Thank you, it's cool. Used for the first time because only then was the right drug. Very revealing detail: ordered Express shipping to get the order within 3 hours because didn't know how to get the order faster https://africarx.co.za/ The drug is authentic exactly. Consistent with the stated prices the Staff is knowledgeable.
Standard operating procedure
Veterinary Recommendations for Anesthesia and Analgesia
This Guidance Document is to establish recommendations for anesthesia and analgesia for use in research animals. PRINCIPLES OF ANESTHESIA AND ANALGESIA 1. The proper anesthetic and analgesic agents must be used in order to eliminate or reduce the potential for pain and distress during the peri-operative period.
2. Witholding anesthesia or analgesia must be justified and approved in the IACUC protocol. 3. A multimodal approach to analgesia should be employed to offer the best broad-spectrum pain control
possible. This includes the use of different categories of analgesics in combination to address different sources of pain perception/stimulation.
For example, a surgical procedure may use a local anesthetic block of lidocaine and bupivacaine at the
incision site, and systemic administration of an NSAID for inflammatory pain and an opioid.
4. According to the 8th edition of the Guide for the Care and Use of Laboratory Animals (NRC), “Guidelines
for the selection and proper use of analgesic and anesthetic drugs should be developed and periodically reviewed and updated as standards and techniques are refined.”
a. The inhalant anesthetics include gases such as isoflurane and sevoflurane. These anesthetics
require an anesthetic machine set-up. In addition, use of a scavenger system is required to prevent personnel exposure to the waste anesthetics. For short procedures it may be possible to administer inhalant anesthesia via a drop jar. For this procedure a cotton ball or gauze soaked with the anesthetic is placed in a jar with the animal. This procedure must be performed under a fume hood, the animal CANNOT contact anesthetic, and can only be done for minor quick procedures. Animals will recover quickly after removal from jar.
b. Advantages: safe and reliable, predictable and rapid control of anesthetic depth, not controlled
c. Disadvantages: induction must be closely monitored, personal training, special equipment
required, potential risk to staff (if not appropriately scavenged)
a. Injectable general anesthetics include ketamine/xylazine and pentobarbital. Most of the
commonly used agents are administered via intraperitoneal (IP) injection (figure 4).
b. Local anesthetics are often delivered subcutaneously along the incision site. They could also be
used in nerve blocks or epidural administration. Local anesthetics are not adequate as the only analgesic for any surgical procedure unless scientifically justified in the protocol.
Page 2 of 11
c. Advantages: They can be used without expensive supporting equipment such as the anesthesia
machines required with the use of inhalants, they are easily transported, and are relatively inexpensive.
d. Disadvantages: Prolonged recovery times. The animal will have to metabolize the drug in order to
completely recover from anesthesia. In addition, once the agent is injected, the anesthetic depth cannot be adjusted throughout the procedure except to achieve a deeper anesthetic plane by giving additional drug if the animal demonstrates signs of arousal. Animals which are sick or compromised may have a difficult time with these anesthetics due to changes in their ability to metabolize the drugs. Also, many of the commonly used injectable anesthetics are controlled substances which will require the laboratory comply with all rules regarding controlled substances and obtain a DEA license.
Monitoring Anesthetic Depth Anesthetic depth should be gauged prior to conducting any surgical manipulation and throughout the surgical procedure. Loss of reflexes (e.g., pedal, corneal, palpebral) can be used to assess appropriate anesthetic plane. There should not response to toe pinch. Signs of Inadequate anesthetic depth include purposeful movement, reflexes present, response to painful stimulus, or twitching whiskers. Equipment (e.g. pulse oximeter) may also be used to monitor depth of anesthesia. Changes in heart rate, respiratory rate, or blood pressure may indicate whether an animal is at too light or too deep of an anesthetic plane. Depth of anesthesia should be assessed every 10-15 minutes during surgery.
