Ordered, immediately called back and the same day delivered the order.Very pleased with the work. Thank you for prompt and accurate work https://africarx.co.za/buy-cialis-south-africa.html great prices, delivered on the day of the order. Pleasant managers consult by phone.
Doi:10.1016/s0003-9993(02)04906-7
Intrathecal Baclofen in Subjects With Spastic Hemiplegia: Assessment of the Antispastic Effect During Gait Olivier Re´my-Ne´ris, MD, PhD, Vincent Tiffreau, MD, Ste´phane Bouilland, MD, Bernard Bussel, MD
ABSTRACT. Re´my-Ne´ris O, Tiffreau V, Bouilland S,
2003 by the American Congress of Rehabilitation Medi-
Bussel B. Intrathecal baclofen in subjects with spastic
cine and the American Academy of Physical Medicine and
hemiplegia: assessment of the antispastic effect during gait.
Arch Phys Med Rehabil 2003;84:643-50. Objective: To determine whether leg muscle stiffness is PENN AND KROIN1 FIRST SHOWED that long-term ad-
measurably reduced after intrathecal baclofen (ITB) in subjects
ministration of intrathecal baclofen (ITB) with implantable
pumps reduces spasticity in nonambulatory subjects with spinal
Design: Nonrandomized trial.
cord injury (SCI). Since then, numerous studies have assessed
Setting: Inpatient multidisciplinary rehabilitation unit in
the functional benefit of ITB in spastic subjects with SCI2 and
with cerebral palsy3 (CP) and in spastic adults with brain
Participants: Seven consecutive subjects with spastic hemi-
injury.4,5 Meythaler et al6 recently showed that continuous
plegia having Ashworth Scale scores for their quadriceps and
delivery of ITB decreases spastic hypertonia due to stroke. ITB
can provide some functional improvements to nonambulatory
Intervention: Subjects were given ITB by lumbar puncture
subjects whose spasticity is of cerebral origin,7 but most of the
improvements do not influence gait,8 although the walking
Main Outcome Measures: Triceps and quadriceps Ash-
capacity of some subjects improved. This inconsistent im-
worth scores, gait analysis at preferred and maximal speed
provement can be attributed to orthopedic conditions, loss of
measured by a motion analysis system with 2 forceplates, and
voluntary motor control, decreased muscle stiffness if the sub-
electromyographic recording of leg muscles before and 4 hours
jects used hypertonia to stay upright,9 or persistent muscle
after ITB. The slopes of the moment-angle curves were mea-
sured on the hemiplegic side at the onset of ankle and knee
The muscle hypertonia of subjects with central nervous
flexion to assess muscle stiffness during walking. Pre- andpost-ITB spatiotemporal, kinetic, and kinematic data were
system lesions may have several explanations. Muscle contrac-
compared by using a nonparametric test (Wilcoxon signed-rank
tures and altered muscle mechanical properties contribute to
muscle hypertonia in subjects with spasticity.10,11 Spasticity,
Results: Ashworth scores of the quadriceps and triceps of all
defined as a velocity-dependent increase in the tonic stretch
subjects decreased significantly after ITB. Maximal walking
reflex,12 is often associated with dystonia, rigidity, spasms, and
speed increased significantly, with a significant increase in
myoclonus6,13 in subjects with acquired brain lesions. All these
stride length, but the preferred walking speed was unchanged.
neural mechanisms can contribute to muscle hypertonia. But
Minimal knee extension and maximal ankle flexion were the
they have very different effects in static and dynamic condi-
only kinematic data significantly different (increased) after
tions, and there seems to be little correlation between patho-
ITB. The slope of the ankle moment-angle curve decreased
logic responsiveness to muscle stretch measured at rest and
significantly after ITB at preferred gait speed; it also decreased
motor impairment assessed under natural conditions during
at maximal gait speed in all but 1 subject. Of the 4 available
motion.14-16 Thus, a clinically identified reduced spasticity at
moment-angle curves, 3 showed decreased knee extensor mus-
rest after ITB does not automatically result in improved func-
cle stiffness. The duration of the bursts of spastic muscles
tional skills, and any such improvement cannot be easily cor-
related with reduced muscle stiffness. Quantitative studies on
Conclusion: Acute ITB improved walking and reduced
the neural components of spastic hypertonia in humans usually
muscle stiffness at both the ankles and knees on the spastic
use electromyographic recordings and measurements of the
hemiplegic side of our subjects. Electromyographic findings
amplitude of reflex responses. Electromyographic recording of
suggest that some of the post-ITB reduction in muscle stiffness
the spontaneous activity of muscles during gait cannot be the
might be attributed to decreased spasticity.
only means of assessing the neural components of a disorder
Key Words: Baclofen; Gait; Hemiplegia; Muscle spasticity;
because electromyographic activity reflects normal voluntary
muscle discharge and hyperactive reflex responses, both ofwhich contribute to the muscle resistance.17,18 The resistancedue to muscle stretch and muscle contraction during gait can beevaluated from joint moments that result from the interplay ofagonist and antagonist forces.19 The coupling of kinematics,
From Groupe Hopale, Motion Analysis Laboratory, and Department of Physical
kinetics, and electromyography thus seems to be the best way
Medicine, Berck sur Mer (Re´my-Ne´ris Tiffreau, Bouilland), and Assistance Publique
to assess the contribution of the neural component of muscle
Hopitaux de Paris, Department of Physical Medicine, Hoˆpital Raymond Poincare,
hypertonia during gait in subjects with spastic CP.17,18
ITB produces a significant decrease in spastic hypertonia at
No commercial party having a direct financial interest in the results of the research
supporting this article has or will confer a benefit upon the author(s) or upon any
rest in subjects with acquired cerebral lesions.6,13,20 The present
organization with which the author(s) is/are associated.
study was therefore undertaken to determine whether acute ITB
Reprint requests to Olivier Re´my-Ne´ris, MD, Centre Calve, Groupe Hopale, 72
injections improved the gait of subjects with spastic hemiplegia
Esplanade Parmentier, 62600 Berck sur mer, France, e-mail: Oremyneris@hopale.com.
and reduced the muscle stiffness measured during gait from
0003-9993/03/8405-7488$30.00/0doi:10.1016/S0003-9993(03)04906-7
Arch Phys Med Rehabil Vol 84, May 2003 INTRATHECAL BACLOFEN AND HEMIPLEGIA, Re´my-Ne´ris Table 1: Subjects’ Characteristics
NOTE. Significance was evaluated with a Wilcoxon signed-rank test. Abbreviation: SD, standard deviation.
