Thank you, it's cool. Used for the first time because only then was the right drug. Very revealing detail: ordered Express shipping to get the order within 3 hours because didn't know how to get the order faster https://africarx.co.za/buy-levitra-south-africa.html The drug is authentic exactly. Consistent with the stated prices the Staff is knowledgeable.
Untitled
SCIENTIFIC REPORT A Prospective Study of 2 Sedation Regimens in Children: Chloral Hydrate, Meperidine, and Hydroxyzine Versus Midazolam, Meperidine, and Hydroxyzine Marianne M. Sheroan, DMD, MS, MS,* Diane C. Dilley, DDS,† Warner J. Lucas, DDS, MD,‡ and William F. Vann, DMD, PhD§ *Private practice, Elizabethtown, Kentucky, and part-time faculty member at the University of Louisville School of Dentistry, Louisville, Kentucky; †Department of Pediatric Dentistry and ‡Department of Anesthesiology, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina; §University of North Carolina at Chapel Hill, Chapel Hill, North Carolina. At the time of this investigation, Dr Sheroan was a resident in the Department of Pediatric Dentistry at the University of North Carolina at Chapel Hill, Chapel Hill, North Carolina
The aim of this study was to compare both the behavioral and physiological effectsof 2 drug regimens in children: chloral hydrate (CH), meperidine (M), and hydroxy-zine (H) (regimen A) versus midazolam (MZ), M, and H (regimen B). Patients be-tween 24 and 54 months of age were examined by crossover study design. Behaviorwas analyzed objectively by the North Carolina Behavior Rating System and subjec-tively through an operator and monitor success scale. Physiological data were re-corded every 5 minutes and at critical points throughout the appointment. Sixteenpatients completed this study. No significant differences in behavior were noted bythe North Carolina Behavior Rating System or the operator and monitor successscale. A quiet or annoyed behavior was observed 93% and 90% of the time forregimen A and regimen B, respectively. Using the operator and monitor successscale, 63% of regimen A and 56% of regimen B sedations were successful. Nostatistically significant differences were noted in any of the physiological parametersbetween the 2 regimens. Ten episodes of hemoglobin desaturation were detectedwith regimen A sedations. There were no differences between the sedative drugregimens CH/M/H and MZ/M/H for behavioral outcomes or physiological param-eters. Key Words: Conscious sedation; Midazolam; Chloral hydrate; Children. Behavior management strategies for pediatric dental to 76% of respondents used conscious sedation.2,3 A
patients have evolved greatly over the past 2 de-
recent survey of the American Association of Pediatric
cades, with adverse techniques such as hand-over-
Dentistry members found an increased use of sedation
mouth exercise and hand-over-mouth with airway re-
by pediatric dentists in 2000.4 The popularity of con-
striction having lost considerable popularity.1 In light of
scious sedation among pediatric dentists is underscored
this trend, conscious sedation is a vital dimension of pe-
by the safe and effective means by which sedative drugs
diatric dentistry for those children who fail to cooperate
can be used when practitioners follow the Guidelines
for treatment in a conventional setting. Surveys of pe-
for the Elective Use of Conscious Sedation, Deep Se-
diatric dentists in the mid to late 1980s found that 70
dation, and General Anesthesia in Pediatric Dentist-ry.5,6
One popular drug regimen for the sedation of pedi-
Received April 4, 2005; accepted for publication June 12, 2006. Address correspondence to Marianne Sheroan, 179 Camara Ct,
atric dental patients is a triple-dose cocktail that com-
Elizabethtown, KY 42701; marianne0228@hotmail.com.
bines chloral hydrate (CH), meperidine (M), and hy-
᭧ 2006 by the American Dental Society of Anesthesiology
droxyzine (H). Hasty et al7 reported excellent behavioral
dazolam offers additional advantages over CH with its
outcomes with this regimen and found this combination
anterograde amnesia and the availability of a reversal
to be safe as assessed by pulse oximetery and capnog-
raphy. A more recent and comprehensive retrospective
This prospective study had 2 specific aims. The first
review of 195 pediatric conscious sedations with the
was to compare the behavioral differences resulting
CH/M/H cocktail reported that 72% of the sedations
from the sedative effects of the triple-dose cocktail CH/
were satisfactory and that adverse outcomes were few
M/H versus the regimen MZ/M/H. Behavior was as-
and minor under a strict protocol and use of oxygen
sessed by the objective North Carolina Behavior Rating
supplementation.8 In one retrospective study,9 an 84%
System (NCBRS) and a subjective scale that allows the
success rate was found when the regimen CH/M/H was
operator and the monitor of the sedation to rate the
success of the sedation by using the operator and mon-
Despite the well-researched and documented safety
itor success scale (OMSS). The second aim was to com-
and efficacy of the CH/M/H triple-dose cocktail,7–9
pare the physiological effects of these regimens.
