Thank you, it's cool. Used for the first time because only then was the right drug. Very revealing detail: ordered Express shipping to get the order within 3 hours because didn't know how to get the order faster https://africarx.co.za/ The drug is authentic exactly. Consistent with the stated prices the Staff is knowledgeable.
Washingtoneye.com
Current management of glaucoma Kenneth Schwartza and Donald Budenzb Purpose of review Introduction
This study reviews current concepts in the goals of glaucoma
The management of glaucoma typically proceeds from
therapy, interventional sequence, and options for the
interventions that are the safest and the least invasive, to
management of glaucoma in light of recent clinical trials.
those that expose the patient to greater risk and are the
Recent findings
most invasive. Glaucoma therapy involves medicines, la-
Recent randomized prospective trials of ocular hypertension
and glaucoma have provided evidence for more specifictreatment goals in glaucoma therapy. In addition, the advent of
Treatment modality follows diagnosis, and the type and
the prostaglandin analogs, advances in laser technology, and
severity of disease must be determined before an appro-
innovative techniques for filtering surgery have expanded the
priate intervention can be selected. Recent, large, pro-
armamentarium that ophthalmologists use in the treatment of
spective studies have examined more closely the role of
intraocular pressure (IOP) lowering in the prevention of
progression of glaucomatous disease. The Collaborative
Despite continued advances in laser and incisional surgery,
Normal Tension Glaucoma Study, Advanced Glaucoma
medical therapy still appears to be the primary means by which
Intervention Study, Collaborative Initial Glaucoma
intraocular pressure is controlled. Initial medical therapy has
Study, Ocular Hypertensive Treatment Study, and the
changed with the introduction of prostaglandin analogs, which
Early Manifest Glaucoma Treatment Study all provide
are replacing -antagonists as the drug of first choice. Laser
evidence that reduction of IOP reduces the rate of dis-
trabeculoplasty, using either photocoagulative (argon and
diode) or photodisruptive (frequency doubled Nd:YAG) lasers,is still reserved for patients who do not improve with medical
Goals of glaucoma therapy
therapy, although there is good evidence that initial laser
The goal of glaucoma therapy in ocular hypertension is
trabeculoplasty is just as effective as initial medical therapy.
to lower IOP by at least 20% in patients at moderate to
Trabeculectomy with antifibrotic agents (5-fluorouracil or
high risk. In patients with perimetry-proven glaucoma,
mitomycin C) is still the next step in intraocular pressure
IOP should be lowered by at least 30% in early to mod-
control, and glaucoma drainage implants are reserved for
erate glaucoma, and perhaps 40% to 50% in severe
refractory cases. Cyclophotocoagulation is a last resort
glaucoma. A number of prospective, randomized clinical
procedure because of poor visual outcomes and is reserved
trials, including the Collaborative Normal Tension Glau-
for patients with intractable pain and vision thought not to be
coma Study [1,2], Advanced Glaucoma Intervention
Study [3], Collaborative Initial Glaucoma Study [4], Ocu-lar Hypertension Treatment Study [5••], and Early
Keywords
Manifest Glaucoma Study [6••] provide evidence that
glaucoma, prostaglandin, SLT, filtering surgery
the above treatment parameters may be useful in settingthe initial IOP goal in patients with glaucoma. However,
Curr Opin Ophthalmol 15:119–126. 2004 Lippincott Williams & Wilkins.
because of individual variability in susceptibility to dam-age of the optic nerve, continued vigilance for progres-sion, using automated static perimetry and optic nervestereo photography, is necessary to determine whether
individual patients will progress at the initial target IOP
The Georgetown University Hospital/Washington Hospital Center Washington,
DC, and bBascom Palmer Eye Institute, University of Miami School of Medicine,
[7]. Visual fields and optic nerve photos should be moni-
tored for signs of change, and IOP should be lowered an
Correspondence to Donald L. Budenz, MD, 900 NW 17th Street, Miami, FL
additional 15% if progression is detected [7].
33136, USATel: 305 326 6384; fax: 305 326 6337; e-mail: dbudenz@med.miami.edu
Glaucoma management options Current Opinion in Ophthalmology 2004, 15:119–126 Medical therapy
2004 Lippincott Williams & Wilkins
There are three general categories of management op-
tions available for IOP lowering. Each has been shown tobe effective in lowering IOP and preventing glaucomaprogression. Most clinicians begin with medical therapy,then go on to laser surgery, and finally perform surgery if
Glaucoma
the IOP is not adequately controlled [Fig. 1]. This step-
Table 2. Relative monotherapy efficacy and approximate
wise approach reflects the safety and efficacy of these
percentage intraocular pressure lowering of currently available topical glaucoma medications
treatments, although several clinical trials have studiedusing laser first [8] or incisional surgery first [4,9], and
have gotten comparable results to medicine first.
Table 1 shows the available classes of medication used
for chronic management of glaucoma. All work by low-
ering IOP, either by improving aqueous humor outflow
or reducing its production [10]. The exact mechanismsby which this is accomplished may differ between
tions in that class group. There are conflicting data in the
classes. For instance, prostaglandin derivatives improve
literature regarding differences in efficacy between la-
aqueous outflow primarily through the uveoscleral path-
tanoprost and bimatoprost. Several studies have shown a
way, whereas cholinergic agonists exert their effect on
minor (0.5 to 2 mm Hg) difference in IOP-lowering ef-
the trabecular meshwork outflow system exclusively.
fect in favor of bimatoprost [17–19•], although all butone of these [19•] failed to show a statistically significant
The osmotic agents (mannitol, glycerin, urea) are in-
difference with properly performed statistical analyses.