The kinematic variables for hip, knee, ankle, and spatiotem-
poral measure (walking speed, length of the stride, single and
Participants
double support stance times) were calculated for the pretreat-
This investigation was performed on 7 subjects with hemi-
ment and posttreatment sessions. Vertical forces (Fz) were
plegia (6 men, 1 woman; mean age, 40y; range, 20 – 64y). It
used to determine the onset and end of the support phase.
was approved by the medical ethics committee of Ambroise
Because 2 parallel, large (length, 1200mm) forceplates were
Pare´ Hospital, and informed consent was obtained from each
used, 2 or more heel strikes on a forceplate were obtained for
subject before he/she entered the trial. Data on the subjects, the
each limb to determine a complete gait cycle.
cause of their disability, time after illness, and initial Ashworth
One purpose of the present study was to determine whether
Scale scores for the triceps and quadriceps are summarized in
acute ITB injections reduced the muscle stiffness exhibited
table 1. The tibialis anterior and hamstring tone were free of
during gait, as measured by biomechanical parameters. Frigo et
spasticity. The mean time after illness was 5.2 years (range,
al19 studied the reproducibility of the coupling of joint angles
1–14y). The hemiplegia was caused by stroke in 4 subjects,
and ankle and knee moments in unimpaired subjects. The
traumatic brain injury (TBI) in 2, and CP in the last subject. All
slopes of the resulting moment-angle curve, which can be
subjects had hyperactive ankle and knee-jerk reflexes and a
related to the force-length relationship that describes the stiff-
minimum Ashworth score of 2 of 5 for the quadriceps.
ness of muscles, can be used to infer the resistance offered by
All participants were able to walk without hand support for
the joint during rotation. We used the same method and cal-
a minimum distance of 10m. They were all on oral antispastic
culated internal joint moments by using the inverse dynamics
drugs that were not sufficient to reduce leg muscle tone. Their
technique. Analysis of the joint moment-angle curve and of the
current antispastic treatment was not changed during the study.
electromyographic activity gives a quantitative indication ofspasticity during gait.17,18 Because joint moments assess the
General Experimental Procedure
resultant force applied to the joints center of rotation, this
All subjects were given a test bolus of 50g baclofen by
method cannot distinguish the action of 1 muscle from that of
lumbar puncture. Ashworth scores for the quadriceps and tri-
the others, but measures their combined, overall action. Surface
ceps were measured, and a free 10-m walk was performed
electromyography registers the muscle activity of superficial
before and 4 hours after injection. The dose of baclofen was
muscles. The electromyographic activity of some muscles that
increased by 50g if the mean Ashworth scores for the quad-
might be spastic and contribute to the joint moment might not
riceps and triceps decreased by less than 1 point after this first
be considered. Despite these limitations and because the stron-
dose. Three of 7 subjects needed a 100-g dose, but none
ger muscles that contribute most to joint moments are super-
ficial (triceps, tibialis anterior, quadriceps, hamstrings), joint
The subjects were tested again after a 48-hour washout
moments and electromyographic activity recordings are in-
period using the appropriate dose of baclofen, injected intra-
creasingly being used to assess spasticity.21-23 This approach
thecally. Ashworth scores for both the quadriceps and triceps
seems a reasonable way to assess changes in spasticity after
were measured just before and 4 hours after the intrathecal
ITB during gait. The markers and electrodes were not removed
injection of baclofen; gait was also assessed by using the Vicon
between the pre- and post-ITB gait measurements so that we
motion analysis system,a 2 forceplates, and electromyography.
could assess the reliability of joint moments and electromyo-
Each subject underwent 2 sessions of 10 trials walking at their
graphic recordings. The slopes of the moment-angle curves,
own pace at preferred and maximal speeds over 10m. Data
which are features of the changes in muscle tone during muscle
were recorded with a 60-Hz sampling rate. Markers were
stretch before and after ITB, were compared for each subject.
placed over the anterior superior iliac spine, trochanter, lateral
The present study focused on spasticity of the flexor and
knee condyle, mid lateral thigh, lateral malleolus, mid lateral
extensor muscles of the ankle and knee. Therefore, only the
shank, heel, and second metatarsal to define the segments of the
kinematic and kinetic data for the ankle, knee, and hip flexion
thigh, shank, and foot. The markers enabled 3-dimensional
are reported. Muscles are phasically activated and passively
motion analysis of the legs. Electromyographic recordings,
stretched by joint motion during walking. The period of the gait
with surface electrodes, were made of the vastus lateralis,
cycle during which the triceps is stretched is illustrated in
biceps femoris, tibialis anterior, and soleus.
figure 1. Because all subjects showed a toe-heel or a flat-foot
Arch Phys Med Rehabil Vol 84, May 2003 INTRATHECAL BACLOFEN AND HEMIPLEGIA, Re´my-Ne´ris
cannot be proved, pre- and post-ITB data were compared bymeans of a nonparametric test (Wilcoxon signed-rank test). Post-ITB data were considered significantly different frompre-ITB data for P less than .05.
Table 1 shows the quadriceps and triceps Ashworth scores.
The spasticity at rest, as indicated by the triceps and quadricepsdata for the hemiplegic side, was significantly reduced in allsubjects after the appropriate dose of baclofen (mean quadri-ceps, 3.3 vs 1.3; mean triceps, 3.4 vs 2.1; see table 1). Thedecrease in spasticity was greater for the quadriceps than forthe triceps.
The preferred gait velocity increased significantly after ITB
(pre-ITB, .53Ϯ.29m/s; post-ITB, .60Ϯ.34). The maximum gaitspeed increased (pre-ITB, .82Ϯ0.4m/s; post-ITB, .93Ϯ.45m/s)but was not statistically significant. The mean increase inmaximum gait speed Ϯ standard deviation (SD) was.15Ϯ.08m/s in the 6 of 7 subjects whose gait velocity increased
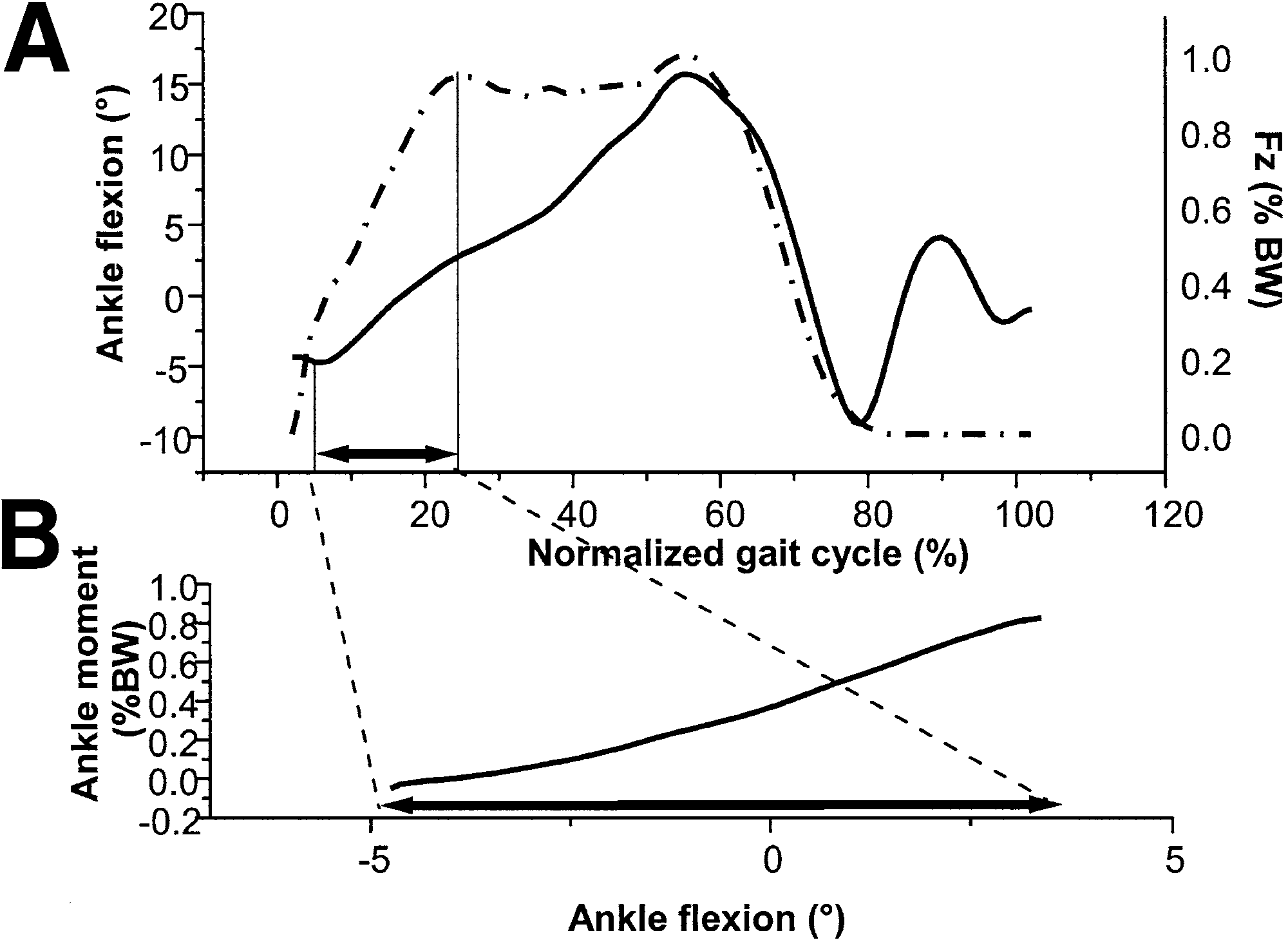
Fig 1. Gait characteristics of S3 before baclofen. (A) Changes in the
(table 2). Subject S5 was the only patient whose maximal gait
ankle joint angle (solid line) and Fz (dotted line) during walking. The time period (arrow in both graphs) is the beginning of the gait cycle
speed decreased greatly (pre-ITB, 1.04m/s; post-ITB, 0.9m/s). just after the heel strike that corresponds to stretching of the
This subject’s preferred gait speed increased slightly after ITB
triceps. (B) The ankle moment increased regularly. Fz and the ankle
(from .65m/s to .68m/s). He said he felt tired at the time of
moment are expressed as a percentage of the body weight (% BW).
