Ordered, immediately called back and the same day delivered the order.Very pleased with the work. Thank you for prompt and accurate work https://africarx.co.za/ great prices, delivered on the day of the order. Pleasant managers consult by phone.
Microsoft powerpoint - clever primary results aha 2011_final-nopw.pptx
Claudication Treatment Comparative Effectiveness: Authors:
Timothy P Murphy, Donald E. Cutlip, Judith G. Regensteiner, Emile R. Mohler III, David J. Cohen, Matthew R. Reynolds, Beth A. Lewis, Joselyn Cerezo, Niki C. Oldenburg, Claudia C. Thum, Alan T. Hirsch. Presenter:
Alan T. Hirsch, Chair, on behalf of the CLEVER Study Investigators
Acknowledgements and Disclosures Acknowledgements: The CLEVER Study was sponsored by the National Heart Lung and Blood Institute (grants HL77221 and HL081656), and also received financial support from Cordis/Johnson & Johnson (Warren, NJ), eV3 (Plymouth, MN), and Boston Scientific (Natick, MA). Otsuka America, Inc., (San Francisco, CA) donated cilostazol for all study participants throughout the study. Omron Healthcare Inc., Lake Forest, IL donated pedometers. Krames Staywell, San Bruno, CA, donated print materials for study participants on exercise and diet. Disclosures: Timothy P. Murphy, M.D.: Research grant support - Abbott Vascular, Cordis/Johnson&Johnson, Otsuka Pharmaceuticals; consultant - Microvention/Terumo, Inc.; David Cohen, M.D.: Research grant support - Medtronic. Boston Scientific, Abbott Vascular, Medrad; consultant - Medtronic, Inc.; Matthew R. Reynolds, M.D., M.Sc. : Consultant - Medtronic, Inc.; Alan T. Hirsch, MD.: Research Grant Support - Cytokinetics, Viromed, Abbott Vascular; consultant - Merck, Pozen, Novartis, AstraZeneca. Background
Claudication is the most frequent symptom of peripheral
artery disease (PAD), and is experienced by an estimated 2 million Americans
Current therapeutic options include home exercise;
supervised exercise; claudication pharmacotherapy (cilostazol); or endovascular procedures
Invasive stent procedures have not been shown to offer
better claudication improvement than supervised exercise; stenting is reimbursed, but supervised exercise is not
Patients with proximal (aortoiliac) PAD are often highly
symptomatic, and are generally considered ideal for stent revascularization
Study Objectives
1. To test whether aortoiliac stenting (ST) and supervised