there are well-reasoned concerns with CH as a sedativeagent for children. Laryngospasms, cardiac arrhyth-mias, cardiac arrest, and seizures are among the re-
ported adverse reactions with CH.10–12 An extensive re-
view of adverse events associated with CH administeredduring dental or medical procedures revealed that 5 of
Approval from the University of North Carolina (UNC)
the 13 patients who sustained permanent neurological
Institutional Review Board Committee on Investigations
damage or death were dental patients.13 Incorrect dose
Involving Human Subjects was obtained. The sample
calculations or inadequate communication among the
consisted of 16 children referred for sedation after treat-
dental staff have led to adverse reactions in the dental
ment was unsuccessful in a conventional setting. Patient
age ranged between 24 and 54 months at the time of
One alternative to the use of CH in the triple-dose
the first sedation. All children needed at least 2 sedation
cocktail is midazolam (MZ). Midazolam is a short-act-
appointments of approximately equal length. All chil-
ing benzodiazepine that has been praised for its sed-
dren included in the study had no previous operative
ative, hypnotic, anxiolytic, and anterograde amnesic
dental experience under conscious sedation. Also, all
effects.15–18 Other clinical advantages of MZ include
children met the requirements of the American Society
water solubility, rapid onset, anticonvulsant action,
of Anesthesiologists Class I anesthesia risk. Any children
clinically inactive metabolites, and high margin of
with tonsils greater than ϩ2 according to Brodsky’s
safety.15–18 Marshall et al19 reported that the MZ oral
Tonsil Classification System25 were excluded from the
syrup was accepted by 99% of all children studied.
This formulation was found to be safe and effective
Sample size was calculated on a 2-sample comparison
over a fourfold dose range. Eighty-one percent of the
of proportions of the quiet and annoyed behaviors used
children reached adequate sedation after only 30 min-
in the NCBRS in a previous sedation study that assessed
utes. Nathan and Vargas20 found that when MZ was
both physiological and behavioral parameters in 10 sub-
combined with the narcotic M, there was an 80% suc-
jects.7 Power was set at 0.90 with  ϭ 0.10 and ␣ ϭ
cess rate for children. Moreover, no episodes of per-
0.05, yielding an adequate sample size of 16.
sistent hemoglobin desaturation, loss of protective re-
Informed consent was obtained for the dental treat-
flexes, respiratory depression, or emesis were report-
ment; sedation; and use of physical restraint, videotap-
ing, and participation in this investigation. Parents were
Studies directly comparing CH and MZ provide sup-
instructed with preappointment procedures and post-
port for the use of MZ as a good substitute for CH.
operative instructions after the sedation appointment.
Differences in behavior were negligible during sedation
The procedures, possible discomforts or risks, as well as
procedures comparing the 2 drugs.21 Haas et al22 con-
possible benefits were explained fully to the legal guardians
cluded that patients receiving oral MZ had an increased
of the human subjects involved, and their informed con-
level of sedation before the administration of local an-
sent was obtained before the start of the investigation.
Postsedation complications may be enhanced in CH
Sedation Appointment
sedations by the extended duration (4–8 hours) and betaelimination half-life of the active metabolite trichloroeth-
The conventional oral triple-dose cocktail (regimen A)
anol (8–11 hours) as compared with the shorter dura-
included 50 mg/kg CH (Pharmaceutical Basics Inc,
tion (2–6 hours) and half-life (1–4 hours) of MZ.23,24 Mi-
Morton Grove, Ill), 1.5 mg/kg M (Demerol, Winthrop-
Table 1. North Carolina Behavior Rating System
Quiet: patient quiet or sleeping with only extraneous, inconsequential movements
Annoyed: patient cooperative for treatment but with 1 or 2 of the undesirable behaviors*
Upset: patient noticeably disturbed, with 2–3 undesirable behaviors* present, making treatment difficult but possible
Wild: patient extremely defiant with presence of all undesirable behaviors,* making treatment extremely difficult
* An undesirable behavior consists of crying, screaming, head movement, torso movement, or foot movement.