cluded in the interest of completeness. These potent
An initial report on travoprost purported a better re-
agents are used in two situations: (1) in the acute man-
sponse to travoprost than latanoprost in black subjects
agement of elevated IOP (such as acute angle closure
[20]. However, this was true at only a few time points,
glaucoma), or (2) before incisional surgery where the IOP
and proper statistical analysis of these data, taking into
is elevated or the eye may be open for a long time, to
account differences in baseline IOPs, fails to show a dif-
prevent expulsive suprachoroidal hemorrhage. The
ference in favor of one drug over the other in black pa-
mechanism of action of these drugs, as traditionally
tients [21]. Subsequent studies comparing travoprost and
taught, is to shrink the vitreous by increasing the osmotic
latanoprost or bimatoprost have failed to detect any sta-
gradient between the plasma and the eye, thereby low-
tistically significant differences in response in black sub-
ering the IOP by reducing the volume in the eye. The
jects [22•,23•]. In the only randomized prospective trial
exact mechanism whereby these drugs work is still un-
comparing latanoprost, bimatoprost, and travoprost, no
statistically significant differences in IOP lowering werefound, even in a subanalysis of black subjects [23•]. So,
When prescribing initial medical therapy for glaucoma or
regarding efficacy within the prostaglandin derivative
ocular hypertension, there are a number of factors to
class, the only conclusive studies show that unoprostone
consider. Efficacy, side effects, cost, convenience of dos-
is significantly less effective at lowering IOP than the
ing, and a new possible consideration, differences in di-
other three in this class. Latanoprost, bimatoprost, and
urnal fluctuation, all must be considered. Entire mono-
travoprost appear to have similar efficacy.
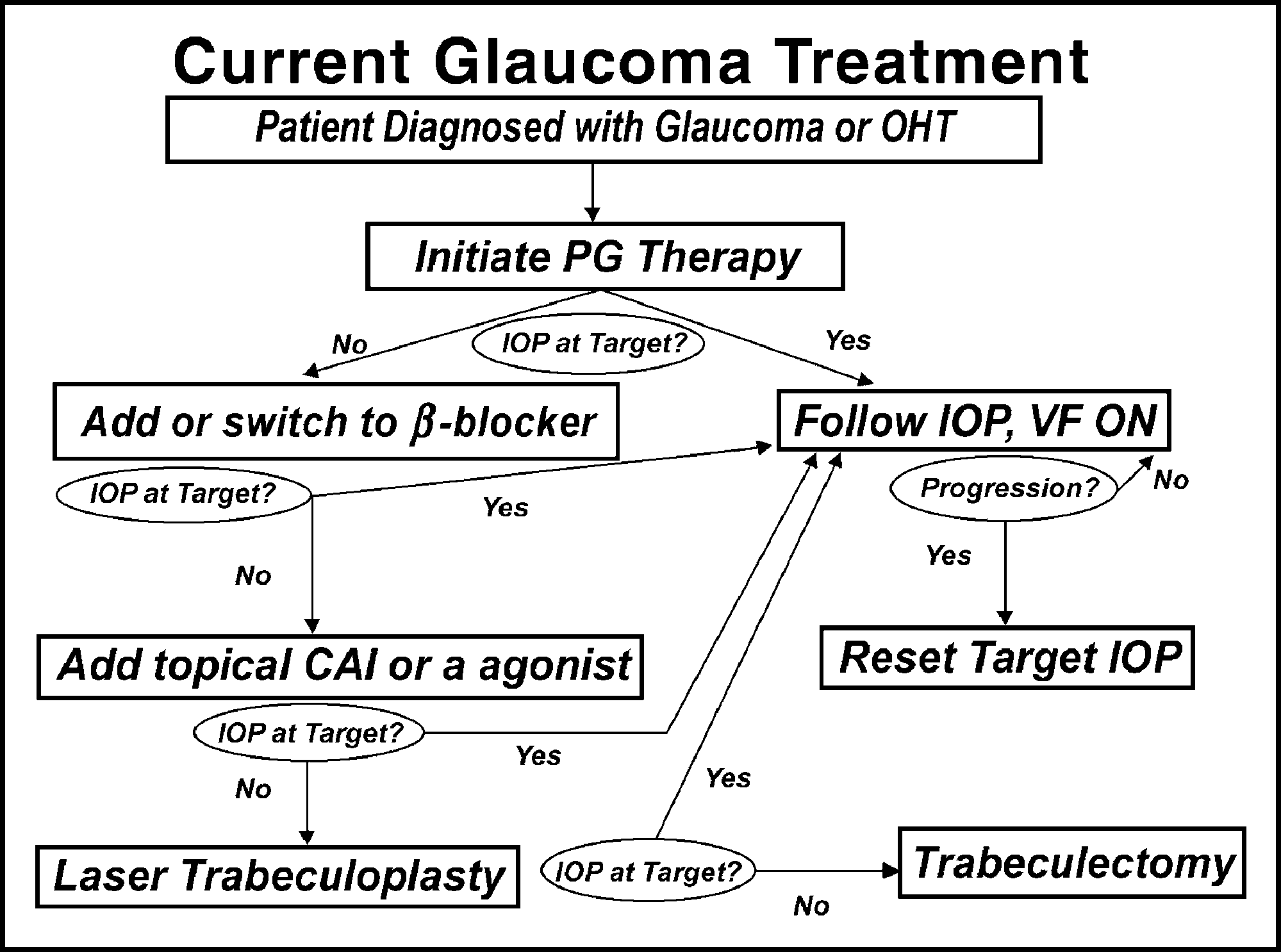
graphs have been written to address these issues [11,12]. Figure 1. Glaucoma treatment decision tree
Table 2 shows the approximate range of IOP loweringthat one may expect based on well-performed controlledclinical trials of these medications. More complete sum-maries are available in the references [11–13,14•]. Classes of medications have been split into individualmedications when appropriate. For instance, betaxolol, a-1 selective -blocker, is not as effective as nonselec-tive -blockers such as timolol or levobunolol. And uno-prostone, a prostaglandin derivative, is less effective thanlatanoprost [15,16•] and, most likely, the other medica-
Table 1. Mechanism of action of glaucoma medications
Treatment options for glaucoma, based on responses. CAI, carbonic anhydrase
inhibitors; IOP, intraocular pressure; OHT, ocular hypertension; ON, optic nerve;
PG, prostaglandin; VF, visual field. Current management of glaucoma Schwartz and Budenz
One important point is that the above efficacies are from
Table 4. Relative frequency/severity of systemic side effects of
clinical trial data from patients with open angle glauco-
current topical glaucoma medications
mas who started with IOPs in the mid to upper 20s. If
one starts with a higher IOP, then percentage lowering
may be more than if one starts at a lower IOP. Also, these
approximations only apply if the medicine is used at the
frequency recommended by the package insert. In par-
ticular, the topical carbonic anhydrase inhibitors and bri-
PG, prostaglandin. Adapted with permission [13].
