Thank you, it's cool. Used for the first time because only then was the right drug. Very revealing detail: ordered Express shipping to get the order within 3 hours because didn't know how to get the order faster https://africarx.co.za/buy-levitra-south-africa.html The drug is authentic exactly. Consistent with the stated prices the Staff is knowledgeable.
Microsoft word - cda spine new patient history.doc
CDA Spine New Patient History
Name _____________________________________ Age ________ Today’s Date __________
Primary Care Physician _______________________ Consult requested by _________________
1. My current pain developed: Gradually Suddenly Date of onset ___/___/_____
Motor vehicle accident Attorney:______________________________________________ Work injury: *If this is a work injury, please fill out the last page of this intake completely
2. My primary pain is located:_____________________________________________________ 3. If you have back or neck pain, does it radiate into your arm/leg? Yes No
100% in my 100% in my back or neck arm or leg
4. Please make a mark on the line below to show your average pain level over the past week. No
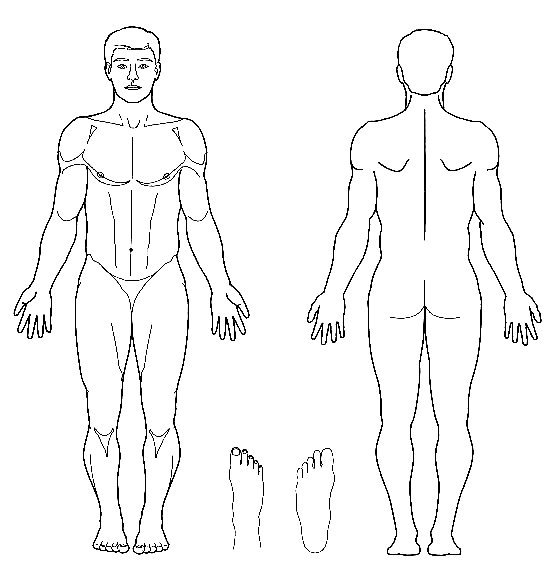
Please use the following key to shade in the distribution of your pain on the figures: Numbness ………. Pins and Needles 00000000 Pain ///////////////
5. My pain is best described as (check all that apply):
6. My pain is worse with (check all that apply): Bending forward
8. Have you experienced new bowel or bladder incontinence recently? Yes No 9. Please list all other physicians you have seen for this problem:
10. Have you had any of the following tests for the current problem? (date, location, and findings)
X-rays _________________________________________________________________
CT scan ________________________________________________________________ MRI ___________________________________________________________________ EMG __________________________________________________________________
Bone scan _______________________________________________________ Diagnostic Spinal Injections (e.g. epidural, facet/sacroiliac joint block, discogram)
_______________________________________________________________________ _______________________________________________________________________
11. I have tried the following treatments for my pain (Circle those that helped, X out those that didn’t):
Spinal Injections Home/gym exercises Surgery
12. I have tried the following medications for my pain (Circle those that helped, X out those that didn’t):
Anti-inflammatories ( Ibuprofen, Aleve, Naproxen, Mobic, Celebrex, Diclofenac, Steroids) Muscle relaxants ( Soma, Flexeril, Carbamazepime, Zanaflex, Skelaxin, Robaxin, Methocarbamol) Anti seizure drugs ( Neurontin, Gabapentin, Lyrica) Anti-depressants ( Paxil, Zoloft, Nortriptyline, Amitriptyline) Narcotics ( Lortab, Hydrocodone, Oxycodone, Oxycontin, Ultram, Vicodin, Percocet, Methadone)
Allergies: None Iodine Contrast dye Steroids Local Anesthetics Latex
Other:_________________________________________________________________
Allergic Reaction that occurred:____________________________________________ Current Medications and Dosages: _______________________ _________________________
_________________________ ________________________ _________________________ _________________________ ________________________ _________________________ _________________________ ________________________ _________________________ _________________________ ________________________ _________________________
Medical History: Please check the following medical problems you have now, or have had:
Have you had previous back or neck problems? □Yes □No If yes, please describe? ____________________________________________________________
Have your received care from a mental health professional? □Yes □No □Still seeing_______________Surgical History (include approximate dates): ____________________________________________________________________________________ ____________________________________________________________________________________ ____________________________________________________________________________________
Family History: Please check those illnesses that your family members have had
Hypertension Diabetes Neurologic Problems Heart Disease Cancer Arthritis
□Living □Deceased (Age) ____
Brothers/Sisters #Living ____ #Deceased ____
□Living □Deceased (Age) ____ Social History:
Do you now, or did you ever smoke? No Yes Packs per day?_____ Quit?_________ Do you drink alcohol?___________ No Yes daily rarely Do you now, or have you ever had a drug or alcohol problem? No
Vocational History: Employed Full Time
Years at current job:__________ Date last worked:___________ Rate your current job satisfaction: Very Satisfied Satisfied Indifferent Dissatisfied Have you ever been on disability? No Yes: ___________________________________
How physically demanding is your job? Check one.
□Very heavy ( lifting > 100 pounds) □Heavy ( lifting > 60 pounds) □Moderate (lifting > 30 pounds) □Light ( lifting > 10 pounds) Review of Systems:
Please check any of the symptoms you have had during the past year.
□Unintentional weight loss of >10 # If this is a work related injury, please provide the following information. If not, then leave blank and sign at bottom of the page.
What is the date of your work injury?____________ Have you filed a claim yet? Yes No Has it been accepted? Yes No
State:_____ Claim #_________________ Claims Manager:________________________________
Is there an attorney assisting you with this claim? Yes No Name:___________________________ Did you leave work after it happened? Yes No Where else were you treated for this injury?
How long have you been at your current job? ________________________________________________ Are you currently working? Yes No If no, date last worked:____________________________ Do you have any current work restrictions? Yes No Restrictions:__________________________ Name of the physician who has placed you on work restrictions or off work: _______________________ Have you ever had a worker’s compensation claim in the past: Yes No
Explain: __________________________________________________________________________
__________________________________________________________________________
Do you have any past injuries in the same location as your work claim? Yes No
Explain: __________________________________________________________________________
__________________________________________________________________________
The information I have provided in this document is true and accurate to the best of my knowledge.
AminoBlend ™ A Balanced Formula of 18 L-Crystalline Amino Acids DESCRIPTION in the amino-acid dependent synthesis of AminoBlend™ capsules, provided by Douglas neurotransmitters and other nitrogenous compounds Laboratories, contain a nutritionally balanced mixture of essential, conditionally essential, and important AminoBlend was formulated to provide optimal non-essential amin
Escuela N° 9-0 0 6 “Profesor Fran cisco H u m berto Tolosa”. San Martín 562 – Rivadavia – Mendoza. Tel: (02623) 442078 PROFESORADO DE LA EDUCACIÓN INICIAL CICLO LECTIVO 2006. CURSO: Segundo ESPACIO CURRICULAR: Música y su Didáctica - Módulo Régimen de cursado : segundo cuatrimestre Carga horaria: 5 horas cátedras Profesor: PARDO, Ana María. OBJET
 CDA Spine New Patient History
CDA Spine New Patient History