Thank you, it's cool. Used for the first time because only then was the right drug. Very revealing detail: ordered Express shipping to get the order within 3 hours because didn't know how to get the order faster https://africarx.co.za/ The drug is authentic exactly. Consistent with the stated prices the Staff is knowledgeable.
Viagra 2-pop test.doc
Testing the Difference Between Proportions (p1 - p2)
BACKGROUND
VIAGRA is a prescription medicine that is used to treat male impotence. To protect American consumers, the U. S. Food and Drug Administration requires drug manufacturers to conduct clinical trials to demonstrate a drug’s safety and effectiveness. In applying for FDA approval for VIAGRA, Pfizer Pharmaceuticals, Inc. submitted the results of 21 separate clinical trials. The information below, obtained from the FDA web site 1,2, is part of the FDA’s summary of those clinical trials. VIAGRA received FDA approval on March 27, 1998.
Review this material, including the footnotes and explanatory remarks. You’ll perform a hypothesis test at the end of the document.
FDA SUMMARY
VIAGRA is used to treat impotence in men. VIAGRA increases the body’s ability to achieve and maintain an erection during sexual stimulation. VIAGRA does not protect you from getting sexually transmitted diseases, including HIV.
In clinical studies, VIAGRA was assessed for its effect on the ability of men with erectile dysfunction (ED) to engage in sexual activity and in many cases specifically on the ability to achieve and maintain an erection sufficient for satisfactory sexual activity. VIAGRA was evaluated primarily at doses of 25 mg, 50 mg and 100 mg in 21 randomized3, double-blind4, placebo5-controlled trials of up to 6 months in duration, using a variety of study designs (fixed dose, titration, parallel, crossover). VIAGRA was administered to more than 3,000 patients aged 19 to 87 years, with ED of various etiologies 6 (organic, psychogenic, mixed) with a mean duration of 5 years. VIAGRA demonstrated statistically significant improvement compared to placebo in all 21 studies.
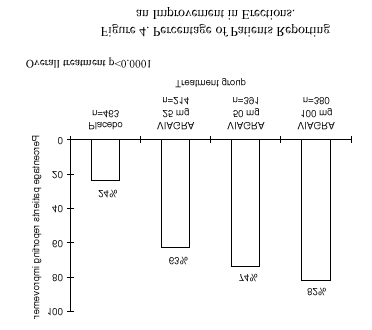
The frequency of patients reporting improvement of erections in four of the randomized, double-blind, parallel, placebo-controlled fixed dose studies (1797 patients) of 12 to 24 weeks duration is shown in Figure 4. Sixty-three percent, 74%, and 82% of the patients on 25 mg, 50 mg and 100 mg of VIAGRA, respectively, reported an improvement in their erections, compared to 24% on placebo.
1 http://www.fda.gov/cder/foi/label/1998/viagralabel2.pdf 2 http://www.fda.gov/cder/consumerinfo/druginfo/Viagra.htm
3 This means patients were randomly assigned to one of the four treatment groups.
4 This means that neither the patient nor the researcher knew whether the patient received Placebo or one of the three doses of VIAGRA.
5 This means that some patients were given a pill with no active ingredients, the other patients were given one of the three doses of VIAGRA. 6 The underlying cause of the patient’s impotence.
EXPLANATORY NOTES
The chart cites the percentage of patients in each treatment group that reported improvement of erections. For convenience, the percentages were cited as whole numbers. For example, the chart cites the improvement percentage for Placebo as 24%. Since we know there were 463 in the Placebo group, we can obtain the number of men with improvement by multiplying the percentage by the number in the Placebo group. This calculates as 111.12 (.24*463). We can infer that there were 111 out of 463, which is actually .2397408, which was rounded to 24% for the chart. Since we need to use the sample proportion in calculations when we perform a hypothesis test, we’ll use the more precise value .2397 rather than the rounded value. Similarly, the improvement rate for VIAGRA25 was .6308, for VIAGRA50 was .7391, and for VIAGRA100 was .8211.
The improvement rates plotted in the chart seem to indicate that VIAGRA was more effective than Placebo, and was even more effective at higher doses (50 and 100 mg). But recall that these are sample results, which may be biased. Although the sample improvement rate for VIAGRA25 was .6308, the true improvement rate could actually be higher or lower. Similarly, Placebo’s sample improvement rate was .2397, which could either overestimate or underestimate the true Placebo improvement rate.