monidine are labeled as three times daily medicationsbecause twice-daily dosing results in significant trougheffects when used as monotherapy [24–26]. However, in
In general, topical medications for glaucoma are very
combination therapy with a nonselective -blocker,
well tolerated systemically [10]. There are minor differ-
these two medications seem to be equivalent whether
ences, however, in individual medications and in particu-
used twice daily or three times daily.
lar patient groups. For example, nonselective -blockersare usually well tolerated, but may cause an exacerbation
Our decision about which medication to choose for our
of respiratory symptoms in patients with reactive airway
patient is never really based on efficacy alone. Other-
disease (such as asthma) and bradycardia in susceptible
wise, all of our patients with glaucoma would be on sys-
patients. Impotence and decreased exercise tolerance
temic carbonic anhydrase inhibitors! Ocular and systemic
have also been reported with -blockers. Betaxolol, a -1
tolerability, dosing regimen, and cost must be considered
receptor selective antagonist, has fewer respiratory side
effects, although the other side effects mentioned for the-blockers are no less in betaxolol-treated patients. Bri-
Table 3 rates classes of topical glaucoma medications,
monidine has been associated with respiratory and car-
and medications within classes where they differ, on the
diac depression in infants and is contraindicated under
basis of the frequency and severity of ocular side effects
age 2, and caution is indicated in all pediatric patients
[13]. Cholinergic medicines, such as pilocarpine, have
and nursing mothers. Both brimonidine and topical car-
excellent efficacy and cost, but have been largely aban-
bonic anhydrase inhibitors can cause fatigue and drowsi-
doned because of the severity of their ocular side effects
ness in adults (elderly patients are particularly suscep-
compared with newer agents available. Brimonidine has
tible), and thus are not as well tolerated systemically as
a relatively high rate of allergic response, and the dis-
the prostaglandin derivatives and cholinergic agonists. In
continuation rate for this medication because of ocular
addition, many patients complain of a metallic taste per-
adverse events is relatively high compared with the other
version while using topical carbonic anhydrase inhibitors.
medications. In a well-performed 12-month study com-
Table 4 rates the available topical glaucoma agents ac-
paring brimonidine to timolol, the discontinuation rate
was 45% for brimonidine, primarily because of ocularadverse events, compared with only 17% for timolol [26].
Dosing regimen is an important factor in patient compli-ance. Although there is good evidence in the ophthalmicliterature to suggest that compliance is worse with four
Within the prostaglandin derivative class, latanoprost
times daily compared with twice daily dosing regimens
and unoprostone appear to have better ocular tolerability
[27,28], evidence for differences in compliance between
than travoprost and bimatoprost, specifically because of
twice daily and every day dosing is lacking. In fact, a
the higher rate and severity of ocular hyperemia associ-
large review of the literature on compliance with oral
ated with the latter two medications [23]. An excellent
medications found 70% compliance with twice daily or
table comparing the frequency of ocular adverse events
every day dosing [29], compared with 52% for three
reported in the Phase 3 clinical trials on the prostaglan-
times daily dosing and 42% with four times daily dosing.
dins may be found in [12], pages 132 to 133.
Differences in the cost of glaucoma medications aremostly related to the availability of these medicines in
Table 3. Relative frequency/severity of ocular side effects of current topical glaucoma medications
generic form. The nonselective -blockers and choliner-gic agonists have been around for more than 25 years;
thus, generics are available and relatively inexpensive
($0.38 to $0.50 per day for bilateral therapy with generics
vs $0.90 to $1.33 per day for newer agents) [30•]. A ge-
neric form of brimonidine recently became available, and
the cost to pharmacies is approximately half the cost of
the branded formulation [31]. However, it is unclear
Glaucoma
whether pharmacies will pass this cost-savings on to pa-
sources. Phase II of the Ocular Hypertension Treatment
Study has just received funding to try to answer thisimportant issue.
