Thank you, it's cool. Used for the first time because only then was the right drug. Very revealing detail: ordered Express shipping to get the order within 3 hours because didn't know how to get the order faster https://africarx.co.za/ The drug is authentic exactly. Consistent with the stated prices the Staff is knowledgeable.
Fenadiabetes.org.ve
Approach to the Patient with Prediabetes
Med Star Clinical Research Center, Washington, D.C. 20003
Prediabetes consists of impaired fasting glucose and/or impaired glucose tolerance and is a significant risk factor for the development of type 2 diabetes, microvascular, and macrovascular disease. The values used to define prediabetes are arbitrary, because prediabetes represents an intermediary category along the continuum from normal glucose levels and tolerance to overt hyperglycemia. The progression from prediabetes to type 2 diabetes occurs over many years, strong evidence to support intervention to delay the progression from prediabetes to diabetes. Large, randomized prospective studies with lifestyle intervention and/or various modes of pharmacotherapy have demonstrated successful delay of diabetes. Several issues in the man- agement of prediabetes remain controversial, such as the role of pharmacotherapy and when to escalate treatment. This article will review some of the issues surrounding the identification and treatment of prediabetes, with an interpretation of the available data to help guide management. (J Clin Endocrinol Metab 93: 3259 –3265, 2008) A46-yr-old female is referred to you for an abnormal fasting andtotalcholesterolto175mg/dl(4.5mmol/liter).Byage54,the
glucose of 115 mg/dl (6.4 mmol/liter). She has no significant
patient’s weight steadily climbs to 68.2 kg (150 lb), and she reports
past medical history. She takes several vitamins but no prescribed
less diligence with her lifestyle changes. An OGTT reveals FPG of
medications. Her family history is remarkable for type 2 diabetes in
123 mg/dl (6.8 mmol/liter) with 2-h glucose of 252 mg/dl (14 mmol/
her father. Her physical examination is notable for a height of 152.5
liter) and HbA1c of 6.9%. The OGTT is repeated within 6 wk,
cm (60 inches), weight of 64.9 kg (142.8 lb), body mass index (BMI)
revealing a FPG of 148 mg/dl (8.2 mmol/liter) and 2-h glucose of
of 27.9 kg/m2, and blood pressure of 121/80 mm/Hg. A 75 gram
224 mg/dl (12.4 mmol/liter), consistent with a diagnosis of type 2
oral glucose tolerance test (OGTT) is performed to evaluate her for
diabetes. Her total cholesterol is 286 mg/dl (7.4 mmol/liter), LDL-c
undiagnosed diabetes, revealing a fasting plasma glucose (FPG) of
206 mg/dl (5.3 mmol/liter), HDL-c 42 mg/dl (1.1 mmol/liter), and
117 mg/dl (6.5 mmol/liter) and 2-h glucose of 153 mg/dl (8.5 mmol/
triglycerides 189 mg/dl (2.1 mmol/liter). She is started on metformin
liter). A hemoglobin A1c (HbA1c) is 6.4%, and lipid panel reveals
850 mg twice daily, a statin, and aspirin. Blood pressure is 138/80mm Hg, urine microalbumin level is normal, and she has no evi-
a total cholesterol of 278 mg/dl (7.2 mmol/liter), low-density li-
poprotein cholesterol (LDL-c) of 218 mg/dl (5.6 mmol/liter), high-density lipoprotein cholesterol (HDL-c) of 40 mg/dl (1.0 mmol/liter), and triglycerides of 99 mg/dl (1.1 mmol/liter). Intensivelifestyle recommendations, including a goal weight loss of 7%
Clinical question no. 1: What is prediabetes?
through a healthy low-calorie, low-fat diet and increased physical
Prediabetes broadly refers to an intermediate stage between com-
activity of 150 min/wk, are recommended. The patient is seen every
pletely normal glucose levels and the clinical entity of type 2
6 months with FPG performed semiannually and HbA1c and
diabetes, encompassing both IFG and impaired glucose tolerance
OGTT performed annually. Over the next few years, the patient
complied with the lifestyle recommendations and lost 6 kg (9%) of
As defined by the American Diabetes Association (ADA), pre-
her body weight, with fasting glucoses ranging from 95–108 mg/dl
diabetes is a FPG of at least 100 mg/dl (5.6 mmol/liter) but less
(5.3– 6 mmol/liter), HbA1c in the range of 6.1– 6.3%, and annual
than 126 mg/dl (7.0 mmol/liter), which is frequently termed IFG,
OGTT revealing isolated impaired fasting glucose (IFG). With this
or an abnormal 2-h response to a 75-g OGTT of at least 140
intervention, her LDL-c decreased to 115 mg/dl (3.0 mmol/liter)
mg/dl (7.8 mmol/liter) and less than 200 mg/dl (11.1 mmol/liter),
Abbreviations: ADA, American Diabetes Association; BMI, body mass index; DPP, Diabetes
Prevention Program; FPG, fasting plasma glucose; HbA1c, hemoglobin A1c; HDL-c, high-density lipoprotein cholesterol; 2hPG, 2-h postchallenge plasma glucose; IFG, impaired
Copyright 2008 by The Endocrine Society
fasting glucose; IGT, impaired glucose tolerance; LDL-c, low-density lipoprotein choles-
doi: 10.1210/jc.2008-1091 Received May 20, 2008. Accepted July 21, 2008.
terol; OGTT, oral glucose tolerance test; QALY, quality-adjusted life years.
J Clin Endocrinol Metab, September 2008, 93(9):3259 –3265
J Clin Endocrinol Metab, September 2008, 93(9):3259 –3265
which is often termed IGT. The World Health Organization de-
should prompt further investigation with a FPG or OGTT (14).
fines IGT similarly as the ADA, but IFG is defined at a fasting
Thus, in this patient, an initial FPG and HbA1c followed by an
glucose of at least 110 mg/dl (6.1 mmol/liter) (1, 2).