evaluation, although most subjects felt they walked more easily
The gait cycle is normalized (100%).
after ITB. The increase in walking speed correlated with asignificant increase in stride length at both preferred (mean
strike, ankle dorsiflexion (the stretching phase of the triceps)
increase Ϯ SD, .05Ϯ.03m) and maximal walking speeds (mean
started at the onset of the gait cycle. Because the single support
increase, .11Ϯ.09m). The stride frequency did not change
phase varied from subject to subject, depending on knee un-
steadiness, ankle clonus, or knee hyperextension, we consid-
Kinetic and kinematic data (maximum, minimum, ampli-
ered only the loading phase (first double support phase) in this
tudes) for the hip, knee, and ankle of the affected and unaf-
study of the ankle moment-angle curve. Knee flexion (quadri-
fected sides were compared before and after baclofen. There
ceps stretching phase) started during the double support phase
was great subject-to-subject variability. The data did not
that preceded swing. Because some subjects showed 20° of
change significantly after ITB at the preferred walking speed.
minimal knee flexion, we compared the knee moment-angle
The minimal knee flexion at maximal walking speed Ϯ SD
curves during stretching of the quadriceps in all subjects from
increased significantly after ITB (pre-ITB, Ϫ1.1°Ϯ5.9°; post-
20° to the end of the knee flexion (fig 2).
ITB, 3.1°Ϯ7.7°), as did maximal ankle dorsiflexion (table 3). Statistical Analysis Ankle Moment
Data from the experiments are presented as means of the 10
Figure 3 shows the ankle flexion during the gait cycle and
consecutive trials. Because the normal distribution of the data
the ankle angle-moment correlation during the initial phase of
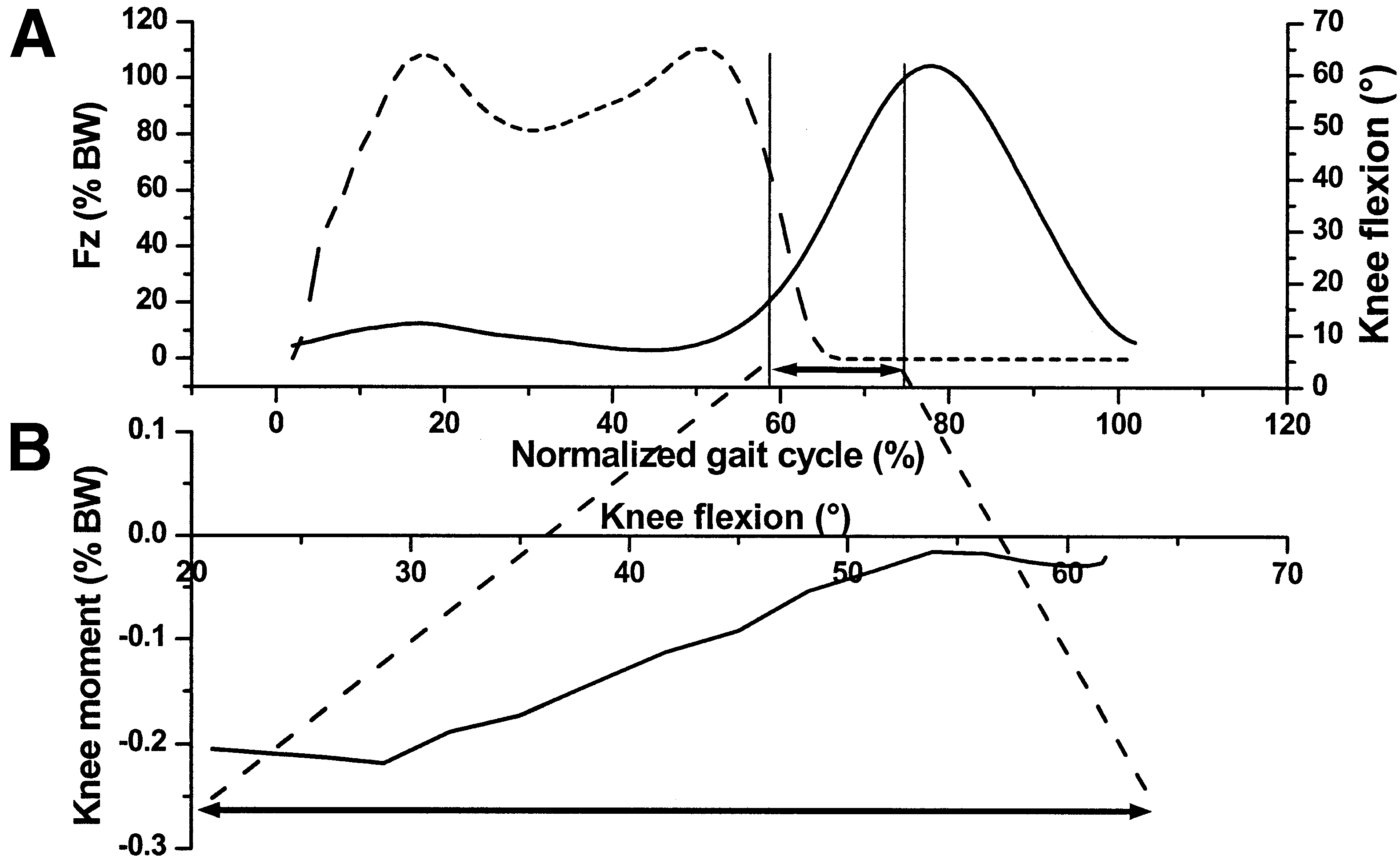
Fig 2. Gait characteristics of S1 before baclofen. (A) Changes in the knee joint angle (solid line) and Fz (dotted line) dur- ing a gait cycle. The period (ar- row in both graphs) is the end of the loading time of the gait cycle just before toe off. (B) The knee moment decreased dur- ing knee flexion in this sub- ject. Fz and the knee moment are expressed as a percentage of the body weight (% BW). The gait cycle is normalized (100%). Arch Phys Med Rehabil Vol 84, May 2003 INTRATHECAL BACLOFEN AND HEMIPLEGIA, Re´my-Ne´ris Table 2: Spatiotemporal Data at Preferred and Maximum Walking Speeds Before and After ITB
Abbreviation: NS, not significant. * Significance was evaluated with a Wilcoxon signed-rank test.