A recent study suggests that high diurnal fluctuation ofIOP, even in treated patients, can result in more progres-
Laser surgery
sion compared with patients who do not show high di-
Laser surgery for open angle glaucoma generally refers to
urnal fluctuations [32]. A subsequent study showed that
laser trabeculoplasty, although endolaser laser photoco-
latanoprost-treated patients show less diurnal variation in
agulation of the ciliary processes has become more
IOP than patients treated with timolol or dorzolamide
widely used in the management of glaucoma. Photoco-
[33]. There is an excellent review on the importance of
agulation of the ciliary processes, using either an endo-
diurnal fluctuation in glaucoma management by Jacob
laser or transscleral technique, has generally been re-
Wilensky, MD, in this edition of Current Opinion in
served for eyes refractory to all other medical or surgical
treatments. Some have advocated endolaser cyclophoto-coagulation as a viable earlier treatment modality [37,38]
Although IOP-lowering therapy medically has been
in developed countries, and others have advocated trans-
shown to be beneficial in delaying or preventing the
scleral cyclophotocoagulation in developing countries
onset of glaucoma in ocular hypertensives and delaying
[39], where healthcare resources do not permit the usual
or preventing visual field loss in those with glaucoma,
stepwise approach to glaucoma management that are
there must be a consideration of the potential downside
available here in the United States and the remainder of
of therapy in general and of specific therapies. For ex-
ample, in a 90-year-old ocular hypertensive patient withno visual field loss, observation to see if the patient de-
Laser trabeculoplasty has been used in the management
velops glaucoma might be better than lowering the IOP
of open angle glaucomas for more than 20 years. Initially
by 20%, especially if your therapy introduces the risk of
performed with the argon blue-green wavelength
ocular or systemic side effects or high medication costs.
[40,41], the same effect may be achieved using argon
At the other end of the spectrum, let’s consider a 60-
green, diode green, and a frequency-doubled Nd:YAG
year-old patient with severe, progressive glaucoma who
laser, known as selective laser trabeculoplasty. There are
has IOPs in the mid-20s on maximal medical therapy and
some advantages to laser trabeculoplasty when compared
has already received laser trabeculoplasty. The risk of
with medical treatment or incisional surgery. It does re-
permanent disability is high without IOP lowering, and
duce IOP in most patients, there is no risk of bleeding or
the benefits of successful trabeculectomy are high. One
infection because it is relatively noninvasive, there is less
would probably be willing to accept the small risk of
dependence on patient compliance to provide IOP con-
complications from trabeculectomy surgery in this case.
trol, and the IOP becomes less susceptible to diurnalvariation [42].
There is some debate as to whether treating IOP earlyprovides more benefit than waiting until one establishes
Laser trabeculoplasty results in an IOP reduction of 20%
that glaucoma is present and, if it is, what the rate of
to 30% in most patients. However, the effect wears off in
progression is. Advocates of early treatment believe that
5% to 10% of patients per year, and the 5-year and 10-
prolonged elevation of IOP triggers a series of events
year success rate is approximately 50% and 32%, respec-
that results in progressive loss of ganglion cells even after
tively [43]. The poor long-term success may be because
IOP is adequately controlled. This hypothesis may ex-
of progression of the disease with worsening IOP or
plain why some patients continue to progress despite
structural changes in the trabecular meshwork over time,
adequate control of IOP [34]. If this is true, it suggests
such as scarring and fusion of trabecular beams [44,45].
early intervention for elevated IOP is necessary. If earlytreatment turns out not to be very important, then wait-
The Glaucoma Laser Trial was a prospective, random-
ing for signs of manifest glaucoma (optic nerve changes
ized study comparing the efficacy and safety of medical
or visual field abnormalities) is a reasonable strategy in
therapy first versus argon laser trabeculoplasty (ALT)
ocular hypertension management. Observing patients
first in the management of glaucoma [8]. In each previ-
with glaucoma for evidence of progression to determine
ously untreated patient, one eye was randomized to ALT
the rate of progression and then tailoring treatment to
first and the other to medical therapy with timolol 0.5%
reduce this rate is a reasonable option. This debate is an
first. Two-year success rates for the Glaucoma Laser
important one in public health circles, because treating
Trial showed a success rate of 44% if eyes were treated
everyone with ocular hypertension is a costly endeavor.
with laser alone, or controlled with a combination of laser
The Framingham Eye Study [35] and The Baltimore
first and any medication at 2 years. This gave support to
Eye Survey [36] found that 4% to 7% of people older
laser therapy when compared with the 30% figure for
than age 40 have elevated IOP; thus, treating all of them
eyes treated with timolol 0.5% alone. Seventy percent of
would place a tremendous burden on health care re-
eyes treated with laser followed by timolol alone had
Current management of glaucoma Schwartz and Budenz
controlled IOP at 2 years, whereas 66% of eyes treated
is fairly limited, even among glaucoma subspecialists.
with a stepwise medical regimen alone were successful at
This is because studies have not shown IOP lowering in
2 years. Eighty-nine percent of patients thought that the
most patients to be as good as trabeculectomy, although
idea of laser trabeculoplasty is a reasonable initial treat-
the complication rate is less [58•,59••]. Glaucoma drain-
age implants have traditionally been reserved for pa-tients who have refractory glaucoma (neovascular, in-
Despite the successful results of laser trabeculoplasty as
flammatory) or those who have not improved with
an initial treatment modality in the Glaucoma Laser
trabeculectomy or have conjunctival scarring from previ-
Trial, members of the American Glaucoma Society (who
ous ocular surgery. Success rates with these devices are
were polled 1 to 2 years after the results of the Glaucoma
comparable to that of trabeculectomy, although there are
Laser Trial were published) were only rarely or never
limited data from randomized prospective trials [60].
performing this procedure as an initial management op-tion [46].