OGTT if FPG was less than 126 mg/dl (7 mmol/liter) and HbA1c
The definitions of diabetes and prediabetes are based on assess-
was less than 7% would complete her diagnostic evaluation. All
ments of disease risk as well as population distributions of plasma
were performed initially, confirming the patient’s diagnosis of pre-
glucose (2). Data suggesting a threshold of plasma glucose above
diabetes (IFG with IGT) and excluding the possibility of undi-
which the incidence of retinopathy significantly increases has been
used to help define diabetes (3, 4). This has been brought into ques-tion with recent data, with the Diabetes Prevention Program (DPP)showing that 7.9% of participants with IGT had findings consistent
Clinical question no. 3: What is the natural
with diabetic retinopathy, and 12.6% of patients with diabetes had
course of untreated prediabetes?
evidence of diabetic retinopathy early in the conversion to diabetes
The progression from prediabetes to type 2 diabetes occurs over
(5). In addition, the primary cause of morbidity and mortality in
many years before the development of overt hyperglycemia seen
diabetes is cardiovascular disease. Multiple prospective studies have
in diabetes (17). The risk of progressing to diabetes is greater in
demonstrated that cardiovascular events increase linearly with 2-h
individuals with both IFG and IGT compared with isolated IFG
postchallenge plasma glucose (2hPG) at levels well below the levels
or isolated IGT alone (10, 11). The risk of progressing to diabetes
diagnostic of diabetes. The DECODE (Diabetes Epidemiology:
depends on the degree of insulin resistance and deficiency of
Collaborative Analysis of Diagnostic Criteria in Europe) study, for
insulin secretion as well as other diabetes risk factors, such as age,
example, demonstrated a graded increase between 2hPG and car-
family history, overweight/obesity, or history of gestational di-
diovascular disease mortality and a J-shaped relation between fast-
abetes or polycystic ovary syndrome.
ing glucose and mortality (6). Such data suggest evidence of disease
The average annual risk of developing diabetes for someone
before the official diagnosis of diabetes. Thus, we should reconsider
with normoglycemia is approximately 0.7% per year (18). In con-
the approach of viewing isolated values of glucose with a threshold
trast, this risk is about 5–10% per year in individuals with IFG or
model, but instead view glucose as a continuous variable in risk
IGT (10). In the DPP, which enrolled subjects with elevated fasting
factor assessment for both cardiovascular and diabetic microvas-
glucose (’Ü95 mg/dl, or ’Ü5.3 mmol/liter) and IGT, 11% of indi-
viduals in the standard arm progressed to diabetes annually (19). Over the lifetime, a majority of patients with IFG, IGT, or both
Clinical question no. 2: Does this patient have
would develop type 2 diabetes in the absence of intervention. prediabetes at presentation?
Prediabetes is not only a significant risk factor for progression
to type 2 diabetes but is also considered a risk factor for mac-
This patient meets criteria for IFG, consistent with prediabetes, even
rovascular disease and for retinopathy. Some of this risk may be
before performing an OGTT. However, it is difficult to exclude the
associated with progression to overt diabetes, but there is still
possibility that this patient does not already have type 2 diabetes by
increased risk in individuals who have not yet progressed to
FPG alone. Fasting glucose alone is reported to miss the detection
diabetes. A metaanalysis of 38 prospective studies, for example,
of approximately 30% of cases of type 2 diabetes (2, 3, 7). This
suggests that postchallenge blood glucose levels in the nondia-
percentage may be even higher as reported in the Rancho Bernardo
betic range appear to have a linear relationship with cardiovas-
cohort and in the DPP. In the Rancho Bernardo cohort, 70% of
cular disease risk and a possible threshold risk with fasting
women and 48% of men aged 50 – 89 had new diabetes diagnosed
plasma glucose of about 100 mg/dl (5.6 mmol/liter) (20).
on the basis of an elevated 2-h plasma glucose alone (8). In the DPP,87% of cases of new diabetes were detected based on initial eleva-tion of 2hPG, as opposed to only 34% that were detected based on
Clinical question no. 4: What is the evidence supporting intervention for prediabetes, and
Upon presentation, an OGTT should be considered to defini-
does treatment alter the natural course of
tively diagnose whether the patient has prediabetes or has unrec-
prediabetes?
ognized type 2 diabetes mellitus. Diagnosis impacts prognosis, be-cause patients diagnosed with both IFG and IGT develop diabetes
There is ample evidence that intensive lifestyle intervention and
approximately twice as often as individuals with either isolated IFG
various modes of pharmacotherapy reduce the risk of progres-
or isolated IGT (10, 11). In addition, cardiovascular risk is greater
sion to diabetes, but is the progression to diabetes truly being
in those with IGT or diabetes based on the 2hPG (6, 12). The
prevented, or is the hyperglycemia of diabetes being treated
OGTT, however, requires additional time and resources, is
early? Are the treatment interventions sustainable? And finally,
considered less reproducible than the FPG, and thus would
is there any impact of treatment of prediabetes on long-term
require an additional confirmatory test if abnormal (9, 13).
microvascular and macrovascular comorbidities?
Alternatively, there is growing acceptance for the role of HbA1c
in the screening, diagnosis, and prognosis of diabetes (14 –16). Ac-
Lifestyle approaches or metformin therapy for diabetes
cording to a recent panel recommendation, an HbA1c of 7% or
prevention?
higher would suggest the presence of diabetes, along with a confir-
Lifestyle changes have consistently demonstrated benefit in pre-
matory test, whereas an elevated HbA1c of at least 6.5– 6.9%
venting or delaying the progression from IGT to diabetes. The Chi-
J Clin Endocrinol Metab, September 2008, 93(9):3259 –3265
nese Da Qing study of more than 500 IGT subjects was one of the
25%, suggesting the possibility that metformin was not just
first to show the benefit of long-term diet and exercise intervention
masking a diagnosis of diabetes but also helped to delay the
to prevent diabetes (21). Both the Finnish Diabetes Prevention
progression of prediabetes (25). Whether metformin was really
Study and the DPP demonstrated a 58% reduction in the progres-
changing the natural history of the disease would have been
sion from IGT to diabetes with intensive lifestyle changes compared
better delineated if the washout period had been longer.