exercise therapy (SE) are superior to optimal medical care (OMC) -- as measured by peak walking time (PWT) at 6 months -- in patients with claudication due to aortoiliac peripheral arterial disease (PAD).
2. If these comparisons are positive, to test whether
stenting is superior to supervised exercise for the same endpoint. Population
Moderate to severe claudication (2-11 min on Gardner treadmill protocol or up to 5.5 METS)
Hemodynamically significant aortoiliac PAD confirmed by
non-invasive vascular lab testing or advanced imaging
No other co-morbid diseases that limited walking
No critical limb ischemia (rest pain, non-healing wound or
SFA disease allowed and endovascular treatment
permitted by protocol, but not required in any patients
Treatment Strategies Optimal Medical Care (OMC): Cilostazol 100 mg bid as tolerated, written and oral advice
about exercise and diet, with monthly coordinator contact
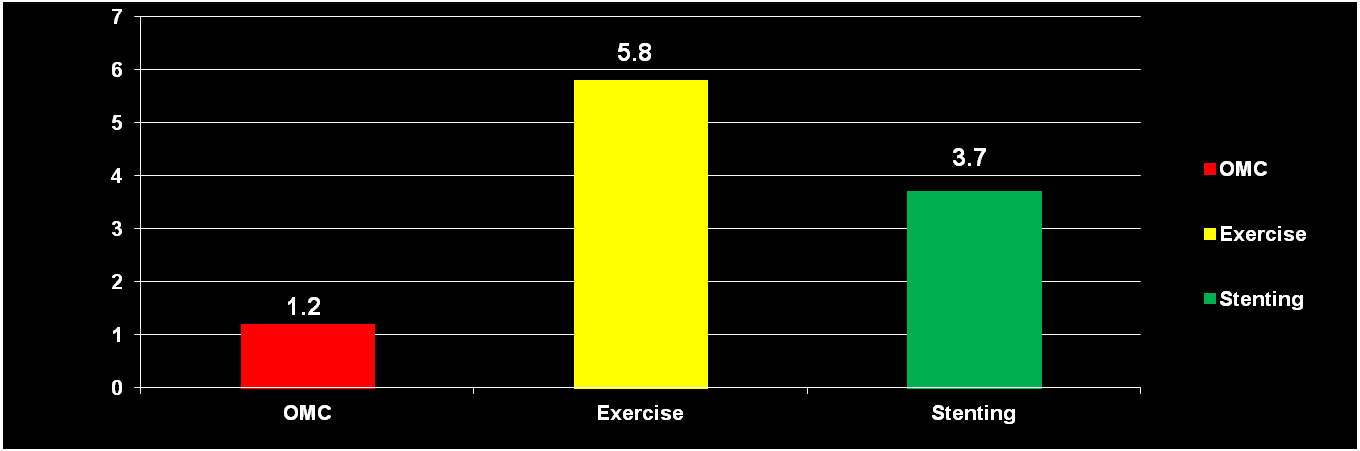
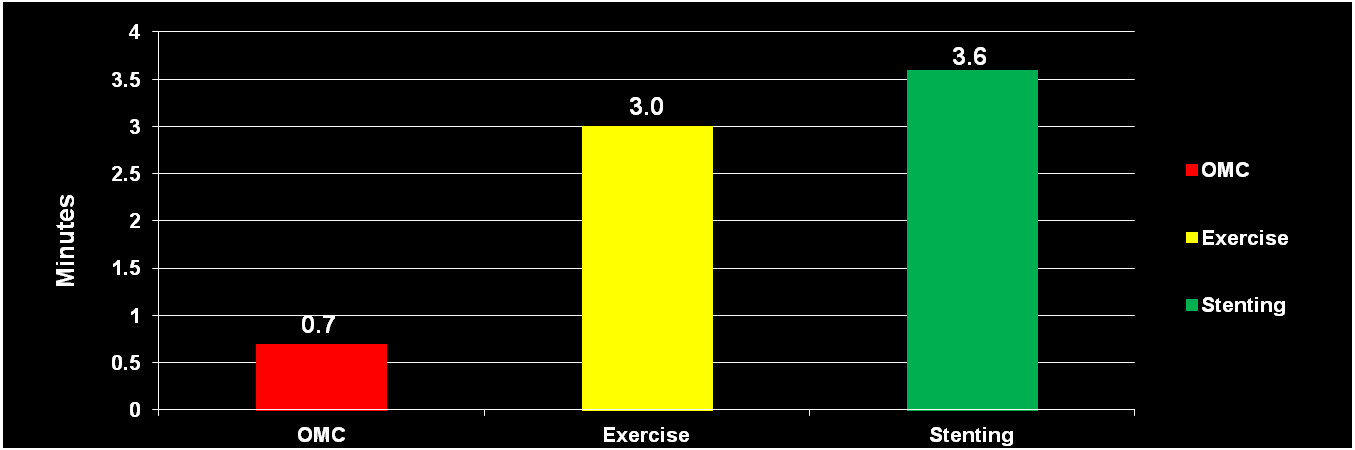
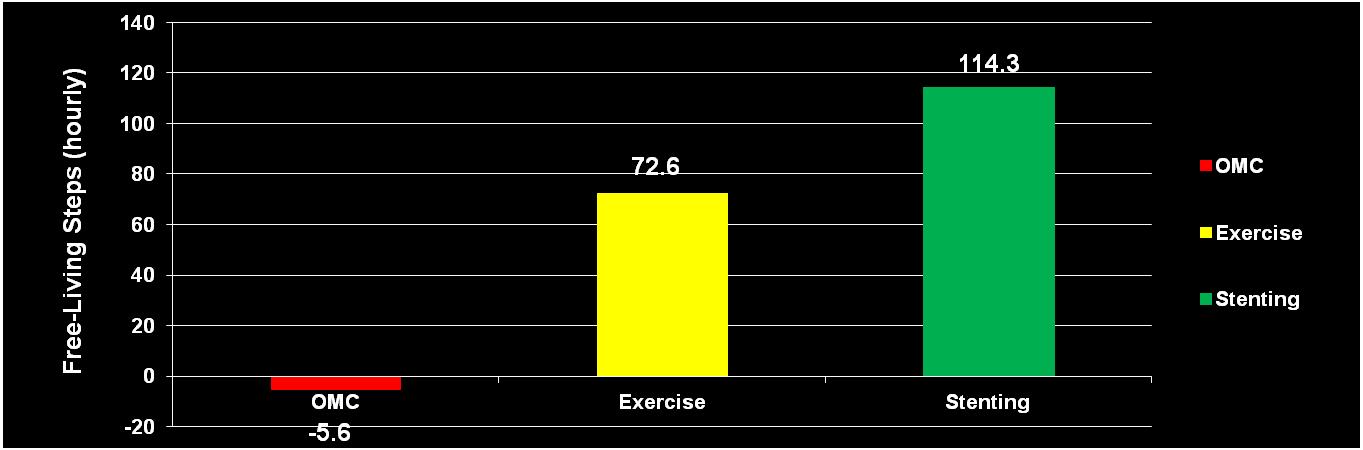
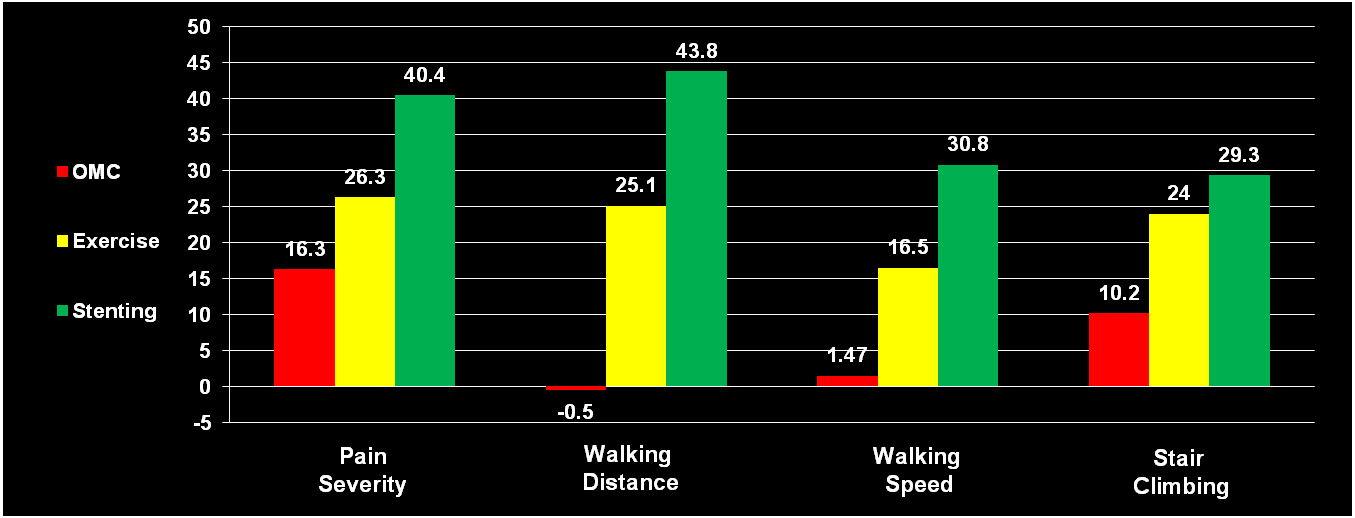
Supervised Exercise (SE): OMC plus 78 sessions of supervised exercise, 3x/wk, for 1 Stenting (ST): OMC plus stent revascularization of aortoiliac PAD Endpoints Primary Endpoint: Peak Walking Time (PWT) on a graded treadmill test Secondary Endpoints: Claudication Onset Time (COT) Community-based walking by pedometer Quality of life (QOL) by WIQ, PAQ, SF-12 Atherosclerosis biomarkers Primary Endpoint Assessed at Six (6) Months Eighteen (18) months long-term follow-up pending Demographic and Medical History Characteristics Age, years 62.4±8.0 64.1±9.5 64.9±10.2 Diabetes (%) Hypertension (%) Current smoking (%) Hypercholesterolemia (%) Prior stroke (%) Prior myocardial infarction (%) Prior use of cilostazol (%) Baseline Physiologic, Biochemical, and Anthropomorphic Characteristics Blood Pressure and ABI SBP (mmHg) DBP (mmHg) Ankle-Brachial Index 0.73±0.2 0.66±0.2 0.66±0.2 Biochemical Profile LDL (mg/dl) HDL (mg/dl) 48±15 0.94 Triglycerides (mg/dl) 147±142 HbA1c (%) 6.3±1.3 6.1±1.1 6.4±1.2 Anthropomorphic Characteristics 28.1±5.9 27.7±5.2 29.3±6.0 Waist Circumference (cm) Baseline Performance Characteristics Treadmill Walking PWT (minutes) 5.5±2.5 5.3±2.3 5.2±2.0 COT (minutes) 1.7±0.7 1.6±0.9 1.7±0.83 Community-based Walking