Notice the text below the chart that says “Overall treatment p<0.0001.” Based partially on this small p-value, the FDA researchers concluded “VIAGRA demonstrated statistically significant improvement compared to placebo.”
In order to verify the FDA’s conclusion regarding VIAGRA’s effectiveness, we can perform hypothesis tests to determine whether the difference between the improvement rate for Placebo and for VIAGRA is significantly different (i.e., unlikely to be caused by sampling error). We can also perform tests to determine whether higher doses of VIAGRA have significantly h igher improvement rates than lower doses. We’ll focus on three hypothesis tests:
• Is the improvement rate for VIAGRA25 significantly different from the rate for Placebo? • Is the improvement rate for VIAGRA50 significantly different from the rate for VIAGRA25? • Is the improvement rate for VIAGRA100 significantly different from the rate for VIAGRA50?
Suppose we perform the first hypothesis test and find a significant difference between the improvement rates for VIAGRA25 and for Placebo. This would mean it is unlikely that sampling error could cause this large a difference (.2397 and .6308) if the true improvement rates for these two treatments were the same. We’d conclude that VIAGRA25 has a higher improvement rate and is more effective than Placebo.
On the other hand, suppose we perform the first hypothesis test and find that the rates aren’t significantly different. This would mean that it is possible that the improvement rate for VIAGRA25 and for Placebo are the same value (eg: .4555) and that sampling error caused the VIAGRA 25 improvement rate to be too high (.6308) and caused the Placebo improvement rate to be too low (.2397). We’d conclude that VIAGRA25 is not more effective than Placebo.
ASSIGNMENT
Although there are three hypothesis tests to do, perform the one assigned to you based on your Student ID (Social Security number) as described in the table below.
Perform this test… …if the last two digits of your StudentId are
Is the improvement rate for VIAGRA25 significantly
different from the improvement rate for Placebo?
Is the improvement rate for VIAGRA50 significantly
different from the improvement rate for VIAGRA25?
Is the improvement rate for VIAGRA100 significantly
different from the improvement rate for VIAGRA50?
Perform your assigned test in the space provided on the attached worksheet, showing all calculations. In step 5, use your choice of either method I or method II, and also calculate the p-value. Use the precise improvement rates of: Placebo = .2397, VIAGRA25 = .6308, VIAGRA50 = .7391, and VIAGRA100 = .8211.
NAME _________________ STUDENT ID________________
Is the improvement rate for VIAGRA25 Is the improvement rate for VIAGRA50 Is the improvement rate for VIAGRA100 significantly different from the significantly different from the significantly different from the improvement rate for Placebo? improvement rate for VIAGRA25? improvement rate for VIAGRA50?
1) Ho: pViagra25 - pPlacebo = 0 (no difference in rates)
1) Ho: pViagra50 - pViagra25 = 0 (no difference in rates)
1) Ho: pViagra100 - pViagra50 = 0 (no difference in rates)
Ha: pViagra25 - pPlacebo ≠ 0 (is a difference in rates)
Ha: pViagra50 - pViagra25 ≠ 0 (is a difference in rates)
Ha: pViagra100 - pViagra50 ≠ 0 (is a difference in rates)
3) Test statistic: __________ whose sampling distribution
3) Test statistic: __________ whose sampling distribution
3) Test statistic: __________ whose sampling distribution
4) Critical value(s) ___________________
4) Critical value(s) ___________________
4) Critical value(s) ___________________
6) The researcher [ can | cannot ] reject Ho and should
6) The researcher [ can | cannot ] reject Ho and should
6) The researcher [ can | cannot ] reject Ho and should
FROZEN COCKTAIL MACHINE INFORMATION Our twin barrel frozen cocktail machines add fun to any party! Delivered with 20 litres (10L in each barrel) of your choice of drink flavours – just add your own alcohol. Self serve means no more wasting time fixing your guests drinks. Less work and more time enjoying your own party, with no clean up! For your convenience, our Frozen Cocktail Machi
RESEARCH Time Savings Associated WithDispensing Unit-of-UsePackages Earlene E. Lipowski, DeArcy E. Campbell, David B. Brushwood, and Debbie Wilson Objectives: To determine how much time can be saved with the use of unit-of-use packaging in a community pharmacy, the distribu- tion of work between the pharmacist and the pharmacy technician when unit-of-use packaging is used, and the numb
 Testing the Difference Between Proportions (p1 - p2)
BACKGROUND
Testing the Difference Between Proportions (p1 - p2)
BACKGROUND