the stance phase corresponding to the stretch of the triceps
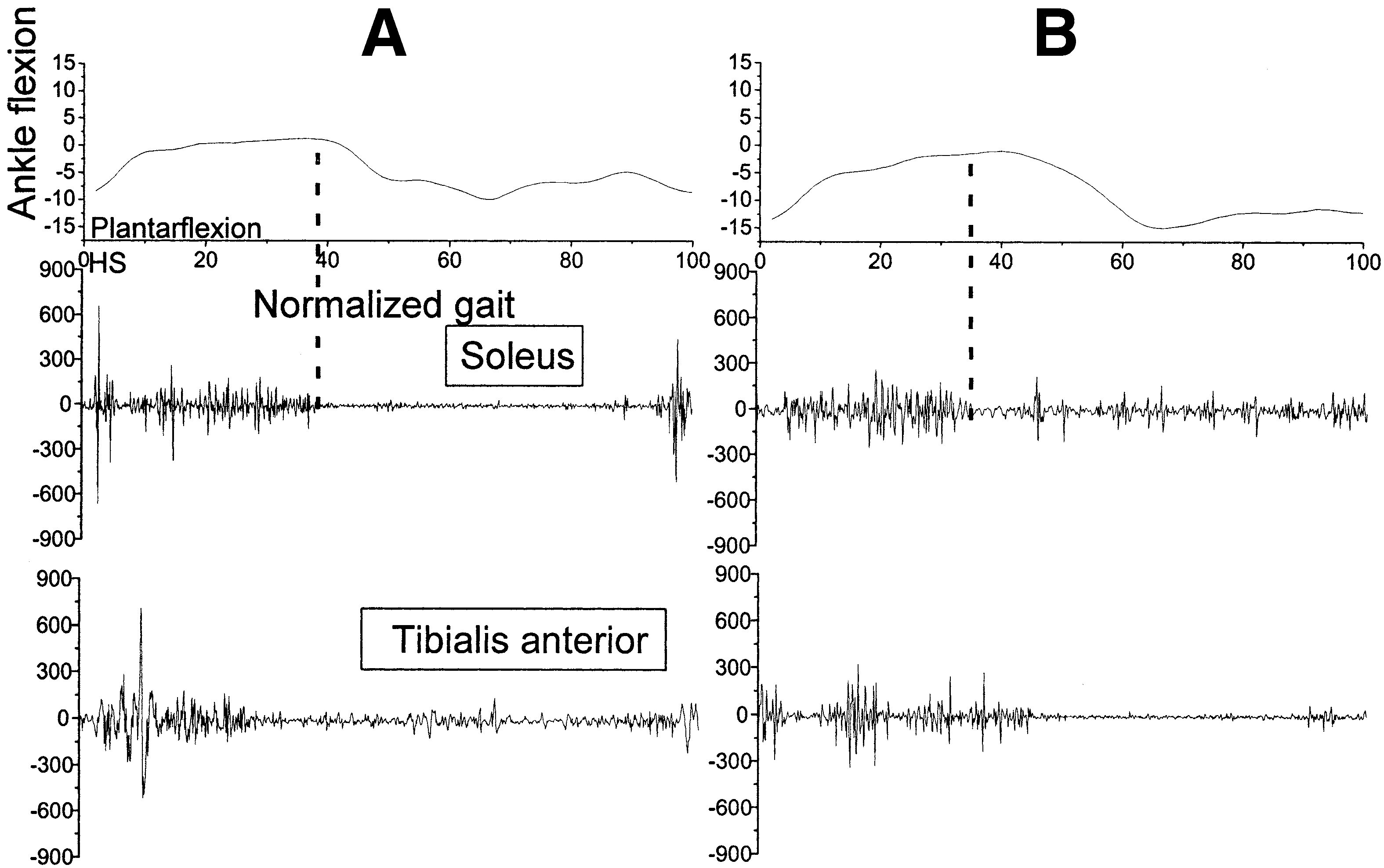
was sustained throughout ankle dorsiflexion. It decreased only
surae at the preferred walking speed in S3. A small plantar-
when the plantarflexion began. ITB produced a decrease in the
flexion appeared at the onset of the gait cycle after ITB. This
electromyographic activity of the soleus at the onset of the gait
corresponds to a retrieval of the heel-toe gait pattern by S3,
cycle. The duration of the burst was shortened until the middle
whose pre-ITB walking pattern was toe-heel.
Data for all subjects are shown in table 3. Maximal dorsi-
All but 1 subject (S5) showed a decrease in the slope of the
flexion of the ankle on the hemiplegic side did not change after
ankle moment-angle curve during ankle dorsiflexion (Pϭ.08)
ITB at preferred walking speed, and it increased slightly at
maximal walking speed Ϯ SD (10.3°Ϯ11.4° vs 13.0°Ϯ11.1°;see table 3). The slope of the moment-angle curve during
Knee Moment
triceps stretching (see Methods) was significantly reduced. The
Subjects S2 and S4, for whom kinetic data were available,
maximal flexion velocity did not change significantly at either
had a stiff leg with a knee flexion that was too small to describe
walking speed. The slope of the ankle-moment curves of the 6
a knee angle-moment curve. Conventionally, knee moments
subjects with spasticity for whom kinetic data were available at
are negative when the resulting force causes knee extension
preferred walking speed decreased significantly after ITB (see
(opening of the popliteal angle) and positive when it causes
table 3). The decrease in the ankle moment-angle curve during
triceps stretching did not correlated significantly with the in-
The slopes of the knee moment-angle curves increased after
crease in walking speed (Spearman test). Figure 4 shows the
ITB in all subjects for whom knee moments could be calculated
ankle motion and electromyographic activity of the ankle flexor
at preferred and maximal gait speeds (S1, S3, S5, S7; fig 5),
and extensor before and after ITB for S1. The soleus electro-
except for S3 at maximal gait speed (see table 3). This pattern
myographic activity before ITB was maximal at heel strike and
indicated a decrease in knee extensor tension or an increase in
Table 3: Ankle and Knee Kinematics and Slope of the Moment-Angle Curve Before (Pre) and After (Post) ITB
NOTE. Significance tested with a Wilcoxon signed-rank test. Abbreviations: AU, arbitrary units; MAD, maximal ankle dorsiflexion; MFV, maximal ankle flexion velocity; MKF, minimal knee flexion duringsupport phase; NA, not available; Slope AMC, slope of the ankle angle-moment curve during the initial phase of dorsiflexion (during stretchingof the soleus, see Methods); Slope KMC, slope of the knee moment-angle curve after 20° of knee flexion in 7 subjects with spastic hemiplegiabefore and after ITB at preferred and maximal walking speed. Arch Phys Med Rehabil Vol 84, May 2003 INTRATHECAL BACLOFEN AND HEMIPLEGIA, Re´my-Ne´ris Fig 3. Ankle dorsiflexion (A) before (dotted line) and after (solid line) ITB at preferred walking speed in S3. The ini- tial plantarflexion is restored. The maximal dorsiflexion is unchanged after ITB. (B) The slope of the moment-angle correlation is reduced.
