Ordered, immediately called back and the same day delivered the order.Very pleased with the work. Thank you for prompt and accurate work https://africarx.co.za/buy-cialis-south-africa.html great prices, delivered on the day of the order. Pleasant managers consult by phone.
Fellowships.asph.org
Title: Implementation of Isoniazid Preventive Therapy (IPT) in South Africa, 2011 J. C. Chehab *, K. Vilakazi-Nhlapo †, P. Vranken * A. Peters *, J. D. Klausner * * Centers for Disease Control and Prevention, South Africa † National Department of Health, Pretoria, South Africa
Running Head: Isoniazid Prophylaxis Therapy in South Africa
The authors have indicated that they have no financial relationships relevant to this
Corresponding Author Contact Information:
SETTING: Public Health Facilities in South Africa
OBJECTIVE: To assess the current implementation of Isoniazid Preventive Therapy
DESIGN: Cross-sectional study of 50 randomly selected facilities in South Africa.
Trained interviewers administered a standardized questionnaire per facility on aspects
of IPT policy, implementation and recording and reporting. We calculated and compared
descriptive statistics by province and facility type.
Of the 49 participating sites, 35 provided IPT (71%). By province: absent (0%) in all
Western Cape facilities, and available in few Mpumalanga (40%) and Limpopo (20%)
sites, resulting in 46% of eligible HIV-infected patients in February 2011 initiated on IPT.
Implementation by facility type was 27% among community health centers. Of facilities
with TB/HIV committees, 85% offered IPT compared to 59% of those without TB/HIV
committees (p=0.1217). Possession of the 2010 South African National IPT guidelines
was statistically significantly associated with sites providing IPT (84% versus 29%;
IPT implementation in South Africa, as of February 2011, has begun. TB/HIV on-site
committees and presence of guideline availability were strongly associated with IPT
uptake. More operational studies are needed to improve IPT implementation among
KEYWORDS: Tuberculosis; HIV; co-infection; integration; prevention
INTRODUCTION
Globally, the HIV and Tuberculosis (TB) epidemics are profoundly intertwined: HIV is
the leading risk factor associated with developing active TB, and the latter is the leading
cause of death and morbidity among HIV-infected individuals [1]. This is particularly
evident in South Africa, home to the highest number of HIV-infected patients and one of
the highest TB incidences worldwide [2]. Co-infection rates in South Africa are high with
as many as 80% of TB patients in Kwazulu-Natal province estimated to be HIV positive
Since the 1990s, several randomized clinical trials found Isoniazid Preventive Therapy
(IPT) to be effective in preventing active TB among HIV-infected individuals [4-7]. A
Cochrane review of 11 randomized trials showed a 33% protective effect of IPT against
active TB [8] and another study showed that protection increased to 64% among
individuals with positive Tuberculin Skin Tests (TST) [9]. In 1999, the World Health
Organization (WHO) recommended adding IPT to existing HIV care packages, and
initiating all HIV-infected individuals with confirmed latent TB infection or TB exposure
on IPT [10]. The newest WHO guidelines recommend that in settings with high rates of
TB transmission among HIV-infected individuals, all HIV-infected people where TB has
been ruled out should be initiated on IPT [11].
In 2010, the South African National Department of Health (NDOH) revised their
guidelines on Tuberculosis Prevention Therapy among HIV-infected individuals
accordingly, recommending that all eligible HIV-infected individuals be initiated
irrespective of TST [12]. Together with Infection Control and Intensive Case-Finding
policies, Isoniazid Preventive Therapy forms WHO’s Three I’s, and South Africa’s core
strategy to combat the spread of TB [11-14]. Despite an abundance of scientific
evidence and clear guidelines in place, IPT implementation has been slow worldwide,
with only 30,000 people living with HIV having started IPT in 2007 [1]. No national
assessment had been conducted since the revised guidelines to determine the level of
We aimed to assess the current implementation of IPT in South Africa.
STUDY POPULATION AND METHODS
We assessed 49 public medical facilities in high HIV prevalence districts in South
Africa’s nine provinces from March 1st to March 31st 2011.