Trabeculectomy has been used for more than 20 yearsfor the surgical management of glaucoma and is currently
Selective laser trabeculoplasty (SLT) is a frequency-
the most widely used incisional procedure worldwide.
doubled Nd:YAG laser that delivers a brief duration (3
When initial trabeculectomy was compared with medical
nS), large spot (400 µm), relatively low-energy (approxi-
therapy in the Collaborative Initial Glaucoma Study, it
mately 0.75 mJ) spot to the trabecular beams [47]. It
was found to provide lower IOPs than medical therapy,
reportedly targets pigmented trabecular meshwork cells,
although the rate of visual field progression was negli-
possibly stimulating them to divide and provide im-
gible in both groups [4]. There was no difference in
proved outflow through the trabecular meshwork [48].
quality of life noted between the initial trabeculectomy
Histologic studies in human cadaver eyes have demon-
versus medical group, either [61]. Other advantages of
strated much less damage to surrounding trabecular
trabeculectomy over medical therapy include stabiliza-
beams with SLT compared with ALT [49]. This may
tion of IOP (minimizing diurnal fluctuation), less reli-
result in improved long-term success and the ability to
ance on patient compliance to take medications, and less
retreat the meshwork in the future with more success
dependence on patient financial resources to stay com-
using SLT compared with ALT. There is a single pro-
spective randomized trial comparing ALT and SLT inthe literature by Damji et al. [50]. In this 6-month trial,they found the same degree of IOP lowering using both
Despite these advantages, in developed countries tra-
lasers, approximately 21%. Just under half of patients in
beculectomy is still performed after medications and la-
each group had already undergone ALT, therefor this
ser surgery have failed. This is probably because of the
group of patients would not be expected to be particu-
risk of immediate visual loss from complications of sur-
larly responsive to further laser treatment.
gery, such as choroidal effusion, hypotony maculopathy,suprachoroidal hemorrhage, or optic nerve snuffing.
In the only published report on SLT used as initial
There are also long-term risks to vision, such as hypotony
therapy for glaucoma, Melamed et al. [51••] found an
maculopathy, bleb infections, and cylindrical changes in
average 30% drop in IOP in the overall group, a number
similar to that obtained with initial medical therapy withprostaglandin derivatives shown in other studies with
Glaucoma drainage implants are most commonly used in
similar baseline IOPs. A randomized prospective trial
patients with glaucoma refractory to trabeculectomy or
comparing initial SLT to initial medical therapy is on-
with neovascular [62,63] or inflammatory glaucomas
[64•]. Recently, however, there has been interest in per-forming glaucoma drainage tube implants as an alterna-
Incisional surgery
tive to trabeculectomy in primary procedures [60]. More
Incisional surgery has traditionally been reserved for pa-
studies are needed to determine the safety and efficacy
tients who do not improve with medical and laser
of glaucoma drainage implants compared directly to tra-
therapy for glaucoma, except in congenital and infantile
glaucomas. Trabeculectomy remains the most commonlyperformed incisional surgery for glaucoma. This may beperformed with antifibrotic agents, such as 5-fluorouracil
Treatment algorithm
or mitomycin C in high-risk patients [53–56]. There is
The figure represents our thought process in treating
reasonable evidence that these agents enhance success
glaucoma. This algorithm is not meant to be a cookbook
in primary filtering surgery (those with no prior incisional
approach to treatment. Rather, it forms the architecture
surgery) [57]. Although deep sclerectomy and viscoca-
of a decision-making tree that must be tempered with
nalostomy (nonpenetrating filtration surgery) have
the individual situation of the patient and an overall ge-
gained popularity overseas, their use in the United States
stalt of the nature of that patient’s disease. Glaucoma
First, the decision to initiate treatment in an ocular hy-
time of trabeculectomy, and which one to choose, is vari-
pertensive patient is variable. This decision is based
able among glaucoma specialists. Most glaucoma special-
upon an individual patient’s risk factors for the develop-
ists are using adjunctive antifibrotic agents at the time of
ment of glaucoma, such as level of IOP elevation, optic
nerve appearance, family history of glaucoma, race, age,central corneal thickness, and the patient’s own prefer-
References and recommended reading
ence for preventative medicine therapy. Generally,
Papers of particular interest, published within the annual period of review,
therapy is initiated with medications, although laser tra-
beculoplasty is a reasonable first-line agent. Of the
classes of medicines available for lowering IOP, the pros-
taglandins have the best balance between efficacy (25%
Collaborative Normal-tension Glaucoma Study Group: Comparison of glau-comatous progression between untreated patients with normal-tension glau-
to 30% lowering), safety, and ease of dosing regimen. If
coma and patients with therapeutically reduced intraocular pressures. Am J
the patient cannot afford prostaglandin therapy, then a
topical -blocker can be started if there are no systemic
Collaborative Normal-tension Glaucoma Study Group: The effectiveness of
contraindications. If only a minimal decrement in IOP is
intraocular pressure reduction in the treatment of normal-tension glaucoma. Am J Ophthalmol 1998, 126:498–505.
seen, the patient is switched to a different class of medi-
The AGIS Investigators: The Advanced Glaucoma Intervention Study (AGIS)
cine, usually the -blockers, because of their efficacy,
7: The relationship between control of intraocular pressure and visual field
tolerability, and ease of dosing. If the IOP does go down
deterioration. Am J Ophthalmol 2000, 130:429–440.
a bit with a prostaglandin, but is not at target IOP, a
Lichter PR, Musch DC, Gillespie BW, et al., for the CIGITS Study Group.:
-blocker is added. Then, if these maneuvers are unsuc-
Interim clinical outcomes in the Collaborative Initial Glaucoma TreatmentStudy comparing initial treatment randomized to medication or surgery. Oph-
cessful, one can add a topical carbonic anhydrase inhibi-
tor, usually in the form of the fixed combination of ti-
Kass MA, Heuer DK, Higginbotham EJ, et al., and the Ocular Hypertension
molol 0.5% and dorzolamide, again attempting to keep
Treatment Study Group. The Ocular Hypertension Treatment Study. A ran-
the dosing regimen simple. If this does not work, the
domized trial determines that topical ocular hypotensive medication delays orprevents the onset of primary open-angle glaucoma. Arch Ophthalmol 2002,
dorzolamide is stopped and substituted with bri-
monidine. Once three or four medicines have been tried
Large, randomized, prospective, multicenter study that examined the effects oftreatment versus nontreatment in ocular hypertensives. The goal in the medication
and the IOP remains refractory, laser trabeculoplasty is
group was to reduce the IOP by 20% or more and to reach an IOP of 24 mm Hg or
performed. If it seems unlikely that laser will make
less. At 5 years, the cumulative probability of developing primary open-angle glau-coma was 4.4% in the medication group and 9.5% in the observation group.