knee flexor tension during the same period (pre- and post-ITB)
at preferred gait speed, with a 19-fold increase. It also in-
of the knee flexion. Subject S3 showed small changes at both
creased slightly at maximal gait speed.
gait speeds (see table 3, fig 5). The knee moment-angle curves
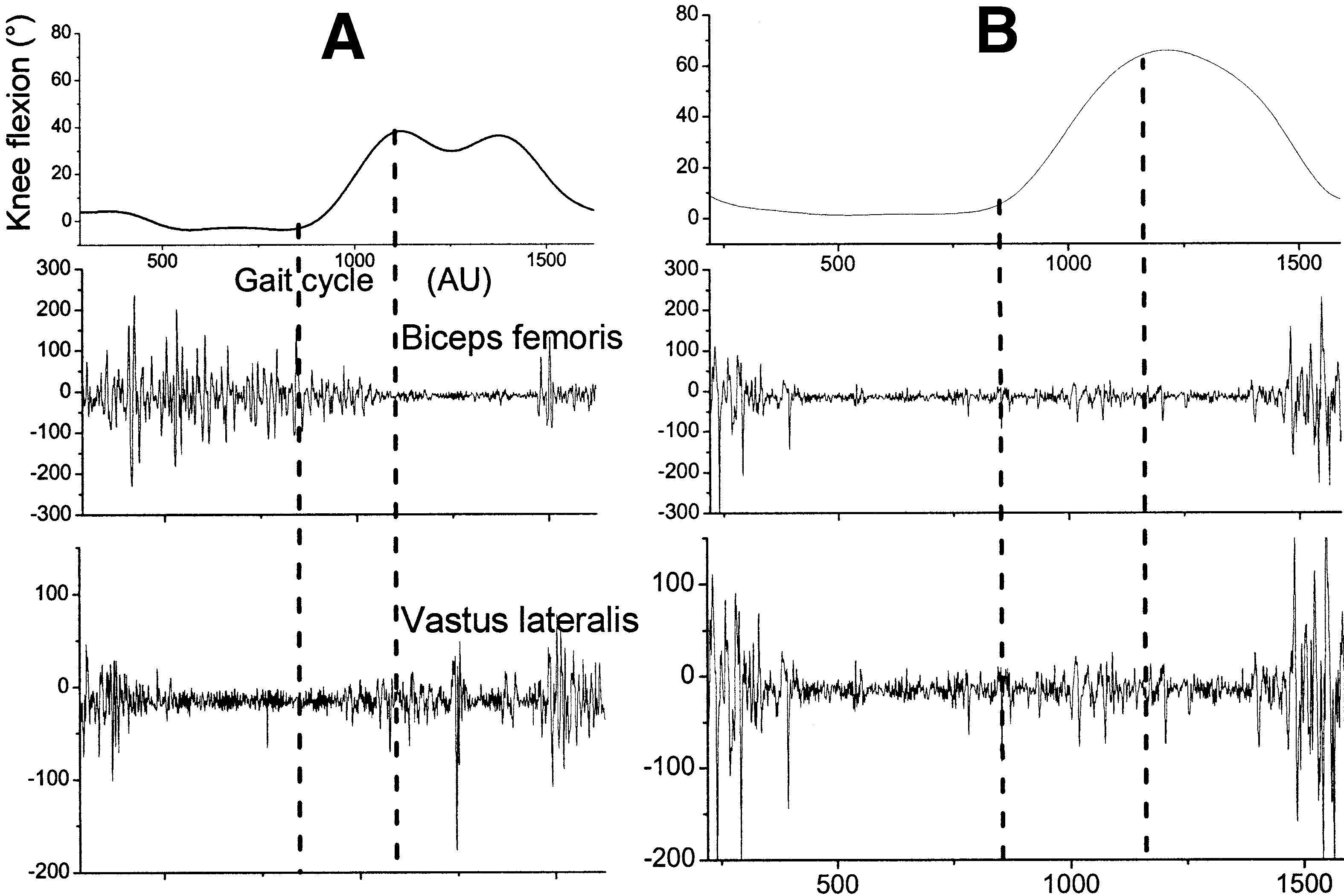
The electromyographic activity of the flexor and extensor
of S1 and S7 (see fig 5) changed markedly after ITB at both
muscles correlated with the calculated joint moment. The elec-
gait speeds: the slope increased 3.7-fold in S1 and was reversed
tromyographic burst seen in the biceps femoris in S1 and S7
in S7. Before ITB, the knee moment increased throughout knee
(fig 6A) before ITB continued until the end of the stance phase.
flexion in S7. After ITB, it decreased as in other subjects. The
This type of increased flexor muscle activity can offset the knee
slope of the knee moment-angle curve for S5 changed greatly
extension moment caused by knee flexion and explain the
Fig 4. Ankle flexion and elec- tromyographic activity of the soleus and tibialis anterior (A) before ITB and (B) after ITB in S1 during a gait cycle. Abbre- viation: HS, heel strike. Arch Phys Med Rehabil Vol 84, May 2003 INTRATHECAL BACLOFEN AND HEMIPLEGIA, Re´my-Ne´ris Fig 5. Mean moment-angle curves of the knee during knee flexion (see fig 2) in 4 hemiple- gic subjects with a knee flexion more than 20° during the swing phase before ITB (dashed lines) and after ITB (solid lines). Joint moments are expressed as a percentage of the body weight (% BW).
almost zero knee moment in these subjects before ITB. The
spasticity is of cerebral origin.5,6,8,13,20,24-27 Subjects with spas-
vastus lateralis of the same subjects showed a burst of electro-
tic hemiplegia after TBI8,13,20 and stroke20,27 all showed im-
myographic activity at the beginning of knee flexion, and it
proved function. But some controversy exists about the im-
increased during knee flexion when the electromyographic
provement in ambulant subjects. Some have shown an
burst in the biceps decreased (see fig 6A). This increased
improvement in gait pattern,8,24 while others suggested that
electromyographic activity of knee extensors might explain the
intrathecal antispastic therapy is contraindicated in some sub-
increased knee-extension moment during knee flexion. The
jects who use muscle stiffness to stay upright.9 Our subjects
burst of electromyographic activity in the biceps femoris was
with hemiplegia walked significantly faster only at maximal
dramatically shorter after ITB, and there was no activity during
walking speed, because their strides were longer. The kine-
knee flexion (fig 6B). There was some electromyographic ac-
matic and kinetic data for our subjects with spasticity varied
tivity in the vastus lateralis during knee flexion, but the elec-
greatly. Administration of ITB resulted in an increased maxi-
mal ankle flexion and a significantly decreased knee hyperex-tension at maximal gait speed. DISCUSSION
One of the most characteristic features of spastic gait is how
it varies for a given subject and between subjects.28 De Quer-
Gait Improvement
vain et al29 showed that subjects with hemiplegia could have
ITB is considered an effective way to reduce spastic hyper-
several types of gait patterns, and we did not choose 1 specific
tonia that is resistant to oral medication in subjects whose
gait pattern in our study. The great variability also noticed by
Fig 6. The patterns of vastus lateralis and biceps femoris ac- tivation (A) before ITB and (B) after ITB in S1. The biceps fem- oris was activated throughout the stance phase until the initial flexion of the knee before ITB and not after ITB. The vastus lateralis activation during knee flexion decreased after ITB. The gait cycle is expressed in arbi- trary units (AU). Arch Phys Med Rehabil Vol 84, May 2003 INTRATHECAL BACLOFEN AND HEMIPLEGIA, Re´my-Ne´ris
previous researchers30-32 looking for improved objective gait
increased walking speed with decreased muscle stiffness, they
parameters after antispastic treatment might partly explain the
clearly suggest that a marked reduction in muscle stiffness
lack of change shown by any subject at preferred walking
might help to improve walking, as was found for spastic
speed after ITB. Gait in subjects with spasticity has usually
subjects with continuous ITB infusion.8,24 But such an infusion
been assessed at preferred walking speed.8,32-34 We showed a
might also be pernicious in subjects who use their stiffness to
significant velocity increase and significant kinematic changes
only at maximal walking speed. Thus, it might be more suitable
Spasticity is a velocity-dependent increase in the stretch
to assess any therapeutic intervention for this population at this
reflex.12 Because gait velocity slightly increased and the peak
walking speed. This needs further investigation.