Breon, New York, NY), and 25 mg H (Vistaril, Pfizer
sal cannula (Salter Labs, Arvin, Calif) at 3.0 L/min
Laboratories, New York, NY). The experimental group’s
triple cocktail (regimen B) included 1.0 mg/kg MZ(Versed, Roche Pharmaceuticals, Nutley, NJ; UNC Hos-
Behavioral Assessment
pital’s Pharmacy), 1.0 mg/kg M, and 25 mg H.20 The
All sedation appointments were videotaped with a video
fixed dose of 25 mg H was used in accordance with the
camera (RCA VHS-C 3-in LCD AutoShot Camcorder,
drug regimen followed in the Pediatric Sedation Clinic
Indianapolis, Ind). Taping commenced from the time the
patient entered the operatory until the time the patient
A crossover study design was used wherein each pa-
left the operatory. Tapes were identified by a randomly
tient served as his or her own control. Each patient was
assigned 3-unit code consisting of 1 letter and 2 num-
assigned randomly to receive 1 of the 2 drug regimens
bers. A blinded, calibrated rater scored each tape by
for the initial sedation appointment, with the other reg-
using the NCBRS (Table 1) as described by Chambers
imen administered at the second appointment. Regi-
et al.28 Undesirable behaviors were defined as crying,
mens were administered by the principal investigator via
screaming, head movement, torso movement, or foot
medicine cup or oral syringe. The principal investigator
movement. Behaviors were assessed throughout the ap-
was in the sedation room if the regimen administered
pointment in 5 discrete time intervals: the preoperative
needed to be revealed for emergency purposes. The op-
period, the local anesthetic period, the rubber dam
erator, monitor, and assistant were blinded to the regi-
placement period, the operative period, and the post-
men being used. Monitors were board-certified pediatric
operative period. The rater was trained and calibrated
dentists with extensive experience in conscious sedation
by assessing 5 videotaped sedations 3 times each to de-
termine his or her success in recognizing each of the
One hour after regimen A was administered or 30
behaviors. After practice and calibration, the rater as-
minutes after regimen B was administered, all patients
sessed the study videotapes in a random order.
were separated from their parents and transferred to the
The OMSS was created by the authors of this study
dental operatory and placed in a Papoose Board (Olym-
to subjectively assess behavior (Table 2). This 4-point
pic Medical Group, Seattle, Wash). Because the purpose
scale ranged from ‘‘successful’’ to ‘‘unsuccessful,’’ de-
of this study was to compare these regimens at each
pending on how the patient’s behavior affected the pro-
individual patient’s optimal sedative effect, the different
start times were necessary because the optimal workingtime of MZ is much shorter than the working time ofM. A shoulder roll was placed under the patient’s neck
Physiological Assessment
and shoulders to aid in maintaining a patent airway.
All patients were monitored with a pulse oximeter, cap-
Supplemental oxygen (100%) was administered via na-
nograph, and a precordial stethoscope. A precordial
Table 2. Operator and Monitor Success Scale
Successful: patient slept throughout procedure with minimal crying or movement at critical events*
Moderately successful: successful sedation with moderate amounts of crying and movement at times other
than critical events,* but behavior did not hinder progress of sedation
Mildly successful: treatment was accomplished as planned, but because of screaming or combative move-
ments throughout the sedation the progression of portions of the treatment was hindered
Unsuccessful: continuous crying or movement throughout sedation; treatment was performed with difficul-
ty; the progression of all treatment was hindered
* Critical events include topical placement, penetration of the needle, rubber dam placement, and burr initially touching first
stethoscope was placed to the left of the sternum to
tinuous data. Because the signed-rank test assumes no
monitor heart and breath sounds. A pulse oximeter
period effect, a Wilcoxon 2-sample test was used to de-
probe BCI sensor (BCI International, Waukesha, Wis)
termine if the order of the sedations significantly affect-
was placed on the great toe of the left foot. Carbon
ed behavior or any of the physiological parameters. The
dioxide monitoring was performed with the BCI Inter-
level of significance was set at ␣ ϭ 0.05 for all statistical
national 9000 Capnograph/Oximeter Monitor (BCI In-
Heart rate (HR), respiratory rate, oxyhemoglobin sat-
uration (SpO ), and end-tidal carbon dioxide (EtCO )
were recorded at 5-minute intervals throughout the en-tire sedation procedure with a time-based anesthesia
Thirteen girls and 3 boys completed the study. The av-
record. Additionally, physiological data were recorded
erage age of the patients at the time they received reg-
at critical events: the placement of topical anesthetic,
imen A (CH/M/H) was 42.8 months (range 27–54
penetration of the needle into mucosa, placement of the
months), whereas the average age of the patients at the
rubber dam, and initial burr contact with the first tooth
time they received regimen B (MZ/M/H) was 43.2
months (range 27–55 months). The average weight of