with standard lifestyle advice (19, 22). In the DPP, lifestyle inter-
Does the combination of lifestyle intervention and metformin
vention with a goal of at least 7% weight loss and at least 150 min
confer additive benefit? The Indian Diabetes Prevention Pro-
of physical activity per week appeared to have greater impact on
gramme (IDPP-1), which showed a very high progression rate to
older persons and those with a lower BMI (19). With a BMI goal of
diabetes of 55% over 3 yr in subjects with IGT, evaluated the
less than 22 kg/m2 in the intensive lifestyle group compared with less
combination of metformin with intensive lifestyle changes com-
than 24 kg/m2 in the standard group, a Japanese study in males with
pared with either treatment alone. Although the tolerated level of
IGT resulted in a 67.4% risk reduction in diabetes over 4 yr (23).
metformin was only 250 mg twice daily compared with the 850
The interventions involved are intense, and require a firm
mg twice daily in the DPP, a combination of metformin with
commitment from patient, provider, and society alike. Even with
lifestyle change had no additional benefit compared with the
the multifaceted approach of lifestyle intervention in the DPP,
treatment with either metformin or lifestyle changes alone (26).
only 38% of the participants in the lifestyle intervention group
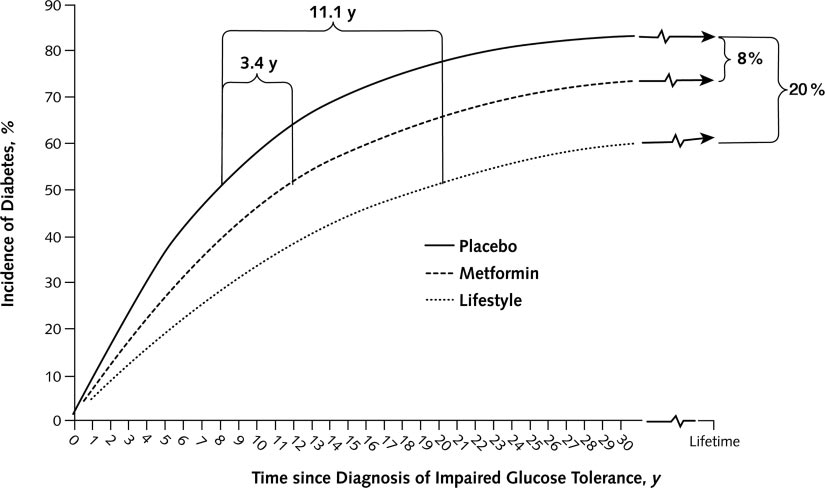
Computer modeling from the DPP estimates that over a lifetime,
achieved the weight loss goal of at least 7% at the end of the
83% of participants treated with standard intervention would de-
study, while only 58% met the goal of at least 150 min of mod-
velop diabetes, compared with 63% of those treated with lifestyle
erate intensity activity (19). Yet, there was clear benefit in the
intervention and 75% of those treated with metformin. Lifestyle
intervention. Encouraging is the follow-up of the Finnish Dia-
intervention would delay the onset of diabetes by 11.1 yr, and met-
betes Prevention Study, in which participants were followed for
formin would delay the onset of diabetes by 3.4 yr (Fig. 1). Lifestyle
an additional median 3 yr after the 4-yr intervention period. No
intervention would increase life expectancy by 0.5 yr and reduce the
diet or exercise counseling was provided in the annual follow-
incidence of blindness by 39%, end-stage renal disease by 38%,
up visits. During the total follow-up, the intervention group
amputation by 35%, stroke by 9%, and coronary heart disease by
maintained a 43% reduction in relative risk of developing dia-
8% (27). Supportive of this, both traditional (hypertension and
betes compared with the standard control group. The risk re-
dyslipidemia) and nontraditional (C-reactive protein and fibrin-
duction was greatest, however, in those who maintained the life-
ogen) risk factors were significantly reduced with intensive
style goals of weight loss, reduced fat intake, increased fiber
lifestyle treatment in the DPP (28, 29).
intake, and increased physical activity (24).
Despite such intriguing data from computer modeling, im-
On the other hand, metformin at 850 mg twice daily resulted
provements in long-term health outcomes (i.e. mortality and re-
in a 31% reduction in progression to diabetes in the DPP, being
duction in cardiovascular events) from diabetes prevention ef-
more effective in younger individuals and in participants with a
forts have yet to be proven. The longest follow-up outcomes
higher BMI (19). In addition, after a 1- to 2-wk washout period,
study to date is the Da Qing Diabetes Prevention Outcome Study,
metformin demonstrated a persistent reduction in diabetes by
evaluating participants 14 yr after the initial 6-yr intervention
FIG. 1. Simulated cumulative incidence of diabetes among adults with impaired glucose tolerance by the Diabetes Prevention Program treatment group. [Reproduced with permission from W. H. Herman et al.: Ann Intern Med 142:323, 2005 (27) American College of Physicians.]
