Thank you, it's cool. Used for the first time because only then was the right drug. Very revealing detail: ordered Express shipping to get the order within 3 hours because didn't know how to get the order faster https://africarx.co.za/ The drug is authentic exactly. Consistent with the stated prices the Staff is knowledgeable.
Cls795.dvi
Clinical Science (2005) 109, 319–324 (Printed in Great Britain)
Effect of sildenafil and acclimatization on
Colin W. M. CHAN∗, Helen HOAR∗, Kyle PATTINSON†, Arthur R. BRADWELL∗, Alexander D. WRIGHT∗, Christopher H. E. IMRAY‡ and the Birmingham Medical Research Expeditionary Society∗
∗Immunodiagnostics Research Laboratory, The Medical School, University of Birmingham, Vincent Drive, Edgbaston,Birmingham B15 2TT, U.K., †Nuffield Department of Anaesthetics, University of Oxford, The John Radcliffe Hospital,Headley Way, Oxford OX3 9DU, U.K., and ‡County Vascular Unit, University Hospitals Coventry and WarwickshireNHS Trust, Clifford Bridge Road, Coventry CV2 2DX, U.K.
Phosphodiesterase-5 inhibitors decrease hypoxic pulmonary vasoconstriction under hypobarichypoxia, but are not known to affect cerebral blood flow or oxygenation. The present study wasdesigned to evaluate the effect of sildenafil on cerebral haemodynamics during acute exposureto altitude and after acclimatization. Ten subjects were studied 1 and 3 days after rapid ascent to3480 m before and for two consecutive hours after taking sildenafil (50 mg). Before acclimatization,HR (heart rate) rose at 1 h (76.3 +
P < 0.05) and had returned to baseline at 2 h (71.3 +
− 1.1 beats/min; P > 0.05). Mean BP (blood pres-
− 2.5 (P < 0.001) at 1 h and 89.8 +
(P < 0.0001) at 2 h, whereas SaO2 (arterial oxygen saturation) increased from 83.9 +
− 0.4 % (P < 0.0001) at 1 h and 85.0 +
− 0.5 % (P < 0.01) at 2 h. MCAV [MCA
(middle cerebral artery) velocity] and PETCO2 (end-tidal partial pressure of CO2) were unchanged,but rSO2 (regional cerebral oxygen saturation) rose progressively at 1 h (62.7 +
− 0.9 %; P < 0.0001) compared with baseline (59.3 +
ization, resting rSO2 and RMCA (MCA resistance) increased and oxygen delivery fell. Changes inHR and mean BP after sildenafil were similar to day 1, but SaO2 did not change. However, rSO2increased [61.7 +
− 1.0 % (P < 0.0001) at 1 h and 64.0 +
at 2h], despite a reduction in MCAV [65.3 +
− 1.7 cm/s (P < 0.0001) at 2 h] and PETCO2 [4.1 +
0.04 kPa at 2 h (P < 0.01)]. These observations suggest that sildenafil improves cerebral oxygen-ation at altitude. Whereas the early changes before acclimatization may be largely pulmonary inorigin, the later observations may be a direct cerebral effect which warrants further study. INTRODUCTION
cerebral autoregulatory responses which provide stableDo2 (oxygen delivery), particularly by increasing cerebral
Increasing numbers of people travel to or work at altitude
and risk development of AMS (acute mountain sickness)
Acute hypobaric hypoxia also affects the pulmonary
[1]. The brain is sensitive to relatively minor fluctuations
circulation resulting in pulmonary hypertension and this
in cerebral oxygenation and is normally protected by
may be associated with high-altitude pulmonary oedema. Key words: acclimatization, altitude, cerebral regional oxygen saturation, hypoxia, middle cerebral artery velocity, phos- phodiesterase-5, sildenafil (Viagra®). Abbreviations: AMS, acute mountain sickness; BP, blood pressure; Do2, oxygen delivery; HR, heart rate; MCA, middle cerebral artery; MCAV, MCA velocity; NIRS, near-IR spectroscopy; NO, nitric oxide; eNOS, endothelial NO synthase; PDE5, phosphodiesterase-5; Petco2, end-tidal partial pressure of CO2; RMCA, MCA resistance; rSo2, regional cerebral oxygen saturation; Sao2, arterial oxygen saturation. Correspondence: Dr Colin W. M. Chan (email colin.chan@mac.com).