A multistage sampling method was used. Firstly, we systematically selected the single
district in each province with the highest HIV prevalence. In Kwazulu Natal, two districts
were selected as it had the highest HIV prevalence and double the number of districts of
other provinces [15]. Secondly, each sub-district per selected district was assigned a
number and one sub-district randomly selected using the random number generator on
stattrek.com. Thirdly, all facilities per selected sub-district were assigned a number,
stratified by facility type- Community Health Center, Primary Health Clinic or District
Hospital. Using the random number generator mentioned above, a random sample of
three primary health clinics, one community health center and one hospital per sub-
district was chosen. This ratio was chosen to approximate the current distribution of
public medical facilities in South Africa. The lists of facilities used for this sampling was
provided by the South African National Department of Health.
We determined the availability of the latest national guidelines, as well as the presence
of dedicated TB/HIV committees within each facility. Those committees were defined as
specific on-site bodies to enable TB and HIV integration with management from both the
TB and HIV sections within each facility.
We also determined the training of staff in TB and HIV, defining trained staff as any
permanent facility staff trained in at least IPT and TB Infection control since January
Finally, we sought out the major reasons for not initiating patients on IPT. In an effort to
assess the quality of counseling offered, we asked each facility to report the four most
important facts about IPT that were covered in their counseling sessions. We defined
the four essential aspects of IPT as adherence, reporting of side effects, reporting of
symptoms of tuberculosis, and stopped or reduced alcohol intake during treatment.
A team composed of five members of the Centers for Disease Control and Prevention
and the South African NDOH created a standardized anonymous survey. The survey
contained questions on various aspects of IPT implementation, including guideline
availability, service provision, supply, and reporting and recording of routine data.
Ten teams of interviewers were trained by the Principal Investigator in the use of the
standardized questionnaire prior to the assessment. Each data collection team was
responsible for conducting the assessment in 5 sites.
The questionnaires were administered to the TB and HIV focal person in each selected
facility. Information reported by interviewees was systematically verified by collecting
routine data from facility registers for TB and HIV information.
Questionnaire data were directly entered into an Epi-Info 3.5.1 database for analysis
(Centers for Disease Control and Prevention, Atlanta, GA), and descriptive statistics
were calculated and compared by province and facility type, using Chi-Square.
The Centers for Disease Control and Prevention determined that the collection of
routine data and its analysis for this study was a non-research activity in accordance to
United States Federal regulations. Further, the South African National Department of
Health waived the need for local human subjects’ review.
Of the 50 facilities randomly selected, 49 (98%) participated in the survey. The missing
site was a facility in Northern Cape, which had merged with another selected site
situated on the same premises shortly prior to data collection.
Of the 49 participating facilities, 35 (71%) provided IPT. Implementation varied
significantly by province: none of the sites in Western Cape, 20% of Mpumalanga and
40% of Limpopo sites offered IPT. Table 1 shows the distribution by province among
Stratified by facility type, community health centers were the least frequent
implementers of IPT with only 56% of 10 offering IPT as opposed to 77% of 29 and 80%
of 10 public health clinics and district hospitals respectively.
Survey participants not implementing IPT (n=14) reported no clear guidance or
commitment from authorities (29%) and concerns of INH resistance (21%). Western
Cape followed national IPT guidelines but required that patients be given a Mantoux test
and be positive in order to be initiated on IPT. Regardless of Mantoux results, no patient
had been initiated on IPT in the five facilities assessed in that province in February
The 2010 National IPT guidelines were available in 39 (80%) out of the 49 participating
facilities. Table 1 shows little variation by province, with the notable exception of
Western Cape where none of the facilities had the latest guidelines. Of the survey
participants, 64% reported using the latest guidelines. Facilities having the 2010 IPT
guidelines were almost three times as likely to offer IPT than those who did not (84%;
In the month prior to the survey, 46% of eligible patients were initiated on preventive
therapy in the 35 facilities implementing IPT. Those 616 patients had been diagnosed
HIV-infected that month, screened negative for tuberculosis and were deemed eligible
to initiate therapy. Implementation by facility type was lowest among community health
centers where only 27% of eligible patients were initiated on INH.
Of the 49 facilities assessed, 38 (78%) had at least one staff member recently trained in
TB and HIV integrated services. Of facilities implementing IPT, 83% had at least one
recently trained staff. These figures stratified by province are shown in table 1.