J Clin Endocrinol Metab, September 2008, 93(9):3259 –3265
period. Participants in the intensive lifestyle intervention arm
Back to the patient . . . clinical question no. 5:
sustained a 43% reduction in diabetes incidence over the 20-yr
Should this patient’s prediabetes be treated?
period. There was no reported difference in cardiovascular dis-ease events or mortality, although the study had limited power to
The evidence is undisputable that diabetes can be delayed or
prevented by either intensive lifestyle modification and/or a va-riety of pharmacotherapies. This patient should have her predi-
Pharmacological intervention in diabetes prevention
abetes addressed, diabetes diagnosed or excluded, and should be
Other methods of pharmacotherapy have also demonstrated
treated. The risks of treatment, particularly with lifestyle inter-
prospective benefit in disease prevention. Acarbose was associ-
vention, are low and the benefits extend beyond the prevention
ated with a 25% reduction in progression from IGT to diabetes
of diabetes. In addition, lifestyle intervention is a highly cost-
after 3 yr in the STOP-NIDDM (Study to Prevent Non-Insulin-
effective method of treating prediabetes. Elegant cost analyses of
Dependent Diabetes Mellitus) trial. This effect disappeared with
the DPP showed that compared with placebo, lifestyle interven-
discontinuation of the acarbose, suggesting that acarbose may
tion would cost $635 more over a lifetime and produce a gain of
have masked the progression to diabetes (31). This trial also
0.57 quality-adjusted life years (QALY), or a cost per QALY
demonstrated a 49% relative risk reduction in cardiovascular
gained of about $1100. The estimated cost per QALY gained for
disease with acarbose, reduction in hypertension, and a reduc-
metformin intervention extended over the lifetime compared
tion in progression of carotid intima-media thickness (32, 33).
with placebo was approximately $31,300 but was substantially
These data suggest that maintenance of normoglycemia may help
lower at $1755 if the cost of generic metformin was substituted
prevent long-term macrovascular morbidity.
in the calculation (27). Eddy and colleagues (43) have estimated
The most enticing data to suggest a biological delay in the pro-
higher cost-effectiveness ratios, but several other models have
gression from prediabetes to diabetes with pharmacotherapy are
now demonstrated the relative cost-effectiveness of lifestyle in-
from Buchanan and colleagues (34, 35). In both the TRIPOD (Tro-
terventions as well as metformin (44).
glitazone in Prevention of Diabetes) and PIPOD (Pioglitazone in
Thus, there is no significant deterrent to treating this patient’s
Prevention of Diabetes) studies in Hispanic women with a history
prediabetes, and a detailed conversation between provider and
of gestational diabetes, Buchanan et al. (34, 35) showed that tro-
patient should ensue. Factors such as the availability of resources
glitazone and pioglitazone, respectively, stabilized pancreatic ␤-cell
for participation in an intensive lifestyle program and the pa-
function compared with placebo. Women in the placebo arm of
tient’s commitment of time toward dietary and lifestyle changes
TRIPOD had a decline in ␤-cellfunction.Pioglitazonestabilizedthis
should be reviewed. If pharmacotherapy is considered, a detailed
decline in ␤-cell function in the PIPOD study, and this effect per-
discussion of the goals, available data, and potential side effects
sisted after an extended washout period of the pioglitazone (35).
The TRIPOD and PIPOD studies also demonstrated decrease incarotid intima-media thickness with troglitazone and pioglitazone,respectively, suggesting a cardioprotective effect (36, 37). Clinical question no. 6: How should
In the DREAM study (Diabetes Reduction Assessment
prediabetes be treated?
with Ramipril and Rosiglitazone Medication), rosiglitazoneincreased the regression of IFG or IGT to normoglycemia and
Published guidelines on the approach to the patient with predi-
reduced the incidence of the composite outcome of diabetes or
abetes include a consensus statement from the ADA, the Indian
death by 60% over 3 yr (38). After a washout period, the
Health Services (IHS) Guidelines for care of the adults with pre-
incidence of diabetes in the placebo and rosiglitazone groups
diabetes and/or metabolic syndrome, and a position statement
were similar (39). Of note, rosiglitazone also reduced the risk
from the Australian Diabetes Society and Australian Diabetes
of renal disease, suggesting that maintenance of normoglyce-
Educators Association (Table 1). The recommendations on
mia may impact development of microvascular disease (40).
treatment of prediabetes differ slightly. The ADA consensus
Although there was no effect on cardiovascular outcomes,
statement stratifies therapy based on whether the patient has
there was an increase in congestive heart failure events com-
isolated IFG, isolated IGT, or a combination of IFG and IGT,
pared with placebo (0.5 vs. 0.1%) (38). The increased risk of
allowing for consideration in differences in the underlying phys-
weight gain, congestive heart failure, fractures (41), and cost
iology and disease progression. Lifestyle modification with a
associated with rosiglitazone must be weighed against its po-
weight loss goal of 5–10% is recommended along with moderate
physical activity of about 30 min daily. Recommendations for
The recently reported ACT NOW (ACTos NOW for the Pre-
use of metformin are tailored around individuals who may have
vention of Diabetes) study demonstrated a remarkable 81% re-
greater benefit from metformin as seen in the DPP and those who
duction in the conversion of IGT to type 2 diabetes over a mean
are at greater risk of progression to diabetes. Thus, metformin is
2.6 yr with pioglitazone compared with placebo. Improvements
considered in individuals less than 60 yr of age, individuals with
in insulin sensitivity and ␤-cell function were seen despite a
a BMI of at least 35 kg/m2, and individuals with increased risk
weight gain of 3.9 kg with pioglitazone compared with 0.8 kg
such as family history of diabetes in first-degree relatives, ele-
with placebo. The results from the washout period will help
vated triglycerides, reduced HDL-c, hypertension, or HbA1c
determine whether the improvements seen were due to biological
more than 6.0% (11). The IHS guidelines similarly advocate
delay of diabetes or early treatment of hyperglycemia (42).
lifestyle changes with consideration for metformin on an indi-
J Clin Endocrinol Metab, September 2008, 93(9):3259 –3265
TABLE 1. Key features of selected published recommendations on prediabetes Indian Health Services Australian Diabetes Society Guidelines for care of adults and Australian Diabetes with prediabetes and/or the Educators Association ADA consensus statement metabolic syndrome in position statement (2007) (11) clinical settings (2006) (45) (2007) (46)
mmol/liter) with 2hPG Ͻ140mg/dl (7.8 mmol/liter)
(7.8 mmol/liter) but Ͻ200mg/dl (11.1 mmol/liter)
Individuals with risk factors for diabetes
elevated triglycerides, reduced HDL-c, hypertension, HbA1c Ͼ6.0%
vidualized basis (45). The Australian guidelines recommend life-
Clinical question no. 7: When should one
style intervention as first-line therapy for a minimum of 6 months
escalate interventions for prediabetes?
before consideration of pharmacotherapy (46).