ankle and knee flexion velocities did not decrease after ITB, we
The increased walking speed was due to a significant in-
can assume that the decrease in muscle stiffness after ITB was
crease in stride length and no change of cadence. Although we
not due to a change in muscle stretch velocity. Nor were small
saw no significant increase in hip flexion amplitude, the in-
changes in ankle flexion velocity and the decreased slopes of
creased stride length might indicate easier muscle stretch, be-
the ankle moment-angle curves correlated. The decreased elec-
cause of decreased spasticity. Gerszten et al8 reported an im-
tromyographic activity in the ankle and knee extensors at the
provement in the gait of some subjects with spasticity after
onset of muscle stretch (ie, the onset of ankle dorsiflexion for
continuous ITB. This increased gait capacity might be due to
the triceps and knee flexion for the quadriceps) might be
increased walking speed or to lower energy consumption re-
attributed to the decreased voluntary muscle contraction or to
sulting from better walking mechanical conditions and reduced
ITB-induced changes in reflex electromyographic amplitude.
energy cost to stretch muscles that would have been weakened
Our experimental design cannot dissociate these 2 mecha-
by ITB. Subjects with spasticity have a high oxygen uptake
nisms. Nevertheless, the post-ITB loss of the electromyo-
relative to the work performed.35-38 Our subject S5, the only
graphic burst of the soleus throughout ankle flexion strongly
subject with impaired walking speed, reported feeling fatigued,
suggests that ITB released inappropriate muscle stretch reflexes
while all other subjects found walking easier. However, this
in these subjects. The simultaneous decrease in muscle stiff-
study focused on a biomechanical assessment after ITB, so we
ness indicated by the angle-moment curves could be due to
cannot comment on subjective improvement in walking after
decreased spasticity. The reduced electromyographic activity
of the vastus lateralis during knee flexion after ITB seems toresult from the same mechanisms. Muscle Stiffness
In unimpaired persons muscle stiffness during motion results
CONCLUSION
from the passive viscoelastic properties of muscle and concen-tric or excentric muscle contractions. Two mechanisms may
Acute ITB improved the walking of adults with hemiplegia
disrupt normal muscle contraction in subjects with spasticity:
whose leg spasticity did not respond to oral antispastic medi-
one is histologic transformations that alter the viscoelastic
cation. The decrease in muscle stiffness and the loss of some
properties,10,11,39 and the other is released segmental spinal
characteristic spastic electromyographic features after ITB sug-
pathways (for a review, see Pierrot-Deseilligny40). Subjects
gest that the improved walking after ITB can be attributed to
with supraspinal lesions of various origins that affect the legs39
reduced stretch reflexes. Further investigation is now needed to
and arms41 show altered muscle viscoelastic properties. The
determine whether these changes produced by acute ITB also
Ashworth Scale42 clinically assesses resistance to passive
occur after continuous ITB infusion.
stretch41 but cannot discriminate between muscle changes andthe release of segmental spinal pathways. Our subjects had no
References
contractures before ITB, but their absence does not exclude
1. Penn RD, Kroin JS. Continuous intrathecal baclofen for severe
histologic changes, as evidenced by Dietz et al,11 who evalu-
ated the influence of such mechanisms in subjects without
2. Azouvi P, Roby-Brami A, Biraben A, Thiebaut JB, Thurel C,
Bussel B. Effect of intrathecal baclofen on the monosynaptic
contractures. These perturbed mechanical properties of mus-
reflex in humans: evidence for a postsynaptic action. J Neurol
cles are not sensitive to antispastic drugs, and any increased
muscle stiffness due to these mechanisms will remain, what-
3. Albright AL, Cervi A, Singletary J. Intrathecal baclofen for spas-
ticity in cerebral palsy. JAMA 1991;265:1418-22.
After ITB, our spastic subjects had a significant decrease in
4. Becker R, Alberti O, Bauer BL. Continuous intrathecal baclofen
the slope of muscle length-tension relationship at the ankle, the
infusion in severe spasticity after traumatic or hypoxic brain
angle-moment curve. This curve indicates that ITB decreased
muscle stiffness in the triceps surae (see Methods). There was
5. Meythaler JM, McCary A, Hadley MN. Prospective assessment of
a marked increase in the slope of the knee angle-moment curve
continuous intrathecal infusion of baclofen for spasticity causedby acquired brain injury: a preliminary report. J Neurosurg 1997;
in some of our subjects at their preferred and maximal walking
speeds. This change suggests that ITB decreased quadriceps
6. Meythaler JM, Guin-Renfroe S, Brunner RC, Hadley MN. Intra-
stiffness, because the decrease in the knee extension moment
thecal baclofen for spastic hypertonia from stroke. Stroke 2001;
was not combined with increased flexor muscle activation.
Subjects who showed the greatest changes in their muscle
7. Van Schaeybroeck P, Nuttin B, Lagae L, Schrijvers E, Borghgraef
stiffness (S1, S5, S7) also showed the greatest changes in their
C, Feys P. Intrathecal baclofen for intractable cerebral spasticity:
maximal walking speed (24% and 27% increase for S1 and S7;
a prospective placebo-controlled, double-blind study. Neurosur-
30% decrease for S5). In S3, the earlier decrease in knee
gery 2000;46:603-9; discussion 9-12.
moment after ITB for knee flexion indicates a slight decrease in
8. Gerszten PC, Albright AL, Barry MJ. Effect on ambulation of
continuous intrathecal baclofen infusion. Pediatr Neurosurg 1997;
quadriceps muscle stiffness: we saw no activity of knee flexors
at this period of the gait cycle like that seen in S1 and S7 after
9. Bodensteiner J. The management of cerebral palsy: subjectivity
ITB. The only subject whose walking capacity greatly deteri-
and a conundrum. J Child Neurol 1996;11:75-6.
orated after ITB was S5. He also showed one of the largest
10. Tabary JC, Tabary C, Tardieu C, Tardieu G, Goldspink G. Phys-
changes in muscle stiffness. While our results cannot correlate
iological and structural changes in the cat’s soleus muscle due to
Arch Phys Med Rehabil Vol 84, May 2003 INTRATHECAL BACLOFEN AND HEMIPLEGIA, Re´my-Ne´ris
immobilization at different lengths by plaster casts. J Physiol
spastic hypertonia in adolescents and adults with cerebral palsy.
Arch Phys Med Rehabil 2001;82:155-61.