75% of facilities had no doctors trained and 84% had at no nurses trained in TB and HIV
Out of our sample of 49 facilities, 20 (41%) had such committees. Facilities with TB/HIV
committees were more likely to offer IPT that those that did not among our sample (85%
versus 59%). There was great variation by provinces, and is shown in table 1.
All 35 facilities offering IPT also offered patients counseling prior to initiation on therapy.
Table 2 illustrates the distribution of counseling content among facilities providing
Of the 35 facilities providing counseling to IPT patients, 30 (86%) covered two or more
essential topics, 54% three topics or more, and only 6 (17%) covered all four essential
topics. Only 3% did not cover any of the essential topics. The four essential topics were
covered to varying degrees among those 35 facilities: 97% of them counseled on the
importance to adhere to the treatment for its entire duration, 66% on the need to
immediately report any side effects, 29% on the importance to immediately report any
signs or symptoms of TB, and only 9% on the need to reduce or stop alcohol intake
IPT data was recorded in 34 of the 35 (97%) facilities - the exception being one primary
health clinic in Mpumalanga. There was no official IPT register available for facilities at
the time of assessment, yet 20 of the 34 facilities (59%) had made their own allowing
them to record patient information and IPT data throughout treatment. Of those sites, 33
(97%) also reported IPT monthly statistics, except for one primary health clinic in North
West province. We investigated separately recording practices for ART patients, and
found that among the sites providing IPT (N=35), 27 (77%) initiated ART patients on
IPT. Recording of IPT information for ART patients among these facilities was poorer,
with only 21 of 27 sites (78%) doing so.
DISCUSSION
Our study assessed the implementation of IPT in South Africa in early 2011. Our data
shows that IPT is being partly implemented. We found that 71% of randomly selected
medical facilities implemented IPT and that in February 2011, 46% of eligible newly
diagnosed HIV-infected patients were initiated on preventive therapy. In this survey,
many of the sites not implementing IPT did so either because of lack of provincial policy,
guidance from authorities or fear of INH resistance. This lends support to current
literature indicating that facility staff’s concerns about INH resistance due to a failure to
rule out active Tuberculosis is a major barrier to IPT implementation [14-19]. Some of
those concerns might be due to inexperienced staff or other organizational barriers, and
some studies have suggested that clinical opinion leaders could be instrumental in
changing fears about INH resistance [20-22].
We found that facilities where the 2010 National IPT guidelines were available were
almost three times as likely to offer the preventive therapy, confirming findings that
developing operational guidelines and strong policy presence are essential for effective
The lack of association between recent staff training in TB and HIV integration and IPT
implementation was not expected. Overall, recent training in TB and HIV among core
staff in our sample sites was poor: although most surveyed sites had at least one
recently trained staff, only some facilities had at least one trained doctor or nurse. This
is of particular concern since the latter are key in initiating patients on ART and TB and
IPT treatment [9,27]. More training of public clinical facility staff is needed in TB and HIV
Further, while effective communication and joint decision-making between managers of
TB and HIV services on site seems paramount to efficient integration of these services,
only a minority of sampled sites had official TB/HIV coordination bodies. We did not find
an association between having TB/HIV committees and increased IPT uptake, but
believe that such an association would have been likely with a larger sample size.
The survey was a rapid assessment and thus included few facilities in each province,
limiting generalizability. The small sample size further limited the power of the survey,
and may have prevented us from finding statistical significance in differences that truly
did exist. The data suggest that greater sample size might have shown an association
between factors such as staff training in TB/HIV and on-site TB/HIV committees and
increased IPT uptake. In addition, facilities were selected in the districts with the highest
antenatal HIV prevalence, which might not be representative of areas with lower HIV
prevalence. We sought to maximize external validity through random sampling and
selecting a range of facility types in each province which approximated national
distribution. Finally, Kwazulu-Natal had twice the number of study sites selected
compared to other provinces, but also had double the number of districts compared to
most other provinces and the highest overall HIV prevalence in 2008 [15]. Northern
Cape only had four study sites as two of the facilities initially selected merged into a
single entity shortly before data collection.
Our study demonstrated that some progress is being made towards IPT implementation
in South Africa, where almost half of eligible patients were initiated in February 2011.