Assessing pain is difficult in animals. Some animals are species of prey and are adapted to hide signs of pain and distress. Clinical signs associated with pain are species specific, but some common signs of all species include changes in appearance such as hunched, scruffy, porphyrin staining (rats/mice), or changes in activity, including less active or inactive, hyperactive or pacing, abnormal postures such as back arching, belly pressing, wound guarding, or writhing. Also, decreased appetite, isolation from cage mates, exaggerated or decreased response to handling, vocalization can be used to gauge pain and distress. Recently, there has been some focus on assessing rodent facial expression or grimace scale in order to assess pain (Figure 1). It is important to pay close attention to the animal’s appearance and behavior post-surgery in order to observe subtle changes that may indicate the need for additional pain management.
Analgesia should be administered to ALL post-surgical animals unless otherwise justified in the protocol. If there is concern regarding an animal’s clinical condition post-surgery and additional analgesia is necessary, contact DLAR veterinary staff for further guidance on treating the animal.
Whenever possible multimodal analgesia is recommended. This involves providing a more ‘balanced analgesia’ through multiple methods or modalities. Local anesthetics at the incision site are often used in conjunction with a stronger opioid or NSAID analgesic.
RECOMMENDATIONS BY PROCEDURE See specific doses, routes, and frequencies in the formularies below.
1. Rodent laparotomy (example major surgery)
Page 3 of 11
Anesthesia induction via isoflurane in an induction chamber at 3-5% followed by isoflurane via facemask at 2-4%. Buprenorphine or other moderate to strong analgesic is given immediately after induction prior to patient prep to allow adequate time to reach therapeutic levels. Subsequently, moderate to strong analgesia is administered at appropriate intervals for 48 hours minimum post-operatively. Rodents are monitored closely thereafter to evaluate for signs of pain, and additional analgesia is given until evidence of pain is no longer present.
2. Rodent subcutaneous implant or vascular catheter placement (example minor surgergy)
Anesthesia induction via ketamine-xylazine. Carprofen is given immediately after induction prior to patient prep to allow adequate time to reach therapeutic levels. Carprofen is given as directed for 24 hours minimum post-operatively. Rodents are monitored closely thereafter to evaluate for signs of pain, and additional analgesia is given until evidence of pain is no longer present.
Anesthesia induction via ketamine-acepromazine. Pre-emptive analgesia is given immediately after induction prior to patient prep to allow adequate time to reach therapeutic levels; buprenorphine (for moderate pain; time to effect - 30 minutes IV & 60 minutes IM) and NSAID (time to effect - 60 minutes IV or IM). Following endotracheal intubation, anesthesia is maintained with isoflurane. Local anesthetics, lidocaine and bupivacaine, are given SC at the location of planned incision. Post-operative analgesia, buprenorphine and NSAID, is given at appropriate intervals for at least 48 hours postoperatively. Swine are monitored closely postoperatively to evaluate for signs of pain, and additional analgesia is given until evidence of pain is no longer present.
Anesthesia induction via ketamine-diazepam. Pre-emptive analgesia is given immediately after induction prior to patient prep to allow adequate time to reach therapeutic levels; buprenorphine (for severe pain; time to effect - 30 minutes IV & 60 minutes IM) and NSAID (time to effect - 60 minutes IV or IM). A fentanyl transdermal patch is secured on skin (time to effect - 12-24 hours). Following endotracheal intubation, anesthesia is maintained with isoflurane. Local anesthetics, lidocaine and bupivacaine, are given SC at the location of planned incision. Once skin incision is made, an intercostal nerve block is performed. Post-operative analgesia is given at appropriate intervals for at least 72 hours postoperatively, buprenorphine for 12-24 hours until fentanyl takes effect, fentanyl transdermal patch in place for 72 hours, and NSAID for 3-5 days. Dogs are monitored closely postoperatively to evaluate for signs of pain, and additional analgesia is given until evidence of pain is no longer present.