There has been recent interest in the use of sildenafil,
was administered orally following baseline measurements
a selective PDE5 (phosphodiesterase-5) inhibitor, which
and repeat measurements made after 1 h at 150 m and at
has been shown to be effective in reducing pulmonary
1 and 2 h at 3480 m. HR (heart rate), BP (blood pressure),
hypertension. Sildenafil has variable vasodilating effects
Sao2 (arterial oxygen saturation), Petco2 (end-tidal par-
on different vascular beds attributable to the differential
tial pressure of CO2), rSo2 (regional cerebral oxygen sat-
expression of PDE5 in the endothelium of blood vessels
uration) and MCAV (MCA velocity) were recorded with
throughout the body. The presence of other synergistic
five measurements made at each time point. Subjects were
factors is postulated to play a role as well, e.g. the pres-
not taking nitrates or any other cardiovascular drugs.
ence of NO (nitric oxide) released from non-cholinergic
The side-effect profile was evaluated by direct question-
non-adrenergic penile nerve endings, which has been
ing of subjects upon completion of the experiment at
utilized in the treatment of erectile dysfunction. The pro-
3480 m. The presence of AMS was scored using the Lake
found effect of sildenafil in abolishing the rise in pul-
Louise self-completed questionnaire [7].
monary artery pressure during acute hypoxia-induced
The Research and Ethics Committee of the South
pulmonary hypertension in human and eNOS (endo-
Birmingham Health Authority granted approval for the
thelial NO synthase)-deficient mice experiments has
studies, and subjects gave written informed consent.
raised the potential therapeutic value of sildenafil and itsanalogues [2]. Furthermore, it has been suggested that
Cerebral NIRS (near-IR spectroscopy)
sildenafil might prove to be of therapeutic benefit to
In the pilot study, continuous non-invasive cerebral NIRS
travellers and indigenous populations not well adapted
was performed at 150 m using a Critikon 2020 cerebral
to altitude in the prevention of pulmonary hypertension
redox spectroscope (Johnson and Johnson Medical Ltd).
The dual detector sensor position was standardized to a
It has been assumed that PDE5 is distributed widely
point over the right fronto-parietal region with sensor
throughout the vasculature, including the cerebral vas-
margins 3 cm from the midline and 3 cm above the supra-
cular bed. Thus sildenafil induces headache and aggrav-
orbital crest taking care to avoid the sagittal sinus. A Blue-
ates migraine at sea level, suggesting a vasodilatory effect
line Tubifast bandage (Seton Healthcare Group) was used
despite no demonstrable change having been shown in
to keep the sensor in place, and maintained a standard
MCA (middle cerebral artery) diameter [4,5]. Immuno-
probe pressure. rSo2was derived from the equation:
localization studies have demonstrated PDE5 within neu-ronal tissue in rat Purkinje fibres [6], but the enzyme
rSo2 = (oxygenated haemoglobin/total haemoglobin)
has not been specifically identified within cerebral blood
vessels. To date, sildenafil has not been shown to affectcerebral perfusion. Given its potential value in reducing
In the main study at 3480 m, an Invos Adult Cerebral
altitude related pulmonary hypertension, we sought to
Oximeter (Somanetics; Somanetic Corporation) was used
evaluate the effect of sildenafil on cerebral blood flow
to measure cerebral oxygenation. Bilateral frontal probes
and oxygenation on acute ascent to high altitude and after
were positioned and kept in place using Blue-line Tubifast