The presence of the latest guidelines, with their simplified algorithms to identify and
initiate eligible patients on IPT, was associated with better IPT uptake. The barriers to
IPT implementation were practitioner’s fear of INH resistance and lack of clear guidance
from authorities. Few of our survey participants had on-site TB/HIV committees and
recent TB/HIV training remained low, particularly among nurses and doctors. One of the
keys to efficient integration of TB and HIV services might be effective communication
between facility TB and HIV coordinators, and updated staff knowledge in TB and HIV
integrated services. Further studies are needed to investigate the effects of on-site
TB/HIV coordination bodies and staff training on IPT implementation.
Kgomotso Vilakazi-Nhlapo, Ntombi Mhlongo and Lorna Nshuti of the South African
National Department of Health were essential in obtaining the support from Provincial
Departments and liaising with medical facilities. We would like to thank all the selected
facilities and their staff for their time and participation that have made this survey
Table 1: Distribution TB/HIV services and policy in selected sites, South Africa, 2011
Province Table 2: Number of essential aspects of IPT covered in counseling (n=35) * 4 Essential topics included adherence; reporting side effects; reporting of tuberculosis signs/symptoms; alcohol reduction/elimination during treatment
1. World Health Organization (WHO). WHO Report 2009: Global tuberculosis
control – epidemiology, strategy, financing. WHO Geneva, Switzerland.
2. Ait-Khaled N, Alarcon E, Bissell K, Boillot F, Caminero JA, Chiang C-Y, et al.
Isoniazid Preventive Therapy for People Living with HIV: public health challenges
and implementation issues. Int J Tuberc Lung Dis 2009, 13(8):927-935.
3. Grant AD, Charalambous S, Fielding KL, Day JH, Corbett EL, Chaisson RE, et
al. Effect of routine Isoniazid preventive therapy on tuberculosis incidence among
HIV-infected men in South Africa: a novel randomized incremental recruitment
4. Whalen CC, Johnson JL, Okwera A, Hom DL, Huebner R, Mugyenyi P, et al. A
trial of three regimens to prevent tuberculosis in Ugandan adults infected with the
human immunodeficiency virus. Uganda–Case Western Reserve University
Research Collaboration. N Engl J Med 1997; 337: 801-8.
5. Pape J, Jean S, Ho J, Hafner A, Johnson W. 1993. Effect of Isoniazid
Prophylaxis of the Incidence of Active Tuberculosis and Progression of HIV
6. Halsey N A, Coberly JS, Desormeaux J, Losikoff P, Atkinson J, Moulton LH, et al.
Randomized trial of isoniazid versus Rifampicin and Pyrazinamide for prevention
of tuberculosis in HIV-1 infection. Lancet 1998; 351: 786-92.
7. Wilkinson D. Drugs for preventing tuberculosis in HIV infected persons.
Cochrane Database Syst Rev 2000; 4:CD000171.
8. Woldehana S, Volmink J. Treatment of latent tuberculosis infection in HIV
infected persons. Cochrane Database Syst Rev 2004; 1:CD000171.
9. Golub JE, Saraceni V, Cavalcante SC, Pacheco AG, Moulton LH, King BS, et al.,
et al. The impact of antiretroviral therapy and Isoniazid preventive therapy on
tuberculosis incidence in HIV-infected patients in Rio de Janeiro, Brazil. AIDS
10. Stop TB Partnership. The global plan to stop TB 2011–2015: transforming the
fight towards elimination of tuberculosis. Geneva, Switzerland: WHO, 2010.
11. World Health Organization (WHO): Guidelines for Intensified Tuberculosis Case
Finding and Isoniazid Preventive Therapy for People Living With HIV in Resource
Constrained Settings. Geneva, Switzerland: World Health Organization; 2010.
12. Republic of South Africa National Department of Health. The Guidelines for
Tuberculosis Preventive Therapy among HIV Infected Individuals. IPT Guidelines
13. Republic of South Africa National Department of Health. The National
Tuberculosis Control Programme. National Tuberculosis Policy Guidelines 2009.
14. Eldred LJ, Churchyard G, Durovni B, Godfrey-Faussett P, Grant AD, Getahun H,
et al. Isoniazid preventive therapy for HIV-infected people: evidence to support
implementation. AIDS 2010, 24 (suppl 5):S1-S3.