The individual dedicated to monitor the patient alert-
the regimen A group was 15.4 kg (range 12.7–19.55
ed the operator to respiratory compromise when the
kg), whereas the average weight of the regimen B group
pulse oximeter read below 90% SpO for longer than
15 seconds (true hemoglobin desaturation) or when thecapnograph read 0 for respiratory rate and EtCO or
no visual signs of breathing and no audible breath
Behavioral Findings
sounds via the precordial stethoscope were detected forlonger than 15 seconds (true apnea). Any desaturation
The reliability at the beginning of the study was high
or apneic event accompanied by crying or movement
(Ͼ95%) for all 4 behaviors. Within- and between-data
was not recorded as a true event. If an apneic event or
set reliability remained greater than 95% throughout the
desaturation occurred, the operator was instructed by
study for the quiet, annoyed, and upset behaviors. Al-
the monitor to reposition the child’s head. Operative
though within-data set reliability remained above 95%,
procedures were instructed to stop until the vitals re-
the percentage reliability of recognizing a wild behavior
in between-data sets fell to a low 74% throughout thecourse of the study. This lower reliability was attributedto the low prevalence of the wild behavior in the vid-
Data Analysis
As previously stated, 5 tapes of typical sedation appoint-
To facilitate statistical analysis, all behaviors were con-
ments were viewed 3 times to evaluate the reliability of
verted from seconds of time to percentages of the total
the behavior rater. For calibration and intraexaminer re-
time. At the first sedation appointment, 9 patients re-
liability determinations, the sedation appointment was
ceived regimen A and 7 received regimen B. A. Wil-
not divided into discrete time blocks. Calibration ses-
coxon 2-sample rank sum test confirmed that the se-
sions occurred at the beginning of the study, after view-
dation appointment order had no effect on any behav-
ing half of the tapes, and at the study’s conclusion. The
ioral or physiological parameters (P Ͼ .05).
time each patient spent exhibiting 1 of the 4 behavior
No significant difference in behavior was observed be-
types was converted into percentages.
tween regimen A and regimen B (P Ͼ .05) during any
Reliability was based on a random effects model as
of the individual time blocks or for the overall sedation
described by Neter29 and utilized in the sedation study
(Table 3). When administered regimen A, the patients
performed by Hasty et al.7 When the ratio is converted
spent an average of 93% of the overall sedation ap-
into percentages, perfect reliability is indicated by
pointment exhibiting either a quiet or annoyed behavior,
100%. Reliability near 80% is considered good.
whereas with regimen B this percentage average was
Because of the paired nature of the study design, the
90%. Because a rubber dam was not used in all oper-
small sample size, and the data’s nonnormal distribu-
ative procedures, only 13 pairs of patients could be eval-
tion, a Wilcoxon matched pairs signed-rank test was
uated during the rubber dam isolation time block (what
used to determine the differences in behavior and phys-
procedures were to be performed and the operative
iological readings between the 2 treatment groups. This
protocol were dictated by the operator and attending
test was used additionally to analyze differences in the
faculty member, not the investigator). During 3 proce-
OMSS because it is based on a scale rather than con-
dures, rubber dam isolation was attempted, but cotton
Table 3. Mean Percentage of Time Spent Exhibiting Each Behavior*
Ͻ0.01/0.4
Ͻ0.01/0
* Wilcoxon matched pairs signed-rank test. A indicates regimen A (chloral hydrate/meperidine/hydroxyzine); B, regimen B
roll isolation had to be used because of the state of the
the lower SpO level in patients who received regimen
A was statistically significant (P ϭ .01), this value had
As illustrated in the Figure, 10 of the 16 patients who
no clinical or practical significance.
received regimen A received a score of 1 or 2 according
Ten episodes of SpO desaturation occurred in 2 pa-
to the OMSS. Nine of the 16 patients who received
tients who received regimen A, whereas no desatura-
regimen B received a score of 1 or 2. In 7 patients,
tions occurred with regimen B sedations. No apneic
regimen A sedations received a better success score
events occurred in patients receiving either regimen. No
than the experimental group sedations. Regimen B se-
desaturation fell below 85%. After head repositioning
dations received a better success score than regimen A
by a chin lift, SpO immediately returned to above 90%.
sedations in 3 patients. No difference was noted in the
No desaturation event exceeded 25 seconds. No phys-
success of the 2 sedation combinations in 6 patients.
iological signs of hypoxemia, such as blue skin, were
These findings were not statistically significant (P Ͼ
DISCUSSION Physiological Findings
There were no significant differences (P Ͼ .05) in any
Individual practitioners have a professional duty to know
physiological parameters for the overall sedation time
the effects of all drugs that are administered to patients.