Transcranial Doppler MATERIALS AND METHODS
Continuous transcranial Doppler assessment of MCAVwas measured by one of two experienced operators using
Two studies were performed. The first was a pilot experi-
a 2 MHz pulsed-wave, range-gated Doppler ultrasound
ment undertaken to assess the cerebrovascular changes at
(MultiDop T1; DWL Elektronische Systeme). The right
150 m (Birmingham, United Kingdom) produced by sil-
MCA was identified by recognition of the characteristic
denafil on six healthy male subjects (age 34–60 years). The
waveform and typical flow velocity profile, and was
aim of the main study was to evaluate the time depen-
insonated at 45–60 mm through the temporal bone
dency and acclimatization response to sildenafil and was
window. The MCA time-averaged mean velocity (MCAV;
carried out in ten healthy subjects (seven male and three
female; age 30–65 years) at 1 and 3 days after acute ascentby cable car to 3480 m (Refugio Guide del Cervino,Aosta, Italy). Barometric pressures were 99.1 kPa in
Measurement of SaO2, PETCO2, HR and BP
Birmingham, and 66.2 kPa and 66.4 kPa on days 1 and 3
Sao2 and HR were monitored using an Ohmeda Biox
respectively, at 3480 m. Five subjects were common to
3740 Pulse Oximeter. Mean BP and Petco2 were mea-
sured using a Datex-Ohmeda S/5 portable critical caremonitor. Data were logged either manually (BP, Petco2,
Study protocol
HR and Sao2) or input via a multichannel I/O port to
Subjects were rested in the supine position for 5 min prior
the hard drive of the transcranial Doppler for subsequent
to any measurements. Sildenafil (50 mg; Viagra®, Pfizer)
Time course effect of sildenafil on systemic parameters and cerebral haemodynamics on days 1 and 3 after arrival
− S.E.M., n = 10. ∗P < 0.05, ∗∗P < 0.01, ∗∗∗P < 0.001 and ∗∗∗∗P < 0.0001 compared with the pre-sildenafil value, as determined by a paired
Student t-test. ††P < 0.01 and ††††P < 0.0001 between the 1 and 2 h time points, as determined by a paired Student t-test. ‡‡‡‡P < 0.0001 comparedwith the pre-sildenafil values on day 1, as determined by an unpaired Student t-test. Estimated cerebral DO2 and RMCA
continued to fall at 2 h. Sao2 increased at 1 h and remained
(MCA resistance)
so during the second hour. Petco2 remained unchanged.
MCAV did not change significantly after sildenafil on
2 to the brain is proportional to the product of
arterial oxygen content and brain blood flow. Since the
day 1 (Figure 1B), but cerebral oxygenation improved at
haemoglobin concentration is unlikely to have altered
1 h and continued to rise at 2 h (Figure 1A). The calculated
within 3 days and the barometric pressure remained
Do2 (Figure 1C) and RMCA (Figure 1D) did not change.
virtually unchanged, an estimate of the cerebral Do
On day 3, HR rose at 1 h and then returned to the
baseline level at 2 h. Mean BP fell at 1 h and remained soat 2 h. Although Sao2 did not alter at 1 or 2 h compared
with pre-sildenafil values, there was a small fall in Petco2
at 2 h. The mean MCAV fell and cerebral oxygenation
increased. The calculated Do2 at all time points on day 3
RMCA (resistance units) = mean arterial BP/MCAV.
was reduced compared with day 1 (P < 0.01; Figure 1C).
Following sildenafil, Do2 fell at 2 h on day 3 (35.5 +
2 and RMCA were calculated for individual subjects
− 1.2 units; P < 0.05). The baseline RMCA was higher
Statistics
− 0.1 units respectively; P < 0.05), but this difference
Statistical and graphical analyses were performed using
was abolished with sildenafil at 1 and 2 h (Figure 1D).