11. Dietz V, Quintern J, Berger W. Electrophysiological studies of
27. Penn RD, Gianino JM, York MM. Intrathecal baclofen for motor
gait in spasticity and rigidity. Evidence that altered mechanical
disorders. Mov Disord 1995;10:675-7.
properties of muscle contribute to hypertonia. Brain 1981;104:
28. Steinwender G, Saraph V, Scheiber S, Zwick EB, Uitz C, Hackl
K. Intrasubject repeatability of gait analysis data in normal and
12. Lance JW. Symposium synopsis. In: Koella W, editor. Spasticity:
spastic children. Clin Biomech (Bristol, Avon) 2000;15:134-9.
disordered motor control. Chicago: Year Book Medical; 1980; p
29. De Quervain IA, Simon SR, Leurgans S, Pease WS, McAllister D.
Gait pattern in the early recovery period after stroke. J Bone Joint
13. Meythaler JM, Guin-Renfroe S, Grabb P, Hadley MN. Long-term
continuously infused intrathecal baclofen for spastic-dystonic hy-
30. Kerrigan D, Roth R, Riley P. The modelling of spastic paretic
pertonia in traumatic brain injury: 1-year experience. Arch PhysMed Rehabil 1999;80:13-9.
stiff-legged gait based on actual kinematic data. Gait Posture
14. Sahrmann SA, Norton BJ. The relationship of voluntary move-
ment to spasticity in the upper motor neuron syndrome. Ann
31. Corston RN, Johnson F, Godwin-Austen RB. The assessment of
drug treatment of spastic gait. J Neurol Neurosurg Psychiatry
15. Knutsson E, Martensson A. Dynamic motor capacity in spastic
paresis and its relation to prime mover dysfunction, spastic re-
32. Orsnes GB, Sorensen PS, Larsen TK, Ravnborg M. Effect of
flexes and antagonist co-activation. Scand J Rehabil Med 1980;
baclofen on gait in spastic MS patients. Acta Neurol Scand 2000;
16. Crenna P, Frigo C. Monitoring gait with a vector diagram tech-
33. Hesse S, Jahnke M, Schreider C, Mauritz K. Gait symmetry and
nique in spastic patients. In: Delwaide PJ, Young RR, editors.
functional walking performance in hemiparetic patients prior to
Clinical neurophysiology of spasticity. Amsterdam: Elsevier;
and after a 4-week rehabilitation programme. Gait Posture 1993;
17. Crenna P, Inverno M. Objective detection of pathophysiological
34. Kerrigan DC, Frates EP, Rogan S, Riley PO. Spastic paretic
factors contributing to gait disturbance in supraspinal lesions. In:
stiff-legged gait: biomechanics of the unaffected limb. Am J Phys
Fedrizzi E, Avanzini G, Crenna P, editors. Motor development in
children. London: John Libbey; 1994. p 103-18.
35. Lundberg A. Maximal aerobic capacity of young people with
18. Crenna P. Spasticity and ‘spastic’ gait in children with cerebral
spastic cerebral palsy. Dev Med Child Neurol 1978;20:205-10.
palsy. Neurosci Behav Rev 1998;22:571-8.
36. Mattsson E, Andersson C. Oxygen cost, walking speed, and per-
19. Frigo C, Crenna P, Jensen LM. Moment-angle relationship at
ceived exertion in children with cerebral palsy when walking with
lower limb joints during human walking at different velocities. J
anterior and posterior walkers. Dev Med Child Neurol 1997;39:
Electromyogr Kinesiol 1996;6:177-90.
20. Meythaler JM, Guin-Renfroe S, Hadley MN. Continuously in-
37. Suzuki N, Shinohara T, Kimizuka M, Yamaguchi K, Mita K.
fused intrathecal baclofen for spastic/dystonic hemiplegia: a pre-
Energy expenditure of diplegic ambulation using flexible plastic
liminary report. Am J Phys Med Rehabil 1999;78:247-54.
ankle foot orthoses. Bull Hosp Jt Dis 2000;59(2):76-80.
21. Edrich T, Riener R, Quintern J. Analysis of passive elastic joint
38. Tantucci C, Massucci M, Piperno R, Grassi V, Sorbini CA.
moments in paraplegics. IEEE Trans Biomed Eng 2000;47:1058-
Energy cost of exercise in multiple sclerosis patients with low
degree of disability. Mult Scler 1996;2:161-7.
22. Lin CJ, Guo LY, Su FC, Chou YL, Cherng RJ. Common abnormal
39. Dietz V, Ketelsen UP, Berger W, Quintern J. Motor unit involve-
kinetic patterns of the knee in gait in spastic diplegia of cerebral
ment in spastic paresis. Relationship between leg muscle activa-
tion and histochemistry. J Neurol Sci 1986;75:89-103.
23. Brunner R, Krauspe R, Romkes J. [Torsion deformities in the
40. Pierrot-Deseilligny E. Electrophysiological assessment of the spi-
lower extremities in patients with infantile cerebral palsy: patho-
nal mechanisms underlying spasticity. Electroencephalogr Clin
genesis and therapy] [German]. Orthopade 2000;29:808-13.
24. Latash ML, Penn RD, Corcos DM, Gottlieb GL. Effects of intra-
41. O’Dwyer NJ, Ada L, Neilson PD. Spasticity and muscle contrac-
thecal baclofen on voluntary motor control in spastic paresis.
ture following stroke. Brain 1996;119:1737-49.
42. Ashworth B. Preliminary trial of carisprodol in multiple sclerosis.
25. Meythaler JM, Steers WD, Tuel SM, Cross LL, Haworth CS.
Continuous intrathecal baclofen in spinal cord spasticity. A pro-spective study. Am J Phys Med Rehabil 1992;71:321-7. Supplier