Inthispatient’scase,intensivelifestylechangeswererecommended,
The issue of when one should escalate intervention depends on
and the patient’s commitment to these changes were reviewed. Met-
the goals of treatment of prediabetes. Is the primary goal com-
formin therapy was not considered as initial therapy but may be con-
plete normalization of glucose levels or rather deterring progres-
sidered in higher-risk patients as outlined by the ADA. Metformin was
sive ␤-cell dysfunction? How will the primary goal reduce long-
added when there was clear evidence of glycemic deterioration, or
term mortality and morbidity? We look toward goals in type 2
progression of underlying disease, as evidenced by increase in FPG,
diabetes to address these important questions. In their 2006 joint
increase in HbA1c, and increase in 2hPG.
consensus statement, the ADA and the European Association for
If pharmacotherapy for prediabetes is initiated, it is im-
the Study of Diabetes (EASD) espoused an HbA1c goal as close
portant for both patient and provider to realize that any ther-
to the nondiabetic range as possible, or at least less than 7%. The
apy will require a long-term commitment. In addition, it is
consensus statement recommended a “call to action to initiate or
important to review with the patient that there are limited data
change therapy” for an HbA1c of at least 7% (47). This HbA1c
demonstrating the long-term health benefits of pharmacolog-
recommendation was based on issues of practicality and pro-
ical intervention compared with lifestyle intervention. Fur-
jected reduction in long-term complications. However, the re-
thermore, one might debate which drug is the appropriate
cent ACCORD (Action to Control Cardiovascular Risk in Dia-
choice. The use of metformin is supported by its relative
betes) trial also brings to light issues of safety in intensification
safety, cost effectiveness, and long-term data in the DPP. The
of therapy. In this trial of more than 10,000 subjects with type 2
ideal pharmacological intervention must demonstrate long-
diabetes, intensive therapy with a goal HbA1c less than 6.0%
term safety, health benefit (reduced incidence of diabetes, ma-
compared with a standard HbA1c goal of 7.0 –7.9% resulted in
crovascular and microvascular complications, and mortality),
increased mortality after a mean 3.5 yr of follow-up (48). Given
cost effectiveness, and the ability to halt the biological pro-
these findings, reasonable goals in prediabetes include 1) pre-
gression from prediabetes to diabetes. These factors will re-
vention of glycemic deterioration as an indicator of preservation
main the subject of current and future research endeavors in
of ␤-cell function and 2) modification of nonglycemic risk factors
(e.g. dyslipidemia and hypertension) to minimize long-term car-
J Clin Endocrinol Metab, September 2008, 93(9):3259 –3265
diovascular risk. Should this involve pharmaceutical interven-
and provider commitment to diagnosis and treatment, and level
tion, safety and avoidance of hypoglycemia are imperative.
of adherence with recommended treatment. Although there may
Which measures would alert the practitioner to deterioration
be debate on the details of management of prediabetes, there is
of glycemic control, or need for further intervention, over time?
no longer any controversy that prediabetes needs to be addressed
There are several options to consider, including FPG, repeat
and treated. Preventing diabetes is the only way of decreasing the
OGTT, HbA1c, or any combination of these tests.
immense current and future burden of diabetes and the attendant
Although FPG is convenient and can be coupled with fasting
lipid tests, FPG alone has limitations. As previously stated, FPGprovides an incomplete picture of chronic glycemic control andchange, providing poor sensitivity (ϳ40 – 60%) in detecting di-abetes (49). Postprandial hyperglycemia due to insulin resistance
Acknowledgments
and insufficient ␤-cell compensation are often more prominent
Address all correspondence and requests for reprints to: Robert
in prediabetes than fasting hyperglycemia. At lower levels of
Ratner, Med Star Clinical Research Center, 650 Pennsylvania Avenue
HbA1c (e.g. Ͻ7.3%), postprandial glucose contributes more
to the overall diurnal hyperglycemia than FPG (50).
Disclosure Statement: The authors have nothing to disclose.
The Australian guidelines in prediabetes recommend an an-
nual OGTT initially with individualized monitoring every 1–3 yrthereafter (Table 1). In addition, participants in the DPP hadannual OGTTs to detect conversion from IGT to diabetes. Al-
References
though the OGTT with repeat confirmatory testing proved its
1. American Diabetes Association 2008 Position Statement: Diagnosis and Clas-
merit in detecting new conversions to diabetes in the DPP (9),
sification of Diabetes Mellitus. Diabetes Care 31:S55–S60
escalation of therapy was based primarily on significant changes
2. World Health Organization/International Diabetes Federation 2006 Defini-
tion and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycemia:
in glycemic control as measured by elevations in FPG of at least
report of a WHO/IDF consultation. http://www.who.int/diabetes/publica-
140 mg/dl (7.8 mmol/liter) (19). Thus, used primarily to label the
tions/Definition%20and%20diagnosis%20of%20diabetes_new.pdf. Ac-
conversion to diabetes, a periodic OGTT would not provide any
3. The Expert Committee on the Diagnosis and Classification of Diabetes
additional information in the decision to escalate therapy. Mellitus 1997 Report of the expert committee on the diagnosis and clas-
The use of HbA1c as a diagnostic and monitoring test in
sification of diabetes mellitus. Diabetes Care 20:785–791
prediabetes is debated. On the one hand, HbA1c is not stan-
4. Ito C, Maeda R, Ishida S, Harada H, Inoue N, Sasaki H 2000 Importance of
OGTT for diagnosing diabetes mellitus based on prevalence and incidence of
dardized across various populations. In the DPP, for example,
retinopathy. Diabetes Res Clin Pract 49:181–186
after correcting for factors that would affect glycemia, HbA1c
5. Diabetes Prevention Program Research Group 2007 The prevalence of reti-
levels were consistently higher across ethnic minorities com-
nopathy in impaired glucose tolerance and recent-onset diabetes in the Dia-betes Prevention Program. Diabet Med 24:137–144
pared with Caucasians (51). Furthermore, HbA1c by itself lacks
6. DECODE Study Group, European Diabetes Epidemiology Group 2003 Is the
sufficient sensitivity to diagnose diabetes. However, HbA1c cor-
current definition for diabetes relevant to mortality risk from all causes and
relates well with long-term complications and is a good indicator
cardiovascular and noncardiovascular diseases? Diabetes Care 26:688 – 696
7. DECODE Study Group 1998 Will new diagnostic criteria for diabetes mellitus
of chronic glycemic control (2). In consideration of many of these
change phenotype of patients with diabetes? Reanalysis of European epide-
issues, the recent panel discussion by Saudek et al. (14) suggested
that an HbA1c at least 7%, confirmed by another test (repeat
8. Barrett-Connor E, Ferrara A 1998 Isolated postchallenge hyperglycemia and
the risk of fatal cardiovascular disease in older women and men. The Rancho
HbA1c ’Ü7%, FPG, or OGTT), would establish the diagnosis of
Bernardo Study. Diabetes Care 21:1236 –1239
diabetes and that an HbA1c of at least 6.5– 6.9% would indicate
9. Diabetes Prevention Program 2006 Repeat glucose testing to confirm glucose
diabetes with a confirmatory glucose-dependent test.