StatView 5.01 (SAS Institute Inc.) and Deltagraph 5 (SPSS
The main side-effect noted was facial flushing in seven
Inc. and Red Rock Software) by unpaired and paired
subjects of whom five felt that this was mild and the
Student’s t tests based on the parametric distribution of
remaining two considered this moderately severe. Head-
data. Results are expressed as mean values with data
ache was noted in three subjects (two subjects had mild
− 1 S.D. P values <0.05 were
symptoms and one moderately severe but not incapacit-
ating). Three subjects experienced mild nasal congestionand two subjects noticed bloodshot eyes although
none experienced photophobia. One subject had mildindigestion and one other had mild transient postural
In the pilot study, there were no changes in HR
DISCUSSION
− 1.4%) before and 1 h after sildenafil
Sildenafil is a cGMP-specific phosphodiesterase inhibitor
that causes selective vasodilatation through a reduction of
On the first day of the main study, there was one
intracellular calcium in vascular smooth muscle. This is
subject who had a Lake Louise symptom score of 3. There
effected by inhibiting PDE5, which prevents the break-
was no recorded AMS on day 3. The responses to silden-
down of pre-existing cGMP, the second messenger in
afil on days 1 and 3 are shown in Table 1. On day 1, there
the NO pathway. The presence of raised levels of NO
was a rise in the mean HR at 1 h, which then returned to
is a prerequisite for PDE5 inhibitors such as sildenafil
the baseline level at 2 h. Mean BP was reduced at 1 h and
to work, as demonstrated by the prolongation of erectile
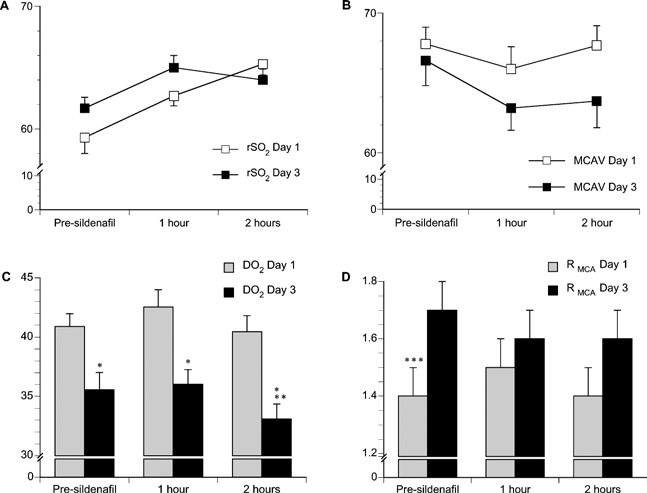
Effect of acclimatization and sildenafil on rSO2 (A), MCAV (B), DO2 (C) and RMCA (D)
− S.E.M. (single-ended error bars); n = 10. ∗P < 0.01 comparing values at day 1 and day 3 at specified time points; ∗∗P < 0.05 comparing
pre-sildenafil with the 2 h time point on day 3; and ∗∗∗P < 0.05 comparing the pre-sildenafil time point on day 1 with that at day 3. Statistical analyses on rSO2and MCAV are shown in Table 1.
function when non-cholinergic non-adrenergic (nitrox-
conditions for cerebral hypoxia and have found this
idergic) penile nerves are stimulated [8].
measure to be sensitive and reproducible as well as robust
Although the reduction in systemic BP due to the vaso-
dilatory effect of sildenafil is modest [9], there is a signi-
A comparison between the rSo2 and MCAV curves
ficant reduction in pulmonary arterial pressure in cases
in response to sildenafil for 1 day (unacclimatized) and
of pulmonary hypertension [10], presumably due to the
3 days (acclimatized) is shown in Figure 1. On day one,
background increase in NO in the pulmonary vasculature
sildenafil caused a progressive improvement in cerebral
secondary to chronic hypoxia. Thus far, sildenafil has
oxygenation at 1 and 2 h. There is a similar rise at 1 h on
not been demonstrated to have an effect on cerebral
day 3, but this effect appears to plateau at 2 h. This
blood flow by transcranial Doppler nor are there any
improvement, however, does not appear to be dependent
data on the effect of sildenafil on cerebral oxygenation as
on cerebral blood flow as there is no change in MCAV on
measured by NIRS. The effect of sildenafil on the cerebral
day 1 and, paradoxically, a reduction in MCAV on day 3.