26. Meythaler JM, Guin-Renfroe S, Law C, Grabb P, Hadley MN.
a. Vicon Motion Systems, 14, Minns Business Park, West Way, Ox-
Continuously infused intrathecal baclofen over 12 months for
Arch Phys Med Rehabil Vol 84, May 2003
CAN – MKTG – TRADESHOWS / EVENTS VERSION 2.0 VER NO. DATE SEC NO. AMENDMENTS MADE PREPARED BY APPROVED BY 17-Apr-08 Initial Release Susan Goncalves Marketing Dept 15-June-08 Raquel Chan Marketing Dept Header & Marketing TRADESHOWS/EVENT PROCESS STANDARD WORK 1.0 Purpose The purpose of events is to strength the relationsh
Explanation of Blood Tests PLEASE NOTE: In keeping with our patient confidentiality standards, results of blood screenings performed by Cass County Memorial Hospital are provided only to you, the patient. We do not send the test results to your doctor. We encourage you to share this important health information with your primary care provider. This information is provided to help you
 INTRATHECAL BACLOFEN AND HEMIPLEGIA, Re´my-Ne´ris
INTRATHECAL BACLOFEN AND HEMIPLEGIA, Re´my-Ne´ris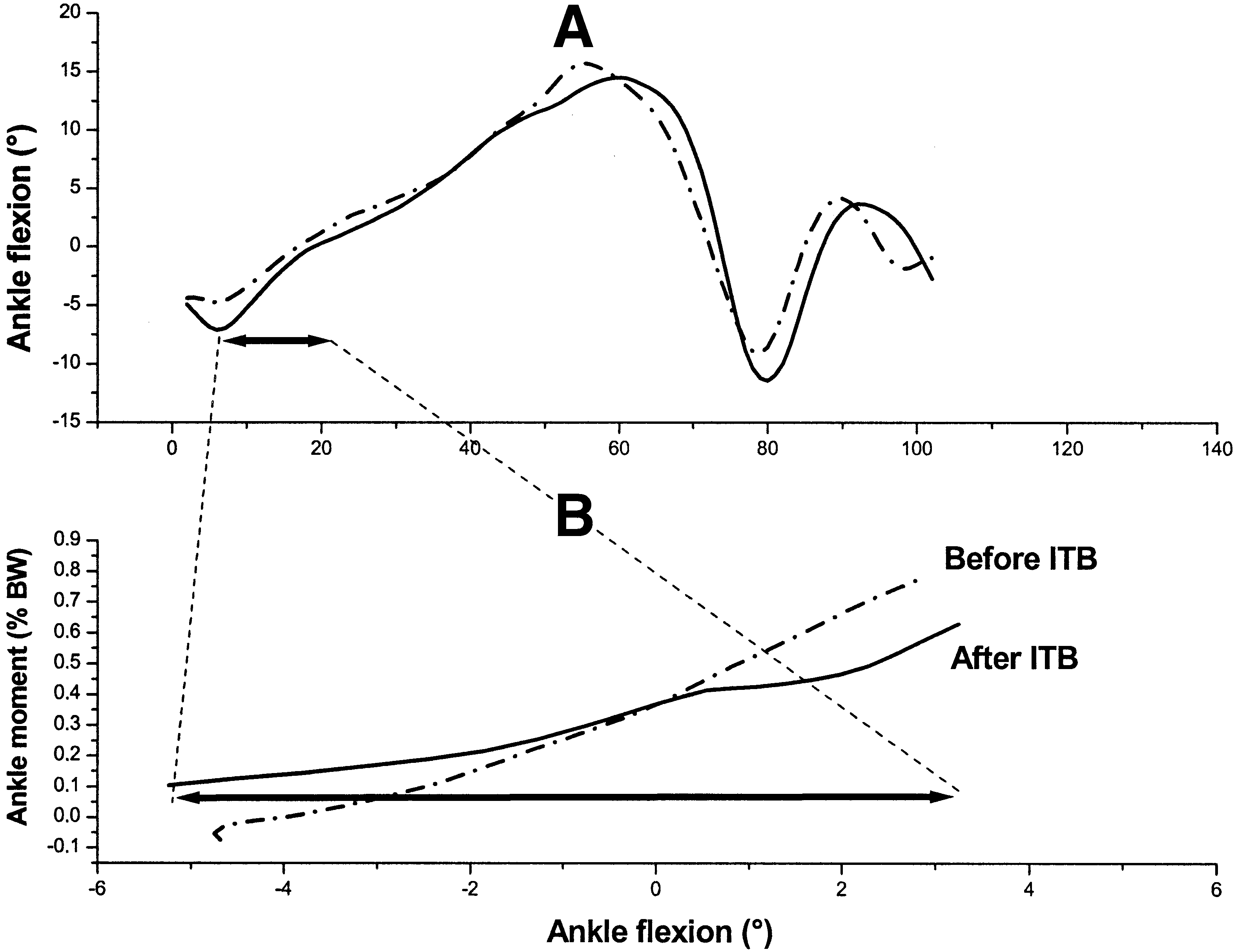
 INTRATHECAL BACLOFEN AND HEMIPLEGIA, Re´my-Ne´ris
INTRATHECAL BACLOFEN AND HEMIPLEGIA, Re´my-Ne´ris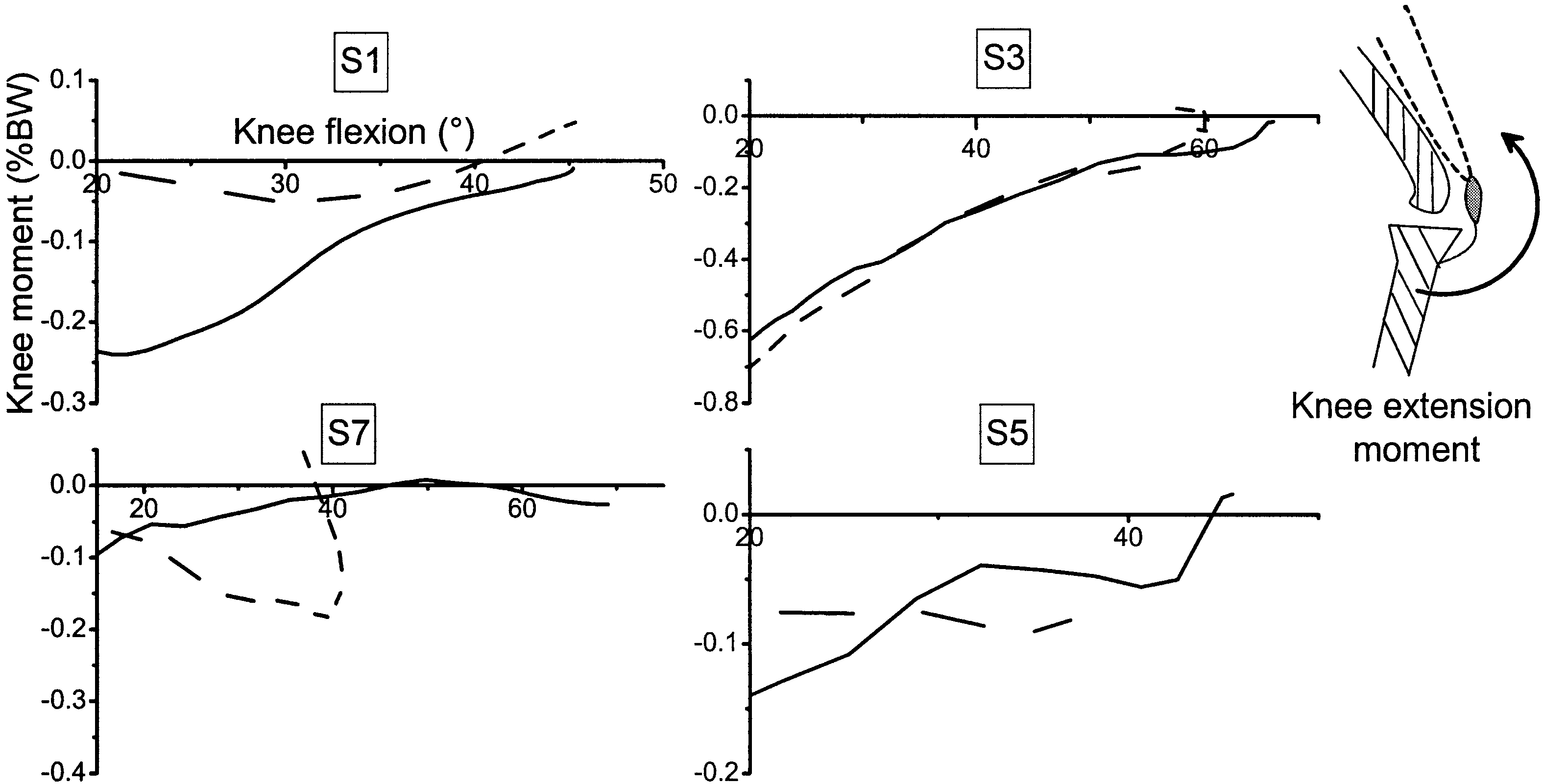
 INTRATHECAL BACLOFEN AND HEMIPLEGIA, Re´my-Ne´ris
INTRATHECAL BACLOFEN AND HEMIPLEGIA, Re´my-Ne´ris