between the 2 drug regimen groups (Table 4). Regimen
Many authors have chronicled the dangers of conscious
B patients had a tendency to exhibit higher HRs during
sedation when proper monitoring, dosages, and strict
rubber dam clamp placement (140.68 beats/min) and
procedural protocols are not followed.13,30 A review of
at the moment of initial burr contact (140.76 beats/
adverse sedation events in pediatric medicine and den-
min). These values were above a normal range for chil-
tistry performed by Cote et al13 points to a dispropor-
dren 2–5 years of age (80–135 beats/min).30 Although
tionately high number of adverse events occurring in pa-tients under the care of ‘‘dental specialists.’’ This reviewhighlights concern with CH when administered outsideits recommended dose range of 50–100 mg/kg, whengiven at home, when administered by a technician, andafter premature discharge of the patient because of thisdrug’s extended half-life.13
Many investigation endeavors have focused on pa-
rameters for minimizing the adverse physiologicalevents associated with CH/M/H while maximizing thesuccess of sedations.7–9,26,27 The thrust of this investi-gation was to explore an oral drug regimen that substi-tuted MZ for CH in the triple-dose cocktail approach.
Operator and monitor success scale (P ϭ .27).
This substitution was chosen because MZ provides pa-
Table 4. Mean Physiological Data†
† A indicates regimen A (chloral hydrate/meperidine/hydroxyzine); B, regimen B (midazolam/meperidine/hydroxyzine). * P Ͻ .05; Wilcoxon matched pairs signed-rank test.
tients with anterograde amnesia, a quicker recovery,
in a Papoose Board, movements of the torso may have
and a reversal agent. The oral dosage of 1.0 mg/kg M,
been more difficult to visualize in a recorded videotape.
1.0 mg/kg MZ, and 25 mg/kg H was based on a ret-
Movements of the head may have been more difficult
rospective study by Nathan and Vargas,20 which found
to visualize if uncooperative behaviors forced the oper-
the combination of 1.0 mg/kg M and 1.0 mg/kg MZ
ator to firmly hold the patient’s head. Finally, if a patient
to maximize effectiveness with minimal physiological ad-
was extremely vocal during the length of operative pro-
cedures, the operator and monitor may have rated thesedation in a more negative manner, even if the childremained still and operations proceeded with ease. In
Behavioral Findings
any case, the videotaped behavioral assessments were
This study design permitted an objective behavior as-
judged to be by far the most valid and reliable tool for
sessment with a blinded, calibrated rater using the
NCBRS. Patients sedated with regimen A (CH/M/H)and regimen B (MZ/M/H) exhibited either a quiet or an
Physiological Findings
annoyed behavior during 93% or 90% of the overallsedation, respectively. These findings are comparable
No significant differences were found between the 2
with those of Hasty et al,7 who found that a quiet or
drug regimens in any of the physiological parameters
annoyed behavior ranged between 82 and 96% of the
for the overall sedation time. Although regimen A had
a significantly lower SpO during topical placement, this
There was no difference in comparing the 2 regimens
finding had no clinical or practical significance because
according to the subjective OMSS. Sixty-three percent
an SpO value of 98% falls within acceptable limits. Ten
(10/16) of the patients who were administered regimen
episodes of hemoglobin desaturation occurred in 2 pa-
A experienced a sedation that was considered successful
tients who received regimen A. These episodes did not
or moderately successful. Fifty-six percent (9/16) of pa-
exceed 25 seconds in either patient, and the oxygen
tients who were administered regimen B achieved the
saturation for the overall sedation remained within an
same level of success. Previous studies examining the
acceptable range. This finding was not surprising be-
drug combination CH/M/H report successes ranging
cause intraoperative desaturations are not uncommon
from 72 to 100%, as assessed by the operators.7–9 The
events in conscious sedations involving CH/M/H.7,26,27
lower success noted in our study may be attributed to
Factors involved in hemoglobin desaturation include air-
the specificity of the OMSS rather than limiting those
way control, drug selection, dosage, lidocaine adminis-
involved in the sedation to chose a simplistic successful
tration, and tonsil size.7,31–34 No desaturation events
or unsuccessful rating for the sedation.
were noted with regimen B, which mirrors a earlier
Although the OMSS represents a completely different
method of assessing behavior from the NCBRS, there
Despite the fact that intraoperative desaturations
appears to be a discrepancy in how the operator and
commonly occur during conscious sedations, desatura-
monitor perceived the sedations compared with the in-
tion events should not be overlooked as an unimportant
dependent rater. This difference might have resulted
finding. In our study, 2 of the 16 children who received
from several factors. Because patients were restrained
the CH cocktail experienced desaturation events. Dur-
ing dental procedures, the operator may unknowingly
tiple extemporaneous formulations. Roche Pharmaceu-
apply pressure to the mandible, forcing the mandible to
ticals recalled this product in 2002 because of a man-
the child’s chest and minimizing the available airway. In
ufacturing difficulty that produced a supernate in a few
our study, simply repositioning the mandible quickly in-
lots, rendering some doses subsaturated and other doses
creased oxygen saturation levels. However, when an in-
supersaturated (from a letter sent to health care profes-
dividual practitioner chooses to perform conscious se-
sionals from Roche Laboratories, February 28, 2002).