vasculature has been postulated but not demonstrated
The calculated Do2 (Figure 1C) demonstrates the effect
previously [11]. The present study describes the effect of
of acclimatization. Do2 is proportionate to the MCAV
sildenafil on cerebral blood flow and oxygenation at sea
and the Do2 profile follows the changes in MCAV with
level and 3480 m. The absence of any change in cerebral
sildenafil. The reduction in MCAV on day 3 is likely to
oxygenation and blood flow at sea level is consistent with
be secondary to the overall improvement in Sao2 and
possibly a decrease in Petco2 with acclimatization. At
Transcranial Doppler insonation of the MCA is
high altitude, the cerebral circulation is exposed to various
accurate and reliable in the measurement of cerebral blood
competing influences: arterial hypoxaemia is a potent
flow [12] and has been shown to be robust in assessing
cerebral vasodilator, whereas arterial hypocapnia is a
cerebral haemodynamics under high-altitude conditions
potent vasoconstrictor [18]. Both these effects are reflec-
[13]. MCAV as measured by transcranial Doppler has a
ted in RMCA (Figure 1D) and are modulated by acclimat-
linear relationship with cerebral blood flow within a wide
ization. In the present study there was an increase in
range of flow values as measured by the 133Xe clearance
RMCA and a decrease in Do2 with acclimatization that
technique [12]. Furthermore, MCAV measurements
was overcome by sildenafil. On acute exposure to high
under conditions of acute hypobaric hypoxia have been
altitude, hypoxia-induced cerebral vasodilatation appears
validated against sea-level measurements and are an ac-
to override the vasoconstrictor effects of hypocapnia
curate indicator of cerebral blood flow and Do2 [14].
but, by day 3, improved peripheral oxygenation with
We have used previously cerebral NIRS under hypobaric
acclimatization increased RMCA. In the present field study,
an indirect measure of Do2 has been made by calculating
Under conditions of high-altitude hypoxia, sildenafil
the product of Sao2 and MCAV which are both non-
has a positive influence on cerebral oxygenation and an
invasive measurements. Calculated Do2 did not take into
attenuation of cerebral blood flow. However, our present
account any changes in plasma volume that may have
study was not designed to establish any therapeutic bene-
occurred at altitude, thus changes in Do2 after sildenafil
fit from improved cerebral oxygenation. The mechanism
by which these effects take place is not currently known
The different profiles in the time-course experiment
and will need to be investigated further. These findings
suggest that there may be multiple mechanisms at work
may influence our knowledge of PDE5 localization and
and the observed effects of sildenafil when acclimatized
direct further studies towards a potentially therapeutic
may be intracranial rather than systemic. It may be pos-
role for PDE5 inhibitors in the management of cerebral
tulated that the improvement in cerebral oxygenation
with sildenafil on day 1 may be due, in part, to an in-crease in Sao2. Despite the improvement in Sao2 due to
ACKNOWLEDGMENTS
acclimatization, the response to sildenafil on day 3 is notcorrelated with any change in Sao2. This suggests that the
We are grateful for the technical assistance of ScanMed
improvement in cerebral oxygenation is predominantly
Ltd, Datex-Ohmeda for the loan of the S/5 portable
intracranial. NIRS provides a measure of the proportion
critical care monitor, and to Selly Oak Hospital,
of oxygenated blood in the cerebral capillaries. It does
Birmingham, U.K. for the loan of a back-up Critikon
not distinguish how much is in the arterial or venous part
of the capillary bed. The proportion of total blood in thecerebral capillaries has been estimated at 28 % arterial
REFERENCES
and 72 % venous [19,20]. It is possible that changesin these proportions could occur both at altitude with
1 Hackett, P. H. and Roach, R. C. (2001) High-altitude
acclimatization and with sildenafil. The observed large
illness. N. Engl. J. Med. 345, 107–114
changes in cerebral NIRS with more modest changes in
2 Zhao, L., Mason, N. A., Morrell, N. W. et al. (2001)
Sildenafil inhibits hypoxia-induced pulmonary
MCAV would tend to support this model. A further
hypertension. Circulation 104, 424–428
possibility is differential vasodilatation with sildenafil (i.e.