15. Charalambousa S, Grant AD, Innesa C, Hoffmann CJ, Dowdeswell Rob,
Pienaare J et al. Association of isoniazid preventive therapy with lower early
mortality in individuals on antiretroviral therapy in a workplace programme. AIDS
16. Durovni B, Cavalcante SC, Saraceni V, Vellozo V, Israel G, King BS, et al. The
implementation of isoniazid preventive therapy in HIV clinics: the experience from
the TB/HIV in Rio (THRio) Study. AIDS 2010, 24 (suppl 5):S49-S56.
17. Getahun H, Granich R, Sculier D, Gunneberg C, Blanc L, Nunn P. et al.
Implementation of isoniazid preventive therapy for people living with HIV
worldwide: barriers and solutions. AIDS 2010, 24 (suppl 5):S57-S65.
18. Dodd LE, Wilkinson RJ. Isoniazid preventive therapy in HIV infection. Lancet
19. Reid MJA, Shah NS. Approaches to tuberculosis screening and diagnosis in
people with HIV in resource-limited settings. Lancet Infec Dis 2009, 9:173-184.
20. Shishana O, Rehle T, Simbayi LC, Zuma K, Jooste S, Pillay-van-Wyk V, Mbelle
N, Van Zyl J, Parker W, Zungu NP, Pezi S & the SABSSM III Implementation
Team. South African national HIV prevalence, incidence, behavior and
communication survey 2008: A turning tide among teenagers? Cape Town:
21. WHO, UNAIDS, UNICEF. Towards universal access. Scaling up priority
HIV/AIDS interventions in the health sector. Progress report 2009. Geneva: WHO
22. Lester R, Hamilton R, Charalambous S, Dwadwa T, Chandler C, Churchyard GJ,
et al. Barriers to Implementation of Isoniazid Preventive Therapy in HIV Clinics: A
Qualitative Study. AIDS 2010, 24 (suppl 5):S45-48.
23. Date AA, Marco V, Granich R, Mazuwa B, Fox MY, Gilks C. Implementation of
co-trimoxazole prophylaxis and Isoniazid preventive therapy for people living with
24. Republic of South Africa Department of Health. Draft tuberculosis strategic plan
for South Africa, 2007-2011. http://www.doh.gov.za/tb/docs/stratplan/2007-
2011/tb/index.html [Accessed online July 20th, 2011].
25. Harries AD, Zachariah R, Corbett EL, Lawn SD, Santos-Filho ET, Chimzizi R, et
al. The HIV-associated tuberculosis epidemic – when will we act?. The Lancet
26. Churchyard GJ, Scano F, Grant AD, Chaisson RE. Tuberculosis preventive
therapy in the era of HIV infection: overview and research priorities. Journal of
Infectious Diseases 2007; 196 (Suppl 1):S52–S62.
27. Sanne I, Orrell C, Fox M, Conradie F, Ive P, Zeinecker J, et al. Nurse
management is not inferior to doctor management of antiretroviral patients: The
CIPRA South Africa randomized trial. Lancet 2010, 376(9734):33-40.
THE PROBLEM - The one how gives the thing away for free, because he I am addressing the problem that we are consuming or she don’t have to get rid of it him/her self. too much. So much that the environment can’t handle - The one who gets something he or she wants for free, it. This solution will also save the users money, at the because he or she gets it for free. same time I t
General Information - Influenza Vaccination The Disease: Influenza (flu) is caused by viruses. The fever, chills, headache, dry cough and muscle aches of flu may last from several days to more than a week, but complete recovery is usual. Certain groups of people, however, are much more likely to suffer major complications if they get the flu. People over age 65, residents of nursing hom
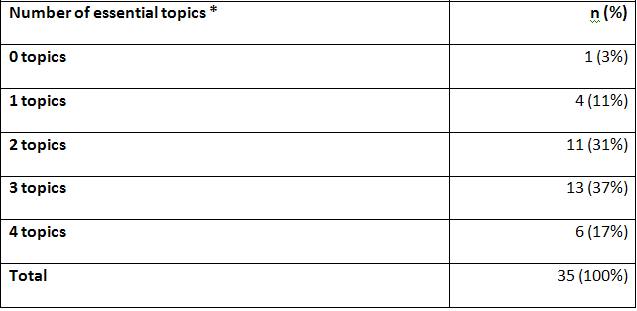 Table 2: Number of essential aspects of IPT covered in counseling (n=35)
Table 2: Number of essential aspects of IPT covered in counseling (n=35)