Thank you, it's cool. Used for the first time because only then was the right drug. Very revealing detail: ordered Express shipping to get the order within 3 hours because didn't know how to get the order faster https://africarx.co.za/buy-levitra-south-africa.html The drug is authentic exactly. Consistent with the stated prices the Staff is knowledgeable.
Exporting.com.br
EIS Clinical Pre-Study of Stress-Related Erectile Dysfunction Clinical Investigator Professor Giuseppe Tritto Andrology Department St. Louis Hospital Paris, France Sponsor and Monitor Mr. Albert Maarek Site of Investigation St. Louis Hospital Paris, France Final Report May 15, 2005 Summary A test group of 37 male patients with erectile dysfunction (ED) undergoing consultation in the Andrology Department at St. Louis Hospital (Paris) were measured by a device called the Electro Interstitial Scanner (EIS) System.
All the patients presented neurovegetative dystonia with high stress levels and an increased level of catecholamine. None of the patients was undergoing treatment and no pathology was present.
The objective was to test the specificity and sensitivity of the ElectroScanGram (ESG), a graph generated by the EIS System, in reference to a patient database with stress-related ED and a control group of 30 subjects without evidence of stress.
Hypotheses The study was based on the following hypotheses:
The ESG graph can be used as a marker of stress and neurovegetative dystonia.
This hypothesis was validated by the statistical results:
A statistical study of the database (Mean Plot: Whisker using STATISTICA version 6.0) indicated that four values (2, 4, 15, and 17) of the ESG graph showed a sensitivity of 84%(IC calculated to 95%) in the stressed ED group, compared to the control group, with aspecificity of 87% (IC calculated to 95%).
The number of patients for this study is sufficient for a statistical analysis in order to calculate a level of specificity for the ESG graph.
This hypothesis was validated for the calculation of the specificity. However, for more accuracy regarding sensitivity, a meta analysis is necessary.
Justification Since the introduction of sildenafil citrate (Viagra®), increased reporting of erectile dysfunction has occurred, opening the way for more conversation on this controversial issue and most likely leading to increased prescribing of sildenafil. However, the origin of this problem is multifaceted, and treatment with sildenafil includes cardiovascular contraindications.
The EIS System was placed in the Andrology Department of St. Louis Hospital to begin a clinical investigation on erectile dysfunction (ED) related to significant stress. It is important to note that the patients were not diagnosed with any other pathology and were not undergoingtreatment. The EIS System The principle of the EIS System is the measurement of the conductivity of interstitial fluid locally and in vivo using the technique of bioelectric impedance. The EIS System uses DC current for access to interstitial fluid data. (16)
This measurement uses six tactile electrodes: Two on the forehead
From these six electrodes, 22 tissue volumes are measured and are recorded on a graph. The graphic display of the conductivity values of these 22 volumes is the ElectroScanGram (ESG). Tested hypotheses The questions raised for investigation were:
1. Would the EIS System offer the possibility of providing a marker for patients with stress or
2. Would the number of patients in this study be sufficient for a statistical analysis in order to
calculate specificity and sensitivity compared to a reference graph?
STUDY CONDITIONS Site of investigation The recordings took place in the Andrology Department at St Louis Hospital from January 7, 2005, to April 20, 2005. Subjects excluded Excluded from testing were patients who: Had skin lesions in contact with the electrodes or excessive perspiration
Were unable to be seated Had been fitted with metal pins or prostheses in the lower limbs or joints
Were undergoing specific treatments or taking certain medications (e.g., hypertensives,
Had a pathology that would have an influence on an erection
Patients recruited Two groups of patients were established:
Group 1: A control group of 40 men in supposed good health. This group was recruited from
hospital employees and their families. These subjects had no pathology, no ED disorders, and were not taking medications.
Group 2: All the patients in this group displayed chronic ED and evidence of stress. Like the
control group subjects, these patients had no diagnosed pathology and were undergoing no treatment.
The patients at St. Louis Hospital were addressed either by their practitioner or by direct consultation in the Andrology Department. Number of patients Forty male patients were selected in Group 1. They ranged in age from 23 years to 59 years. Thirty-seven male patients were selected to participate in Group 2 of this study. They ranged in age from 17 years to 60 years. Enlightened consent After the safety aspects and benefits of the study were presented to the patients, they signed an enlightened consent form. Monitoring Measurements were taken by the sponsor of the study, Mr. Albert Maarek. Confidentiality Due to patient confidentiality, identities of all the patients were kept anonymous and each patient was numbered by date of examination. Only clinical data were mentioned for each patient.
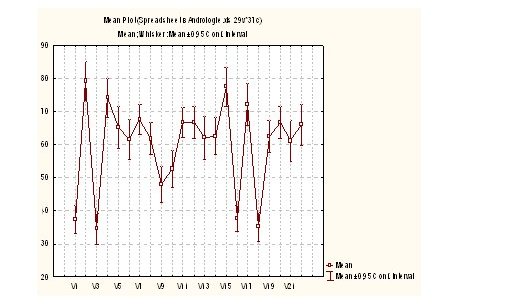
See below the statistical result analysis of the ESG graph carried out with the method Mean Plot: Whisker (program STATISTICA, version 6.0.) These graphs represent the average of the ESG graph of the two groups of patients. Group 1: Control group Group 2: ED patients (Summary plot)
The results of the graph group with stress and ED and the ESG graph of the control group determine a sensitivity of 84% (IC calculated to 95%) and a specificity of 87% (IC calculated to 95%). This sensitivity and specificity are related to the high values of the volumes 2, 4, 15 and 17 of the ESG graph. CONCLUSIONS
This study shows, with very high specificity, that the marker of stress, neurovegetative dystonia, and undoubtedly an important catecholamine rate should be the volumes 2, 4, 15 and 17 of the ESG graph. Hypothesis 1 is validated.