enough of an impact on IOP, trabeculectomy is recom-
Heijl A, Leske MC, Bengtsson B, et al.: Reduction of intraocular pressure and
mended. Usually primary trabeculectomy is completed
glaucoma progression. Results form the Early Manifest Glaucoma Trial. Arch
with intraoperative and possibly postoperative 5-fluoro-
Large, randomized prospective study performed in Sweden to evaluate glaucoma-
uracil, unless the patient has risk factors for scarring, such
tous progression in patients with early manifest glaucoma. Two hundred fifty-five
as young age or prior incisional eye surgery, in which case
patients with open-angle glaucoma were randomized to ALT plus topical betaxololor no treatment and were followed up every 3 months. Results showed that treated
patients had half the risk of progression of their nontreated counterparts. Disk hem-orrhage, higher IOP, pseudoexfoliation, worse mean deviation, and older age wereall risk factors for progression. Conclusion Although there are a number of options that have been
American Academy of Ophthalmology Preferred Practice Patterns Commit-tee Glaucoma Panel: Preferred practice patterns. Primary open angle glau-
studied as initial management of IOP in glaucoma and
coma. San Francisco, CA: American Academy of Ophthalmology;
ocular hypertension, medical management still appears
to be the most widely used treatment initially. Within
The Glaucoma Laser Trial Research Group: The Glaucoma Laser Trial (GLT)2. Results of argon laser trabeculoplasty versus topical medications. Oph-
medical management, prostaglandins make the most
sense for initial therapy, although only one of them (la-
The AGIS Investigators: The Advanced Glaucoma Intervention Study (AGIS):
tanoprost) has actually been approved for first line
4. Comparison of treatment outcome within race. Seven year results. Oph-
therapy [10]. Laser trabeculoplasty is still mostly used in
patients for whom medical therapy does not provide ad-
Physicians Desk Reference for Ophthalmic Medicines. Montvale, NJ: MedicalEconomics, Inc.; 2003.
equate IOP lowering, although results from the glau-coma laser trial indicate that initial treatment with laser
Netland PA, Kolker AE: Osmotic drugs. In Glaucoma Medical Therapy: Prin-ciple and Management. Edited by Netland PA, Allen RC. Foundation of the
trabeculoplasty is a reasonable option. If SLT turns out
American Academy of Ophthalmology; 1999:133–147.
to be repeatable, it may quickly surpass standard ALT as
Tsai JC, Forbes M: Medical Management of Glaucoma. Caddo, Oklahoma:
the laser treatment of choice for open angle glaucoma.
Professional Communications Inc.; 2003.
Despite results from the Collaborative Initial Glaucoma
Camras CB, Toris CB, Tamesis RR: Efficacy and adverse effects of medica-
Trial, showing equivalent outcomes in patients treated
tions used in the treatment of glaucoma. Drugs Aging 1999, 15:377–388.
with trabeculectomy initially as an alternative to medical
Eisenberg DL, Toris CB, Camras CB: Bimatoprost and travoprost: a review of
therapy, the complications of surgery and short-term vi-
recent studies of two new glaucoma drugs. Surv Ophthalmol 2002, 47(suppl1):S105–S115.
sual results have prevented trabeculectomy from being
Review article evaluating two studies that compare bimatoprost and travoprost
adopted as an initial treatment for glaucoma in most pa-
with timolol and latanoprost. Each study supports the conclusion that these agentswere more effective than timolol and as effective as latanoprost in terms of their
tients. Whether or not to use antifibrotic therapy at the
Current management of glaucoma Schwartz and Budenz
Susanna R, Giampini J, Borges AS, et al.: A double-masked randomized clini-
Asrani S, Zeimer Wilensky J, Gieser D, et al.: Large diurnal fluctuations in
cal trial comparing latanoprost with unoprostone in patients with open-angle
intraocular pressure are an independent risk factor in patients with glaucoma.
glaucoma or ocular hypertension. Ophthalmology 2001, 108:259–263.
Jampel HD, Bacharach J, Sheu WP, et al.: Latanoprost/Unoprostone Study
Orzalesi N, Rossetti L, Invernizzi T, et al.: Effect of timolol, latanoprost, and
Group. Randomized clinical trial of latanoprost and unoprostone in patients
dorzolamide on circadian IOP in glaucoma or ocular hypertension. Invest
with elevated intraocular pressure. Am J Ophthalmol 2002, 134:863–871.
Ophthalmol Vis Sci 2000, 41:2566–2573.
Randomized clinical trial comparing efficacy of latanoprost versus unoprostone in
Brubaker RF: Delayed functional loss in glaucoma. LII Edward Jackson Me-
lowering IOP. During an 8-week study period, latanoprost once daily lowered IOP
morial Lecture. Am J Ophthalmol 1996, 121:473–483.
more than unoprostone twice daily in patients with elevated IOP.
Leibowitz HM, Krueger DE, Maunder LR, et al.: The Framingham Eye Study
Dubiner H, Cooke D, Dirks M, et al.: Efficacy and safety of bimatoprost in
monograph: An ophthalmological epidemiological survey of cataract, glau-
patients with elevated intraocular pressure: a 30-day comparison with latano-
coma, diabetic retinopathy, macular degeneration, and visual acuity in a gen-
prost. Surv Ophthalmol 2001, 45(suppl 4):S353–S360.
eral population of 2631 adults, 1973–1975. Surv Ophthalmol 1980,24(suppl):335–610.