dation procedures, he or she must have proper ad-
At that time, the MZ used in this study was obtained
vanced training in sedation and anesthesia and have the
from UNC Hospital’s pharmacy. The UNC Hospital’s
proper monitors and life-support training, such as the
formulation is made from the injectable solution of MZ,
Pediatric Advanced Life Support course offered by the
Syrpalta (sucrose, water, and glycerin), and citric acid
American Heart Association. During our study, the ad-
calibrated to a pH of 4.2 (UNC Hospital’s Drug Infor-
ministrator of the drug regimens was in the sedation
mation Center, oral communication, February 4, 2003).
room in case the drug regimen that was given needed
The Roche formulation of Versed syrup contained sor-
to be revealed to administer emergency medicines.
bitol, glycerin, citric acid, sodium citrate, sodium ben-
Emergency equipment such as positive pressure masks
zocaine, and other dyes and sweeteners calibrated to a
and even intubation equipment was available if needed.
pH of 3.0.37 Differences in pH may have resulted in
A tendency toward an increased HR was noted in reg-
differences in the solubility of MZ. Because of the small
imen B patients when the rubber dam clamp and the
number of regimen B patients who received the com-
burr first contacted a tooth. When MZ alone was used
mercial syrup versus the UNC formulation, we could not
in other sedation studies, a clinically insignificant in-
analyze behavioral or physiological differences that may
creased HR was noted.9,35 It is not possible to differen-
have been secondary to the variation in formulations.
tiate between an increased HR secondary to the drug
Future research efforts should focus on the efficacy of
regimen and an increase due to increased disruptive be-
the MZ cocktail with lower doses of MZ.
haviors at the points in time in which the readings oc-curred. Although no significant differences were noted
CONCLUSIONS
in behavior during the rubber dam placement or oper-ative time blocks, behavior was rated over a course of
In this study, regimen A included CH (50 mg/kg), H (25
time rather than at a specific point in time. Of critical
mg), and M (1.5 mg/kg), and regimen B included MZ
importance was the average HR for the overall sedation,
(1.0 mg/kg), H (25 mg), and M (1.0 mg/kg). Under the
which reflects the average of multiple readings through-
conditions of this study, (a) there were no differences in
out the course of the sedation. This fell within the nor-
behavior between the 2 drug regimens as measured ob-
mal range of 85–135 beats/min for children between 2
jectively by the NCBRS or subjectively by the OMSS; (b)
there were no statistical differences during the overallsedation for any of the measured physiological param-
Concerns With MZ
eters; and (c) 10 desaturation events occurred for pa-tients who received regimen A, whereas no events oc-
Although MZ has been administered orally for a long
curred for patients who received regimen B.
time, studies performed to determine the pharmacoki-netics of a single dose of this drug yielded inconsistentresults because the oral formulation was produced by
ACKNOWLEDGMENTS
individual pharmacies.15 Acidic conditions between 2.8and 3.6 pH provide optimal conditions to solubilize MZ
This investigation was supported by MCH grant 2 T17
in solution. Under these conditions, MZ exists in equi-
MC0015-11 and by the AAPD Foundation and OMNII
librium between the active closed-ring form and the in-
Pharmaceuticals through the OMNII Fellowship pro-
active open-ring form of this drug. After ingestion, the
gram. The authors express their appreciation to Mrs
pH rises above 5.0 and the equilibrium shifts, allowing
Jennifer Mann—our blinded, calibrated rater—for her
the absorption of MZ in the active closed-ring form.37
hours of dedication to this study and to Doctoral Can-
The additions of sweeteners or juices by individual phar-
didate Lan Kong and the UNC Biometrics Laboratory
macies may change the pH of the solution, leading to
of the UNC School of Public Health, Chapel Hill, NC.
various degrees of MZ that are soluble in that formula-tion. Because of these differences, the pharmacokinet-
REFERENCES
ics would change from formulation to formulation.