Hourly Free-Living Steps 343±411 264±216 291±196 Treatment Delivery Cilostazol Compliance: >90% in all treatment groups Exercise Compliance: 71% Technical Success of Stenting: All ST patients successfully stented Pre-procedure mean lesion length 3.9±3.4 cm Mean stenosis 83±19%; post-procedure stenosis 5±8% ABI 0.66±0.2 at baseline, improved by 0.29±0.33 Crossover Rates: None at six months Primary Endpoint: Peak Walking Time Change from Baseline to Six (6) Months Pair-Wise Comparisons Difference (minutes) Exercise vs. OMC 4.6 (95% CI, 2.7-6.5) <0.001 Stenting vs. OMC 2.5 (95% CI, 0.6-4.4) Exercise vs. Stenting 2.1 (95% CI, 0.0-4.2) Claudication Onset Time Change from Baseline to Six (6) Months Pair-Wise Comparisons Difference (minutes) Exercise vs. OMC <0.003 Stenting vs. OMC Exercise vs. Stenting Community Walking Change from Baseline to Six (6) Months Pair-Wise Comparisons Difference (steps) Exercise vs. OMC Stenting vs. OMC Exercise vs. Stenting Walking Impairment Questionnaire Change from Baseline to Six (6) Months SE vs. OMC ST vs. OMC <0.001 <0.001 <0.001 Peripheral Artery Questionnaire Change from Baseline to Six (6) Months SE vs. OMC ST vs. OMC <0.001 <0.001 <0.001 Conclusions
In patients with moderate to severe claudication and
hemodynamically significant aortoiliac disease, supervised exercise offers better treadmill walking performance outcomes than stent revascularization
Both supervised exercise and stenting are more effective at
increasing walking distance compared to pharmacotherapy alone
Aortoiliac stent revascularization was associated with better
QOL scores than patients treated with supervised exercise, which is unexplained
Ongoing 18 month follow-up will provide greater insight into
the relative durability of these treatments, as well as the health economic impact
CLEVER Study Sites Rhode Island Hospital in Providence, RI (Tim Murphy) Henry Ford Hospital in Detroit, MI (Jonathan Ehrman) VA Ann Arbor in Ann Arbor, MI (Venkat Krishnamurthy) Aiyan Diabetes Center in Evans, GA (Janaki Nadarajah) University of Minnesota & Abbott Northwestern Hospital in Minneapolis, MN (Alan T. Hirsch) Jobst Vascular Center in Toledo, OH (Anthony Comerota) Torrance Memorial Medical Center in Torrance, CA (Mark Lurie) Vascular and Endovascular Specialist of Ohio in Mansfield, OH (William Miller) Ochsner Clinic in