Gandolfi S, Simmons ST, Sturm R, et al.: Three-month comparison of bima-toprost and latanoprost in patients with glaucoma and ocular hypertension.
Sommer A, Tielsch JM, Katz J, et al.: Relationship between intraocular pres-
sure and primary open angle glaucoma among white and black Americans:The Baltimore Eye Survey. Arch Opthalmol 1991, 109:1090–1095.
Noecker RS, Dirks MS, Choplin NT, et al.: Bimatoprost/Latanoprost Study
Group. A six-month randomized clinical trial comparing the intraocular pres-
Uram M: Ophthalmic laser microendoscope ciliary process ablation in the
sure-lowering efficacy of bimatoprost and latanoprost in patients with ocular
management of neovascular glaucoma. Ophthalmology 1992, 99:1823–
hypertension or glaucoma. Am J Ophthalmol 2003, 135:55–63.
Six-month randomized, multicenter study comparing the IOP-lowering effect of bi-
Bartamian M, Higginbotham EJ: What is on the horizon for cycloablation?
matoprost with latanoprost. The study concluded that bimatoprost was more ef-
Curr Opin Ophthalmol 2001, 12:119–123.
fective than latanoprost in lowering IOP. A greater incidence of conjunctival hyper-emia and eyelash growth were found in the bimatoprost group.
Egbert PR, Fiadoyor S, Budenz DL, et al.: Diode laser transscleral cyclopho-tocoagulation as a primary surgical treatment for primary open-angle glau-
Netland PA, Landry T, Sullivan EK, et al.: Travoprost compared with latano-
coma. Arch Ophthalmol 2001, 119:345–350.
prost and timolol in patients with open-angle glaucoma or ocular hyperten-sion. Am J Ophthalmol 2001, 132:472–484.
Wise JB, Witter SL: Argon laser therapy for open-angle glaucoma. A pilotstudy. Arch Ophthalmol 1979, 97:319–322.
Palmberg PF: Personal communication.
Wise JB: Long-term control of adult open angle glaucoma by argon laser
Noecker RJ, Earl ML, Mundorf T, et al.: Bimatoprost 0.03% versus travoprost
treatment. Ophthalmology 1981, 88:197–202.
0.004% in black Americans with glaucoma or ocular hypertension. Adv Ther
Greenidge KC, Spaeth GL, Fiol-Silva Z: Effect of argon laser trabeculoplasty
on the glaucomatous diurnal curve. Ophthalmology 1983, 90:800–804.
Randomized, multicenter, parallel design trial comparing the IOP-lowering efficacyof bimatoprost versus travoprost in black Americans. Results showed that after 3
Shingleton BJ, Richter CU, Dharma SK, et al.: Long-term efficacy of argon
months, mean IOP reduction from baseline was 8.4 mm Hg in the bimatoprost
laser trabeculoplasty. A 10-year follow-up study. Ophthalmology 1993,
group and 7.9 mm Hg in the travoprost group. This relatively small study—16 pa-
tients were enrolled in the bimatoprost group and 15 in the travoprost group—is a
Rodrigues MM, Spaeth GL, Donohoo P: Electron microscopy of argon laser
precursor to a larger clinical trial.
therapy in phakic open-angle glaucoma. Ophthalmology 1982, 89:198–210.
Parrish RK, Palmberg P, Sheu WP and the XLT Study Group: A comparison
Melamed S, Pei J, Epstein DL: Delayed response to argon laser trabeculo-
of latanoprost, bimatoprost, and travoprost in patients with elevated intraoc-
plasty in monkeys. Morphological and morphometric analysis. Arch Ophthal-
ular pressure: a 12-week, randomized, masked-evaluator multicenter study.
Am J Ophthalmol 2003, 135:688–703.
This well-designed interventional study compared the IOP-lowering effect and
Schwartz AL: Argon laser trabeculoplasty in glaucoma: What’s happening
safety of latanoprost, bimatoprost, and travoprost in patients with open-angle glau-
(survey results of American Glaucoma Society members). J Glaucoma 1993,
coma or ocular hypertension. Results showed comparable efficacy in pressure
lowering among the three agents, with latanoprost having the least adverse ocular
Latina MA, Sibayan SA, Shin DH, et al.: Q-switched 532-nm Nd:YAG laser
trabeculoplasty (selective laser trabeculoplasty): a multicenter, pilot, clinicalstudy. Ophthalmology 1998, 105:2082–2088.
Strahlman E, Tipping R, Vogel R: A double-masked, randomized 1-year studycomparing dorzolamide (Trusopt), timolol, and betaxolol. International Dorzol-
Latina MA, Tumbocon JA: Selective laser trabeculoplasty: a new treatment
amide Study Group. Arch Ophthalmol 1995, 113:1009–1016.
option for open angle glaucoma. Curr Opin Ophthalmol 2002, 13:94–96.
Schuman JS, Horwitz B, Choplin NT, et al.: A 1-year study of brimonidine
Kramer TR, Noecker RJ: Comparison of the morphologic changes after se-
twice daily in glaucoma and ocular hypertension. A controlled, randomized,
lective laser trabeculoplasty and argon laser trabeculoplasty in human eye
multicenter clinical trial. Chronic Brimonidine Study Group. Arch Ophthalmol
bank eyes. Ophthalmology 2001, 108:773–779.
Damji KF, Shah RC, Rock WJ: Selective laser trabeculoplasty v argon laser
LeBlanc RP: Twelve-month results of an ongoing randomized trial comparing
trabeculoplasty: A prospective randomized clinical trial. Br J Ophthalmol
brimonidine tartrate 0.2% and timolol 0.5% given twice daily in patients with
glaucoma or ocular hypertension. Brimonidine Study Group 2. Ophthalmol-
Melamed S, Ben Simon GJ, Levkovitch-Verbin H: Selective laser trabeculo-
plasty as primary treatment for open-angle glaucoma. A prospective, nonran-domized pilot study. Arch Ophthalmol 2003, 121:957–960.