3 Wilkins, M. R., Aldashev, A. and Morrell, N. W. (2002)
mid-sized arteries versus smaller downstream arterioles)
Nitric oxide, phosphodiesterase inhibition, and adaptation to hypoxic conditions. Lancet 359, 1539–1540
which may potentiate the observed differences in cerebral
4 Kruuse, C., Thomsen, L. L., Jacobsen, T. B. and Olesen, J.
(2002) The phosphodiesterase 5 inhibitor sildenafil has noeffect on cerebral blood flow or blood velocity, but
The presence of PDE5 in the cerebral arteries or
nevertheless induces headache in healthy subjects.
microvasculature has thus far not been demonstrated, and
J. Cereb. Blood Flow Metab. 22, 1124–1131
our present findings of a change in MCAV with PDE5
5 Kruuse, C., Thomsen, L. L., Birk, S. and Olesen, J. (2003)
Migraine can be induced by sildenafil without changes in
inhibition suggest indirectly that this enzyme may in
middle cerebral artery diameter. Brain 126, 241–247
fact be present under hypobaric hypoxia. The absence
6 Kotera, J., Fujishige, K. and Omori, K. (2000)
Immunohistochemical localisation of cGMP-binding
of a discernible change in MCAV at sea level implies
cGMP-specific phosphodiesterase (PDE5) in rat tissues.
that a hypoxic drive is a precondition to cerebrovascular
J. Histochem. Cytochem. 48, 685–693
7 Roach, R. C., Bartsch, P., Hackett, P. H. and Oelz, O.
sensitivity to sildenafil. This is the first time that PDE5
(1993) The Lake Louise acute mountain sickness scoring
inhibition has been demonstrated to affect cerebral oxy-
system. In Hypoxia and Mountain Medicine (Sutton, J. R.,
genation (both unacclimatized and acclimatized subjects)
Houston, C. S. and Coates, G., eds.), pp. 272–274, QueenCity Printers, Burlington, VT
and cerebral blood flow (acclimatized subjects). Possible
8 Cheitlin, M. D., Hutter, A. M., Brindis, R. G. et al. (1999)
explanations for the unmasking of this cerebral response
ACC/AHA Expert Consensus Document: Use ofsildenafil (Viagra) in patients with cardiovascular disease.
at altitude may be the priming effect of increased levels
Circulation 99, 168–177
of local NO within the cerebral vascular bed consequent
9 Seftel, A. (2002) Effects of sildenafil citrate (Viagra) on
upon hypobaric hypoxia, or perhaps hypoxic up-regul-
blood pressure in normotensive and hypertensive men. J. Urol. 168, 2318–2319
ation of hitherto indiscernible PDE5 at altitude. The role
10 Peacock, A. J. (2003) Treatment of pulmonary
of NO priming has yet to be explored with respect to
hypertension. Br. Med .J. 326, 835–836.