In 1998, MZ became commercially available as an
1. Carr KR, Wilson S, Nimer S, Thornton JB Jr. Behavior
oral syrup, eliminating the guess work concerning mul-
management techniques among pediatric dentists practicing in
the southeastern United States. Pediatr Dent. 1999;21:347–
19. Marshall J, Rodarte A, Blumer J, Khoo KC, Akbari B,
Kearns G. Pediatric pharmacodynamics of midazolam oral syr-
2. Davis MJ. Conscious sedation practices in pediatric
up. Pediatrics. 2000;40:578–589.
dentistry: a survey of members of the American Board of Pe-
20. Nathan JE, Vargas KG. Oral midazolam with and with-
diatric Dentistry College of Diplomates. Pediatr Dent. 1988;
out meperidine for the young pediatric dental patients. Pediatr
3. Houpt M. Project USAP the use of sedative agents in
21. Feld LH, Negus JB, White PF. Oral midazolam prean-
pediatric dentistry: 1991 update. Pediatr Dent. 1993;15:36–
esthetic medication in pediatric outpatients. Anesthesiology.
4. Houpt M. Project USAP 2000—use of sedative agents
22. Haas DA, Nenniger SA, Yacobi R, et al. A pilot study
by pediatric dentists: a 15-year follow-up survey. Pediatr
of the efficacy of oral midazolam for sedation in pediatric den-
tal patients. Anesth Prog. 1996;43:1–8.
5. Saxen MA, Wilson S, Paravecchio R. Anesthesia for
23. Oertel M, ed. UNC Drug Formulary 1998/1999. Hud-
pediatric dentistry. Dent Clin North Am. 1999;43:231–245.
son, Ohio: Lexi-Comp Inc; 1998:182–183.
6. Ad Hoc Committee on Sedation and Anesthesia.
24. Oertel M, ed. UNC Drug Formulary 1998/1999. Hud-
Guidelines for the elective use of conscious sedation, deep se-
son, Ohio: Lexi-Comp Inc; 1998:576–578.
dation and general anesthesia in pediatric dentistry. Pediatr
25. Brodsky L. Modern assessment of tonsils and adenoids. Pediatr Clin North Am. 1989;36:1551–1568.
7. Hasty MF, Vann WF Jr, Dilley DC, Anderson JA. Con-
26. Leelataweewud P, Vann WF Jr, Dilley DC, Lucas WJ.
scious sedation of pediatric dental patients: an investigation of
The physiological effects of supplemental oxygen versus ni-
chloral hydrate, hydroxyzine pamoate, and meperidine vs.
trous oxide/oxygen during conscious sedation of pediatric den-
chloral hydrate, and hydroxyzine pamoate. Pediatr Dent.
tal patients. Pediatr Dent. 2000;22:125–133.
27. Rohlfing GK, Dilley DC, Lucas WJ, Vann WF Jr. The
8. Leelataweewud P, Vann WF Jr. Adverse events and out-
effect of supplemental oxygen on apnea and oxygen saturationduring pediatric conscious sedation. Pediatr Dent. 1998;20:
comes of conscious sedation for pediatric patients: using chlo-
ral hydrate, meperidine, and hydroxyzine pamoate with O2
28. Chambers WL, Fields HW, Machen JB. Measuring se-
supplementation. J Am Dent Assoc. 2001;132:1531–1539.
lected disruptive behaviors of the 36 to 60 month-old patient.
9. Wilson S, Easton J, Lamb K, Orchardson R, Cassa-
Part 1: development and assessment of a rating scale. Pediatr
massimo P. A retrospective study of chloral hydrate, meperi-
dine, hydroxyzine, and midazolam regimens used to sedate
29. Neter J. Applied Linear Statistical Models. 2nd ed.
children for dental care. Pediatr Dent. 2000;22:107–113.
Homewood, Ill: Irwin Press; 1985:643–647.
10. Granoff DM, McDaniel DBL, Borkowf SP. Cardiore-
30. Goodson JM, Moore PA. Life-threatening reaction after
spiratory arrest following aspiration of chloral hydrate. Am J
pedodontic sedation: an assessment of narcotic, local anes-
Dis Child. 1971;122:170–171.
thetic, and antiemetic drug interaction. J Am Dent Assoc.
11. Rokicki W. Cardiac arrhythmia in a child after the usual
dose of chloral hydrate. Pediatr Cardiol. 1996;17:419–420.
31. Moore PA, Mickey EA, Hargreaves JA, Needleman
12. Munoz M, Gomez A, Soult JA, et al. Seizures caused
HL. Sedation in pediatric dentistry: a practical assessment pro-
by chloral hydrate sedative doses. J Pediatr. 1997;131:787–
cedure. J Am Dent Assoc. 1984;109:564–569.