Kass MA, Meltzer DW, Gordon M, et al.: Compliance with topical pilocarpine
This study explored the safety and efficacy of SLT as primary treatment for patients
treatment. Am J Ophthalmol 1986, 101:515–523.
with open-angle glaucoma. Forty-five eyes of 31 patients with open-angle glau-coma or ocular hypertension underwent SLT as primary treatment. Eighty-nine per-
Kass MA, Gordon M, Morley RE Jr, et al.: Compliance with topical timolol
cent had a decrease of 5 mm Hg or more. The study concluded that SLT is a safe
treatment. Am J Ophthalmol 1987, 103:188–193.
and effective treatment for newly diagnosed ocular hypertension and open-angle
Greenberg RN: Overview of patient compliance with medication dosing: a
literature review. Clin Ther 1984, 6:592–599.
http://www.som.tulane.edu/tccep/slt/slt.htm
Fiscella RG, Green A, Patuszynski DH, et al.: Medical therapy cost consider-
Fluorouracil Filtering Surgery Study one-year follow-up: The Fluorouracil Fil-
ations for glaucoma. Am J Ophthalmol 2003, 136:18–25.
tering Study Group. Am J Ophthalmol 1989, 108:625–635.
This study attempted to calculate the daily patient cost of medical glaucomatherapy and review cost trends. Findings were that all generic timolol, Betimol,
Three year follow-up of the Fluorouracil Filtering Surgery Study: The Fluoro-
OptiPranolol, Timoptic, and Timoptic XE ranged from 38 cents to 50 cents per day.
uracil Filtering Study Group. Am J Ophthalmol 1993, 115:82–92.
Cosopt (US$1.05 per day) was less costly than separate bottles of a topical
Chen CW: Enhanced intraocular pressure controlling effectiveness of tra-
-blocker and a topical carbonic anhydrase inhibitor. The prostaglandin analogs
beculectomy by local application of mitomycin-C. Trans Asia-Pacific Acad
ranged from 90 cents per day (Rescula) to $1.25 per day (Xalatan).
Gonzalez: Serafin, RPh, Pharmacy Director, Anne Bates Leach Eye Hospital.
Palmer SS: Mitomycin as adjunct chemotherapy with trabeculectomy. Oph-
Glaucoma
Singh K, Mehta K, Shaikh NM, et al.: Trabeculectomy with intraoperative mi-
Initial Glaucoma Treatment Study: interim quality of life findings after initial
tomycin C versus 5-fluorouracil. Prospective randomized clinical trial. Oph-
medical or surgical treatment of glaucoma. Ophthalmology 2001,
Lachkar Y, Hamard P: Nonpenetrating filtering surgery. Curr Opin Ophthal-
Mermoud A, Salmon JF, Alexander P, et al.: Molteno tube implantation for
neovascular glaucoma. Long-term results and factors influencing the out-
This article provides a thorough review of the various modalities of nonpenetrating
come. Ophthalmology 1993, 100:897–902.
filtering surgery. The article examines techniques, efficacy, and results from clinicaltrials.
Sidoti PA, Dunphy TR, Baerveldt G, et al.: Experience with the Baerveldtglaucoma implant in treating neovascular glaucoma. Ophthalmology 1995,
Carassa RG, Bettin P, Fiori M, Brancato R: Viscocanalostomy versus trabec-
ulectomy in white adults affected by open-angle glaucoma: a 2-year random-ized, controlled trial. Ophthalmology 2003, 110:882–887.
Ceballos EM, Parrish RK 2nd, Schiffman JC: Outcome of Baerveldt glaucoma
Single-masked, prospective, randomized 24 month trial comparing the effective-
drainage implants for the treatment of uveitic glaucoma. Ophthalmology
ness and safety of viscocanalostomy and trabeculectomy in adults with uncon-
trolled open-angle glaucoma. The group randomized to viscocanalostomy
Retrospective, noncomparative case series that looked at 24 eyes of 24 patients
achieved IOP between 6 mm Hg and 21 mm Hg 76% of the time versus 80% of the
who received Baerveldt glaucoma drainage implants for the treatment of uveitic
time for trabeculectomy with no intraoperative antimetabolites. A lower pressure,
glaucoma. Success (IOP 5 to 21 mm Hg) was achieved in 91.7% of the patients at
albeit with a greater complication rate and more labor-intensive postoperative
24 months. The study concluded that these drainage implants provide reasonable
course, was achieved more often with trabeculectomy.
safety and effectiveness for the control of IOP in eyes with uveitis and refractory
Wilson MR, Mendis U, Smith SD, et al.: Ahmed glaucoma valve implant vs
trabeculectomy in the surgical treatment of glaucoma: a randomized clinical
trial. Am J Ophthalmol 2000, 130:267–273.
Chen PP, Yamamoto T, Sawada A, et al.: Use of antifibrosis agents and glau-coma drainage devices in the American and Japanese Glaucoma Societies. J
Janz NK, Wren PA, Lichter PR, et al.: CIGTS Study Group. The Collaborative
SHANNON S. TEMPLET, DIRECTOR This public document was published at a total cost of $.31. Two copies of this public document were published in this 1st printing at a cost of $.62 each. The total cost of all printings of this document including reprints is $.62. This document was published by the Department of State Civil
Federal Bureau of Investigation Color of Law - Civil Application Request for Investigation and Remedies for Violations of Title 42, U.S.C., Section 14141 (Police Misconduct Statute) This application is a formal request for the Department of Justice to seek civil remedies due to policies and practices that foster a pattern of misconduct by employees of the Los Angeles Police Dep
 Glaucoma
Glaucoma