tolerance status: implications for diagnosing diabetes in high risk adults. Diabetes 55:S1 (Abstract 209)
In this patient, baseline labs included FPG, HbA1c, and OGTT.
10. Gerstein HC, Santaguida P, Raina P, Morrison KM, Balion C, Hunt D, Yazdi
Based on our discussion, one strategy for follow-up would be to
H, Booker L 2007 Annual incidence and relative risk of diabetes in people with
measure both FPG and HbA1c on a periodic basis (e.g. every 6
various categories of dysglycemia: a systematic overview and meta-analysis ofprospective studies. Diabetes Res Clin Pract 78:305–312
months) to decide whether intervention should be escalated. If FPG
11. Nathan DM, Davidson MB, DeFronzo RA, Heine RJ, Henry RR, Pratley R,
and HbA1c remain stable, no additional intervention is required. If
Zinman B 2007 Impaired fasting glucose and impaired glucose tolerance.
HbA1c increases to 7.0% or higher or if FPG increases to at least
12. Tominaga M, Eguchi H, Manaka H, Igarashi K, Kato T, Sekikawa A 1999 Im-
140 mg/dl (7.8 mmol/liter) (19), pharmacotherapy should be ad-
paired glucose tolerance is a risk factor for cardiovascular disease, but not im-
vanced to minimize long-term complications. An OGTT would
paired fasting glucose. The Funagata Diabetes Study. Diabetes Care 226:920 –924
help time the conversion to an arbitrary diagnosis of diabetes and
13. Balion CM, Raina PS, Gerstein HC, Santaguida PL, Morrison KM, Booker L, Hunt DL 2007 Reproducibility of impaired glucose tolerance (IGT) and im-
may influence treatment targets for blood pressure and lipids. The
paired fasting glucose (IFG) classification: a systematic review. Clin Chem Lab
information provided by a periodic OGTT should be weighed
against the practical issues of inconvenience, time, and need
14. Saudek CD, Herman WH, Sacks DB, Bergenstal RM, Edelman D, Davidson MB 2008 A new look at screening and diagnosing diabetes mellitus. J Clin
for a confirmatory test if abnormal.
Clearly, many of these long-debated issues remain unre-
15. Magliano D, Barr ELM, Zimmet PZ, Cameron AJ, Dunstan DW, Colagiuri S,
solved. In this article, we have offered our interpretation of the
Jolley D, Owen N, Phillips P, Tapp RJ, Welborn TA, Shaw JE 2008 Glucose indices, health behaviors, and incidence of diabetes in Australia: the Australian
existing data in an effort to guide the practitioner. The decision
Diabetes, Obesity and Lifestyle Study. Diabetes Care 31:267–272
with each patient must factor in availability of resources, patient
16. Pradhan AD, Rifai N, Buring JE, Ridker PM 2007 Hemoglobin A1c predicts
J Clin Endocrinol Metab, September 2008, 93(9):3259 –3265
diabetes but not cardiovascular disease in nondiabetic women. Am J Med
␤-cell function and prevention of type 2 diabetes by pharmacological treatment
of insulin resistance in high-risk Hispanic women. Diabetes 51:2796 –2803
17. Weyer C, Bogardus C, Mott DM, Pratley RE 1999 The natural history of
35. Xiang AH, Peters RK, Kjos SL, Marroquin A, Goico J, Ochoa C, Kawakubo
insulin secretory dysfunction and insulin resistance in the pathogenesis of type
M, Buchanan TA 2006 Effect of pioglitazone on pancreatic ␤-cell function and
2 diabetes mellitus. J Clin Invest 104:787–794
diabetes risk in Hispanic women with prior gestational diabetes. Diabetes
18. National Center for Chronic Disease Prevention and Health Promotion Dia-
betes Public Health Resource: frequently asked questions. Prediabetes. http://
36. Xiang AH, Peters RK, Kjos SL, Ochoa C, Marroquin A, Goico J, Tan S, Wang
www.cdc.gov/diabetes/faq/prediabetes.htm#6. Accessed May 15, 2008
C, Azen SP, Liu CR, Liu CH, Hodis HN, Buchanan TA 2005 Effect of thia-
19. Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker
zolidinedione treatment on progression of subclinical atherosclerosis in pre-
EA, Nathan DM; Diabetes Prevention Program Research Group 2002 Reduc-
menopausal women at high risk for type 2 diabetes. J Clin Endocrinol Metab
tion in the incidence of type 2 diabetes with lifestyle intervention or metformin.