32. Moore PA. Local anesthesia and narcotic drug inter-
13. Cote CJ, Karl HW, Notterman DA, Weinberg JA, Mc-
action in pediatric dentistry. Anesth Prog. 1988;35:17.
Closkey C. Adverse sedation events in pediatrics: analysis of
33. Allen GD. Diagnosis and treatment of respiratory prob-
medications used for sedation. Pediatrics. 2000;106:633–
lems in sedation and anesthesia for dentistry. Anesth Prog.
14. Hayden J Jr. Chloral hydrate as a sedative in dentistry.
34. Verwest TM, Primosch RE, Courts FJ. Variables influ-
J Colo Dent Assoc. 1982;61:3–4.
encing hemoglobin oxygen desaturation in children during rou-
15. Payne K, Matheyse FJ, Liebenberg D, Dawes T. The
tine restorative dentistry. Pediatr Dent. 1993;15:25–29.
pharmacokinetics of midazolam in paediatric patients. Eur J
35. Silver T, Wilson C, Webb M. Evaluation of two dosages
Clin Pharmacol. 1989;37:267–272.
of oral midazolam as a conscious sedation for physically and
16. Singh N, Pandey RK, Saksena AK, Jaiswal JN. A com-
neurologically compromised pediatric dental patients. Pediatr
parative evaluation of oral midazolam with other sedatives as
premedication in pediatric dentistry. J Clin Pediatr Dent.
36. Anderson J. Physiologic principles in pediatric dentist-
ry. In: Pinkham JR, ed. Pediatric Dentistry: Infancy Through
17. Kain ZN, Hafstadter MB, Mayes LC, et al. Midazolam. Adolescence. 2nd ed. Philadelphia, Pa: WB Saunders Co;
Anesthiology. 2000;93:676–684.
18. Kupietzky A, Houpt MI. Midazolam: a review of its use
37. Roche Laboratories Inc. Versed—complete product in-
for conscious sedation of children. Pediatr Dent. 1993;15:
formation. Available at: http://www.rocheusa.com/products/
versed/pisyr.html. Accessed February 16, 2003.
CURRICULUM VITAE Thomas N. Hangartner, PhD, FAAPM 4058 Whitegate Dr. Beavercreek, Ohio 45430 Phone H: (937) 427-2177 Phone W: (937) 775-5070 PERSONAL INFORMATION: EDUCATION: Matriculation,Stiftsschule Einsiedeln, SwitzerlandDipl. Phys. ETH,Swiss Federal Institute of Technology, ZürichTeaching Certificate (Secondary Education),Swiss Federal Institute of Technology, Züric
THIS YEAR’S TOPICS: • Concussions – Lessons from the NFL • POST/Palliative Care • Pediatric Trauma – Myths & Metaphors • National ACEP Update • Opiate Perspective • Left Ventricular Assist Devices • Tranexamic Acid • Anticoagulants/Rescue • Ultrasound Skills That Can Change Your Practice • Indiana Legislation – Impact on EPs T
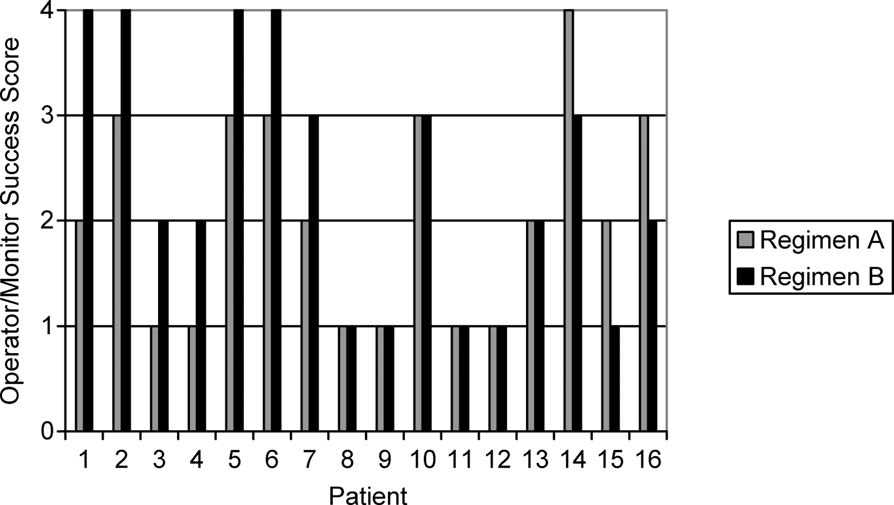 Table 3. Mean Percentage of Time Spent Exhibiting Each Behavior*
Table 3. Mean Percentage of Time Spent Exhibiting Each Behavior*