Metairie, LA (Olusegun Osinbowale) Spokane-Providence Medical Center in Spokane, WA (Stuart Cavalieri) St. Joseph Hospital in Orange, CA (Mahmood Razavi) Forsyth - Salem Surgical in Salem, NC (Ray Workman) Capital Health in Halifax, NS (Robert Berry) Johns Hopkins Hospital in Baltimore, MD (Elizabeth Ratchford) Stony Brook Hospital in Stony Brook, NY (Apostolos Tassiopoulos) University of Pennsylvania in Philadelphia, PA (Emile Mohler) Oregon Health Science University in Portland, OR (John Kaufman) Iowa Clinic in Des Moines, IA (John Matsuura) Peripheral Vascular Associates in San Antonio, TX (Jeffrey Martinez) Central Arkansas Veterans Health Care in Little Rock, AR (Mohammed Moursi)
SCRIPTURE: Luke 5:17-26 (to be read during the sermon) PP#1: A Healing Balm Is Raised “The Gospel is the power of God for the healing of everyone who believes.” -Romans 1:16 “A Healing Balm Is Raised” or “The Great Physician” PP#2: A child with hives all over the back. When Rebekah was little, we went to Hutchinson for supper at a buffet. When we wereheading over to the
The first publications about biphosphonates , which were initially named diphosphonates, were available in 1969, now more than 40 years ago. Biphosphonates are internalized by osteoclasts where they interfere with specific biochemical pathways (Russell, 2011). They enhance osteoclasts apoptosis and they inhibit osteoclasts attachment to the bone matrix (Dominguez et al., 2011). They are theref
 Claudication Treatment
Claudication Treatment  Acknowledgements and Disclosures
Acknowledgements and Disclosures Background
Background Study Objectives
Study Objectives Population
Population Treatment Strategies
Treatment Strategies Endpoints
Endpoints Demographic and Medical History Characteristics
Demographic and Medical History Characteristics Baseline Physiologic, Biochemical,
Baseline Physiologic, Biochemical,  Baseline Performance Characteristics
Baseline Performance Characteristics Treatment Delivery
Treatment Delivery



 Primary Endpoint: Peak Walking Time
Primary Endpoint: Peak Walking Time

 Claudication Onset Time
Claudication Onset Time

 Community Walking
Community Walking

 Walking Impairment Questionnaire
Walking Impairment Questionnaire


 Peripheral Artery Questionnaire
Peripheral Artery Questionnaire Conclusions
Conclusions
 CLEVER Study Sites
CLEVER Study Sites