37. Xiang AH, Hodis HN, Kawakubo M, Peters RK, Kjos SL, Marroquin A, Goico
20. Levitan EB, Song Y, Ford ES, Liu S 2004 Is nondiabetic hyperglycemia a risk J, Ochoa C, Liu CR, Liu CH, Buchanan TA 2008 Effect of pioglitazone on
factor for cardiovascular disease? A meta-analysis of prospective studies. Arch
progression of subclinical atherosclerosis in non-diabetic premenopausal His-
panic women with prior gestational diabetes. Atherosclerosis 199:207–214
21. Pan XR, Li GW, Hu YH, Wang JX, Yang WY, An ZX, Hu ZX, Lin J, Xiao JZ,
38. DREAM (Diabetes REduction Assessment with ramipril and rosiglitazone Cao HB, Liu PA, Jiang XG, Jiang YY, Wang JP, Zheng H, Zhang H, Bennett Medication) Trial Investigators, Gerstein HC, Yusuf S, Bosch J, Pogue J, PH, Howard BV 1997 Effects of diet and exercise in preventing NIDDM in Sheridan P, Dinccag N, Hanefeld M, Hoogwerf B, Laakso M, Mohan V, Shaw
people with impaired glucose tolerance. The Da Qing IGT and Diabetes Study. J, Zinman B, Holman RR 2006 Effect of rosiglitazone on the frequency of
diabetes in patients with impaired glucose tolerance or impaired fasting glu-
22. Tuomilehto J, Lindstro¨m J, Eriksson JG, Valle TT, Ha¨ma¨la¨inen H, Ilanne-
cose: a randomised controlled trial. Lancet 368:1096 –1105
Parikka P, Keina¨nen-Kiukaanniemi S, Laakso M, Louheranta A, Rastas M,
39. Holman RR, Late-breaking trials: DREAM washout period results. Pro- Salminen V, Uusitupa M; Finnish Diabetes Prevention Study Group 2001
gram and abstracts of the 19th World Diabetes Congress, Cape Town,
Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects
with impaired glucose tolerance. N Engl J Med 344:1343–1350
40. DREAM Trial Investigators, Dagenais GR, Gerstein HC, Holman R, Budaj A,
23. Kosaka K, Noda M, Kuzuya T 2005 Prevention of type 2 diabetes by lifestyle Escalante A, Hedner T, Keltai M, Lonn E, McFarlane S, McQueen M, Teo K,
intervention: a Japanese trial in IGT males. Diabetes Res Clin Pract 67:
Sheridan P, Bosch J, Pogue J, Yusuf S 2008 Effects of ramipril and rosiglitazone
on cardiovascular and renal outcomes in people with impaired glucose toler-
24. Lindstro¨m J, Ilanne-Parikka P, Peltonen M, Aunola S, Eriksson JG, Hemio¨
ance or impaired fasting glucose: results of the Diabetes REduction Assessment
K, Ha¨ma¨la¨inen H, Ha¨rko¨nen P, Keina¨nen-Kiukaanniemi S, Laakso M,
with ramipril and rosiglitazone Medication (DREAM) trial. Diabetes Care
Louheranta A, Mannelin M, Paturi M, Sundvall J, Valle TT, Uusitupa M, Tuomilehto J; Finnish Diabetes Prevention Study Group 2006 Sustained
41. Kahn SE, Zinman B, Lachin JM, Haffner SM, Herman WH, Holman RR,
reduction in the incidence of type 2 diabetes by lifestyle intervention: follow-up
Kravitz BG, Yu D, Heise MA, Aftring RP, Viberti G; Diabetes Outcome
of the Finnish Diabetes Prevention Study. Lancet 368:1673–1679
Progression Trial (ADOPT) Study Group 2008 Rosiglitazone-associated frac-
25. Diabetes Prevention Program Research Group 2003 Effects of withdrawal
tures in type 2 diabetes: an Analysis from A Diabetes Outcome Progression
from metformin on the development of diabetes in the diabetes prevention
Trial (ADOPT). Diabetes Care 31:845– 851
42. DeFronzo R, Banerji MA, Bray G, Buchanan T, Clement S, Henry R, Kitabchi
26. Ramachandran A, Snehalatha C, Mary S, Mukesh B, Bhaskar AD, Vijay V; A, Mudaliar S, Musi N, Ratner R, Reaven P, Schwenke D, Stenz F, Tripathy Indian Diabetes Prevention Programme (IDPP) 2006 The Indian Diabetes Pre- D, ACTos NOW for the Prevention of Diabetes (ACT NOW) Study. American
vention Programme shows that lifestyle modification and metformin prevent
Diabetes Association 68th Scientific Sessions, San Francisco, 2008 (Late
type 2 diabetes in Asian Indian subjects with impaired glucose tolerance (IDPP-1).