The number of patients (37) appears to be sufficient to determine the levels of specificity and sensitivity. Hypothesis 2 is also validated.
However, a future meta analysis with the recording of more pathologies will determine with more precision the sensitivity of obtained results. REFERENCES
Frôhlich, H., Ed., 1988. Biological Coherence and Response to External Stimuli. Springer-Heidelberg, Berlin
Nyboer, J., S. Bango, A. Barnett, and R.H. Halsey, 1940. Radiocardiograms—The electrical impedance changes of the heart in relation to electrocardiograms and heart sounds. J. Clin. Invest. 19: 963
Settle, R.G., B. Gutin, E. Presta, J. Wang, and T. Van Itallie, 1965. Estimation of human body composition by electrical impedance methods: A comparative study. Journal of Applied Physiology 58(5): 1565-1571
Bryan, K., 1991. Numerical recovery of certain discontinuous electrical conductivities. Inverse Problems 7: 827-840
Ikchata, M., 2000. On reconstruction in the inverse conductivity problem with one measurement. Inverse Problems 16: 785-793
Jackson, J.D., 1999. Classical Electrodynamics, 3rd Ed., John Wiley & Sons, New York
Lehmann-Horn, F., and K. Jurkat-Rott, 1999. Voltage-gated ion channels and hereditary disease. Physiol. Rev. 79(4): 1317-1372
Willumsen, N.J., M. Bech, S.-P. Olesen, B.S. Jensen, M.P.G. Korsgaard, and P. Christophersen, 2003. High throughput electrophysiology: New perspectives for ion channel drug discovery. Receptors and Channels 9(1): 3-12
Neher, E., 1992. Ion channels for communication between and within cells (Nobel Lecture). Neuron 8: 605-612
10) Owen, D., and A. Silverthorne, 2002. Channelling drug discovery. Current trends in ion
channel drug discovery research. Drug Discovery World 3(2): 48-61
11) Thomasset, A.L., 1995. Impèdancemètrie bio-electrique. Principes et applications cliniques.
12) Cole, K.S., 1968. Membranes, Ions, and Impulses. University of California Press,
13) Koryta, J., 1991. Ions, Electrodes and Membranes. John Wiley, Chichester
14) Brunswick, P., 2005. DDFAO/Rapport d’étude issue des tests cliniques sur la spécificité et
15) Cole, K.S., 1940. Permeability and impermeability of cell membranes for ions. Cold Spring
16) Kanai, H., K. Sakamoto, and M. Haeno, 1983. Electrical measurement of fluid distribution
in human legs; estimation of extra and intra cellular fluid volume. Journal of Microwave Power 18: 233-243
17) Meijer, J.H., P.M. de Vries, H.G. Goovaerts, P.L. Oe, A.J. Donker, and H. Schneider, 1989.
Measurement of transcellular fluid shift during haemodialysis. Part 1. Method. Medical and Biological Engineering and Computing 27: 147-151
18) Selye, Hans. A syndrome produced by diverse nocuous agents. Neuropsychiatry Clin.
Neurosci. 10: 230-231. 1998 American Psychiatric Press, Inc.
19) Cerqueira1, J., M. Moraes, and S. Glina, 2002. Erectile dysfunction: prevalence and
associated variables in patients with chronic renal failure. International Journal of Impotence Research 14: 65-71
James Bard, Senior Inspector: Mr. Bard has 12 years of experience in roadway construction. Mr. Bard is CTQP Florida Department of Transportation – District VI Certified and has experience in the following areas: Ms. Carol Cann, Professional Services Unit Letter of Response (Contract 13609) • Experience with the installation and relocation of CIMA is pleased to submit this Lett
T h e n e w e n g l a n d j o u r n a l o f m e d i c i n e This Journal feature begins with a case vignette highlighting a common clinical problem. Evidence supporting various strategies is then presented, followed by a review of formal guidelines, when they exist. The article ends with the author’s clinical recommendations. A 36-year-old woman with a long history of catamenia
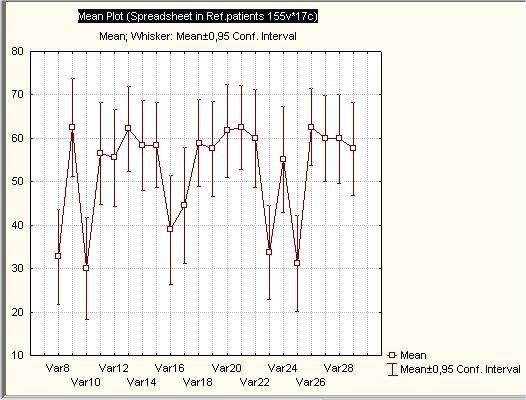 Group 1: Control group
Group 1: Control group