11 Arnavaz, A., Aurich, A., Weissenborn, K., Hartmann, U.,
PDE5 inhibition, but experimental evidence showing loss
Emrich, H. M. and Schneider, U. (2003) Effect of sildenafil
of protection by ischaemic preconditioning when eNOS
(Viagra®) on cerebral blood flow velocity: a pilot study.
and nNOS (neuronal NOS) knockout mice are exposed
Psychiatry Res. 122, 207–209
12 Clark, J., Skolnick, B., Gelfand, R. et al. (1996)
to focal cerebral ischaemia suggests an important role for
Relationship of 133Xe cerebral blood flow to middle
NO in the cerebrovascular response to sildenafil [21].
cerebral arterial flow velocity in men at rest. J. Cereb. Blood Flow Metab. 16, 1255–1262
Although the potential role of PDE5 inhibition in the
13 Imray, C. H., Walsh, S., Clarke, T. et al. (2003) Effects of
treatment of pulmonary hypertension has been high-
breathing air containing 3 % carbon dioxide, 35 % oxygen
lighted previously, the present study demonstrates the
or a mixture of 3 % carbon dioxide/35 % oxygen oncerebral and peripheral oxygenation at 150 m and 3459 m.
wider influence of sildenafil on the cerebral vasculature.
Clin. Sci. 104, 203–210
14 Tauboll, E., Sorteberg, W., Owe, J. O. et al. (1999) Cerebral
18 Poulin, M. J., Fatemian, M., Tansley, J. G., O’Connor,
artery blood velocity in normal subjects during acute
D. F. and Robbins, P. A. (2002) Changes in cerebral blood
decreases in barometric pressure. Aviat. Space
flow during and after 48 h of both isocapnic and
Environ. Med. 70, 692–697
poikilocapnic hypoxia in humans. Exp. Physiol. 87,
15 Imray, C. H., Barnett, N. J., Walsh, S. et al. (1998)
Near-infrared spectroscopy in the assessment of cerebral
19 McCormick, P. W., Stewart, M., Goetting, M. G. and
oxygenation at high altitude. Wilderness Environ. Med. 9,
Balakrishnan, G. (1991) Regional cerebrovascular oxygen
saturation measured by optical spectroscopy in humans.
16 Imray, C. H., Brearey, S., Clarke, T. et al. (2000) Cerebral
Stroke 22, 596–602
oxygenation at high altitude and the response to carbon
20 Wolff, C. B. and Imray, C. H. (2003) Partitioning of arterial
dioxide, hyperventilation and oxygen. Clin. Sci. 98,
and venous volumes in the brain under hypoxic conditions.
Adv. Exp. Med. Biol. 540, 19–23
17 Imray, C. H., Clarke, T., Forster, P. J. et al. (2001) Carbon
21 Atochin, D. N., Clark, J., Demchenko, I. T., Moskowitz,
dioxide contributes to the beneficial effect of
M. A. and Huang, P. L. (2003) Rapid cerebral ischemic
pressurization in a portable hyperbaric chamber at high
preconditioning in mice deficient in endothelial and
altitude. Clin. Sci. 100, 151–157
neuronal nitric oxide synthases. Stroke 34, 1299–1303
Received 26 January 2005/5 April 2005; accepted 3 May 2005Published as Immediate Publication 3 May 2005, doi:10.1042/CS20050036
Dr. Naseem Rahman d) The attitude of health workers in sterilizing a female with out partner’s consent. Often after this happens-the husband uses this excuse to re-marry. 1) Pills - Irregular, usage causes DUB and is 2) IUCD - After Insertion in multipara,IUD may be lost .Even the patient may not be aware of it- resulting pregnancy. Husband complains about painfu
Autologous blood patch in persistent air leaks after pulmonary resection Andrea Droghetti, Andrea Schiavini, Piergiorgio Muriana, Andrea Comel, GiuseppeDe Donno, Massimiliano Beccaria, Barbara Canneto, Carlo Sturani and Giovanni The online version of this article, along with updated information and services, is The Journal of Thoracic and Cardiovascular Surgery is the official publicatio
 Effect of acclimatization and sildenafil on rSO2 (A), MCAV (B), DO2 (C) and RMCA (D)
Effect of acclimatization and sildenafil on rSO2 (A), MCAV (B), DO2 (C) and RMCA (D)