43. Eddy DM, Schlessinger L, Kahn R 2005 Clinical outcomes and cost-
27. Herman WH, Hoerger TJ, Brandle M, Hicks K, Sorensen S, Zhang P, Hamman
effectiveness of strategies for managing people at high risk for diabetes. Ann
RF, Ackermann RT, Engelgau MM, Ratner RE; Diabetes Prevention Program Research Group 2005 The cost-effectiveness of lifestyle modification or met-
44. Norris SL, Kansagara D, Bougatsos C, Fu R; U.S. Preventive Services Task
formin in preventing type 2 diabetes in adults with impaired glucose tolerance. Force 2008 Screening adults for type 2 diabetes: a review of the evidence for
the U.S. Preventive Services Task Force. Ann Intern Med 148:855– 868
28. Ratner R, Goldberg R, Haffner S, Marcovina S, Orchard T, Fowler S,
45. Indian Health Services 2006 IHS guidelines for care of adults with prediabetes Temprosa M; Diabetes Prevention Program Research Group 2005 Impact of
and/or the metabolic syndrome in clinical settings. http://www.ihs.gov/Medi-
intensive lifestyle and metformin therapy on cardiovascular disease risk factors
calPrograms/Diabetes/resources/r_index.asp. Accessed April 28, 2008
in the diabetes prevention program. Diabetes Care 28:888 – 894
46. Twigg SM, Kamp MC, Davis TM, Neylon EK, Flack JR; Australian Diabetes
29. Haffner S, Temprosa M, Crandall J, Fowler S, Goldberg R, Horton E, Society; Australian Diabetes Educators Association 2007 Prediabetes: a posi- Marcovina S, Mather K, Orchard T, Ratner R, Barrett-Connor E, Diabetes
tion statement from the Australian Diabetes Society and Australian Diabetes
Prevention Program Research Group 2005 Intensive lifestyle intervention or
Educators Association. Med J Aust 186:461– 465
metformin on inflammation and coagulation in participants with impaired
47. Nathan DM, Buse JB, Davidson MB, Heine RJ, Holman RR, Sherwin R,
glucose tolerance. Diabetes 54:1566 –1572
Zinman B 2006 Management of hyperglycemia in type 2 diabetes: a consensus
30. Li G, Zhang P, Wang J, Gregg EW, Yang W, Gong Q, Li H, Li H, Jiang Y, An
algorithm for the initiation and adjustment of therapy: a consensus statement
Y, Shuai Y, Zhang B, Zhang J, Thompson TJ, Gerzoff RB, Roglic G, Hu Y,
from the American Diabetes Association and the European Association for the
Bennett PH 2008 The long-term effect of lifestyle interventions to prevent
Study of Diabetes. Diabetes Care 29:1963–1972
diabetes in the China Da Qing Diabetes Prevention Study: a 20-year follow-up
48. Action to Control Cardiovascular Risk in Diabetes Study Group, Gerstein HC, Miller ME, Byington RP, Goff Jr DC, Bigger JT, Buse JB, Cushman WC,
31. Chiasson JL, Josse RG, Gomis R, Hanefeld M, Karasik A, Laakso M, STOP- Genuth S, Ismail-Beigi F, Grimm Jr RH, Probstfield JL, Simons-Morton DG, NIDDM Trail Research Group 2002 Acarbose for prevention of type 2 dia- Friedewald WT 2008 Effects of intensive glucose lowering in type 2 diabetes.
betes mellitus: the STOP-NIDDM randomised trial. Lancet 359:2072–2077
32. Chiasson JL, Josse RG, Gomis R, Hanefeld M, Karasik A, Laakso M, STOP-
49. Engelgau MM, Narayan KM, Herman WH 2000 Screening for type 2 diabetes. NIDDM Trial Research Group 2003 Acarbose treatment and the risk of car-
diovascular disease and hypertension in patients with impaired glucose toler-
50. Monnier L, Lapinski H, Colette C 2003 Contributions of fasting and postprandial
ance: the STOP-NIDDM trial. JAMA 290:486 – 494
plasma glucose increments to the overall diurnal hyperglycemia of type 2 diabetic
33. Hanefeld M, Chiasson JL, Koehler C, Henkel E, Schaper F, Temelkova-
patients: variations with increasing levels of A1c. Diabetes Care 26:881– 885
Kurktschiev T 2004 Acarbose slows progression of intima-media thickness of
51. Herman WH, Ma Y, Uwaifo G, Haffner S, Kahn SE, Horton ES, Lachin JM,
the carotid arteries in subjects with impaired glucose tolerance. Stroke 35:
Montez MG, Brenneman T, Barrett-Connor E; Diabetes Prevention Program Research Group 2007. Differences in A1C by race and ethnicity among pa-
34. Buchanan TA, Xiang AH, Peters RK, Kjos SL, Marroquin A, Goico J, Ochoa
tients with impaired glucose tolerance in the Diabetes Prevention Program. C, Tan S, Berkowitz K, Hodis HN, Azen SP 2002 Preservation of pancreatic
Gesundheitsdienst 10/07/GvL/GB Merkblatt f√ºr Besch√§ftigte und Reisende H√∂henkrankheit Wenn Reisen ins Hochgebirge vern√ºnftig vorbereitet werden, besteht f√ºr Gesunde nur ein geringes Risiko. Sogar gute Erholung ist m√∂glich. Touristen und Reisende im Hochgebirge gehen aber selbst aus Unwissenheit unn√∂tige Risiken ein. Hierzu z√§hlen besonders: Bergunf√§lle: ausgel√
1 treatment 1 size smal er™* LIPOSONIX® TREATMENT SETTINGS AND PEARLS PRE-TREATMENT: APPOINTMENT PLANNING AND PATIENT EXPECTATIONS • Instruct patient to wear loose fitting clothing for treatment. Consider using modesty garments to prevent soaking/staining • Discuss post-treatment expectations – specifical y that swel ing and bruising lasting as much as several weeks may occ
 J Clin Endocrinol Metab, September 2008, 93(9):3259 –3265
nese Da Qing study of more than 500 IGT subjects was one of the
25%, suggesting the possibility that metformin was not just
first to show the benefit of long-term diet and exercise intervention
masking a diagnosis of diabetes but also helped to delay the
to prevent diabetes (21). Both the Finnish Diabetes Prevention
progression of prediabetes (25). Whether metformin was really
Study and the DPP demonstrated a 58% reduction in the progres-
changing the natural history of the disease would have been
sion from IGT to diabetes with intensive lifestyle changes compared
better delineated if the washout period had been longer.
J Clin Endocrinol Metab, September 2008, 93(9):3259 –3265
nese Da Qing study of more than 500 IGT subjects was one of the
25%, suggesting the possibility that metformin was not just
first to show the benefit of long-term diet and exercise intervention
masking a diagnosis of diabetes but also helped to delay the
to prevent diabetes (21). Both the Finnish Diabetes Prevention
progression of prediabetes (25). Whether metformin was really
Study and the DPP demonstrated a 58% reduction in the progres-
changing the natural history of the disease would have been
sion from IGT to diabetes with intensive lifestyle changes compared
better delineated if the washout period had been longer.