severe gastric reflux and had undergonea laparoscopic cholecystectomy, which
affecting her ability to maintain employ-
lems were stable with little vomiting ornausea. The patient returned for a gastricemptying study showing normal gastric
Treatment
intestinal motility studies and a gastricemptying study to confirm gastroparesis.
It was decided that a laparoscopic Nissen
fundoplication, pyloroplasty and lysis of
adhesions be performed to reduce hersevere reflux, prior to insertion of the
3. Diabetes Mellitus/ Gastroparesis Case Overview
A 34-year-old diabetic man was referredto the Complex Digestive Disease Centerwith a 7-year history of severe gastro-paresis. He had been unable to tolerateor had been unresponsive to conven-tional medical therapy for this condition. He was recently seen in his local hospital emergency room due to his inability tomaintain minimal nutritional intakewhere a nasogastric tube was placed todecompress the abdomen. He had beenhospitalized 10 times in the last year andvomiting up to 6 times a day. He had lostapproximately 100 pounds over the lastfour years. The patient had a T-half emptying time of 280 minutes with noisotope leaving the stomach for twohours. X-ray of implanted Enterra™ deviceTreatment Gastric Emptying Study
ultrasound, gastric and small intestinalmotility studies and a gastric emptyingstudy to confirm gastroparesis. It wasdecided that he was an excellent candidate for insertion of the gastricpacemaker device.
His surgery proceeded without compli-cations and he was discharged home forfollow-up with his local GI specialist.
T-half emptying time of 280 minutes tonormal of 45 minutes. G a s t r i c E l e c t r i c a l S t i m u l a t i o n What are the risks? What can a patient For more information
• Risks associated with general anesthe-
Medical Director, Gastrointestinal Motility
each patient requires, the batteries last
rarely notice the mild stimulation to the
• Persistent pain at the neurostimulator
Director, Minimally Invasive SurgeryPatient referral to the Gastrointestinal Motility Services How is the gastric
mary care provider or physician specialistprior to scheduling their evaluation and
electrical stimulator
surgery. Medical records, pertinent labo-
implanted?
The implantation of the gastric electrical
to be forwarded to California Pacific’s
mately 21/2" long, 2" wide and 1/2" thick,
indication appropriateness. Patients need
is done surgically under general anesthe-
to be seen in consultation prior to sched-
uling the Enterra™ Therapy procedure.
implants two small electrodes into thestomach muscle wall. Lead connectors
Insurance coverage
are run subcutaneously along theabdomen and connected to the neu-
the belt line. The duration of surgery is
coverage for this service and obtain prior
required to stay overnight in the hospital
Copyright California Pacific Medical Center. All rights reserved. • MOT-gaselecstimpro-2002
Polycythemia Vera Dr. Jeannie Callum Updated May 2003 Introduction PV is a chronic, clonal, myeloproliferative disorder, classically associated with an increase in red cellmass, leukocytosis, thrombocytosis, splenomegaly, thrombosis and bleeding. 2 in 100 000 incidence with peak age of 60. 20% of patients present with thrombosis and 30% develop in follow-up despite control of disease
Patient name: __________________________________________________ 1. D/C home when awake, oriented and vital signs stable. 4. Provide Rx when patient goes home. These are located on the last page of Dr. Watson's Discharge Instruction form or on the chart. 5. Have patient and family READ and SIGN Dr. Watson's Discharge Instruction form and provide a copy for the permanent chart and provide the or

 G a s t r i c E l e c t r i c a l S t i m u l a t i o n
G a s t r i c E l e c t r i c a l S t i m u l a t i o n case studies
case studies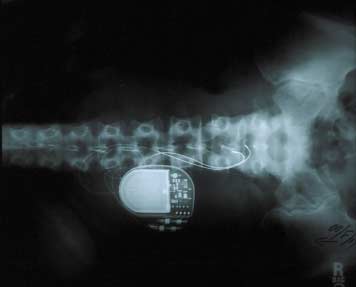
 3. Diabetes Mellitus/
3. Diabetes Mellitus/