Page 4 of 11
FORMULARY FOR MOST COMMONLY USED SPECIES AND DRUGS
Mouse and Rat Formulary Analgesics
Not adequate as a sole analgesic except for very minor pain. May be
combined with another class of analgesic for post-op pain.
Change water every other day. Water must be placed on cage 48
hours prior to painful procedure in order for rats to acclimate.
For chronic or severe pain. Literature does not define recommended dosing interval in rodents. In other species administered up to TID. Start at BID dosing.
Anesthetics
Gold standard anesthetic. Must have appropriate equipment to use
safely (precision vaporizer and scavenging).
Ketamine combinations are the next best anesthetic if isoflurane
cannot be used. Do not re-dose xylazine; if additional dose needed
Very short term anesthesia, not recommended for survival
procedures; inappropriate storage or mixing may result in toxicity.
Reversal Agents Local anesthetics Mouse
Page 5 of 11 Dog Formulary Analgesics
Severe pain; 24 hours for maximal effect
NSAIDS/OTHER
Excellent synergistic effect with opioids
Excellent synergistic effect with opioids
Anesthetics INHALATION
Must use precision sevoflurane vaporizer
INJECTABLE
Use for anesthetic induction; duration 20-30
Use for anesthetic induction; duration 20-30
Must administer slowly over 30-60 seconds to
avoid apnea, hypotension. Rapid recovery in
Single dose duration approximately 45 minutes
Page 6 of 11 Local anesthetics
Mix in same syringe for infiltration or local nerve block.
Bupivacaine has slow onset (20-30 minutes), longer duration (4-8 hours); Lidocaine has rapid onset (5-10 minutes), shorter duration (1-2 hours).
Neuromuscular Blocking Reversal agents
Reverses neuromuscular block; give atropine
Swine Formulary3 Analgesics
Severe pain; dosage variable depending upon
breed, age, patch location, heat, moisture, procedure
Excellent synergistic effect with opioids
Excellent synergistic effect with opioids
Anesthetics INHALATION
Must use precision sevoflurane vaporizer
INJECTABLE
Use for anesthetic induction; duration 30
Page 7 of 11
Use for anesthetic induction; duration 45-60
minutes; profoundly hypothermic due to peripheral vasodilation; terminal procedures only
Use for anesthetic induction; use anticholinergic
20 minutes immobilization; use for minor
surgery & anesthetic induction; hypothermia, cardiodepression
Use for anesthetic induction and intubation; not
Must administer slowly over 30-60 seconds to
avoid apnea, hypotension. Effective sedation
Reversal agents
Reverses sedative, cardiodepression, analgesic effects of xylazine
Local anesthetics
Mix in same syringe for infiltration or local nerve block.
Bupivacaine has slow onset (20-30 minutes), longer duration (4-8 hours); Lidocaine has rapid onset (5-10 minutes), shorter duration (1-2 hours).
Neuromuscular Blocking Reversal agents
Reverses neuromuscular block; give atropine
Cat Formulary Analgesics
Page 8 of 11
Severe pain; 6-12 hours for maximal effect
Excellent synergistic effect with opioids; chronic
Anesthetics INHALATION
Must use precision sevoflurane vaporizer
INJECTABLE
Use for anesthetic induction; duration 20-30
Use for anesthetic induction; duration 20-30
Administer xylazine first as stimulation of
chemoreceptor trigger zone frequently causes vomiting; wait 10 minutes, then administer ketamine
Reversal agents
Reverses sedative, cardiodepression, analgesic effects of xylazine
Local anesthetics
Mix in same syringe for infiltration or local nerve block.
Bupivacaine has slow onset (20-30 minutes), longer duration (4-8 hours); Lidocaine has rapid onset (5-10 minutes), shorter duration (1-2 hours).
Neuromuscular Blocking Reversal agents
Reverses neuromuscular block; give atropine
Page 9 of 11 Rabbit Formulary Analgesics
Severe pain; do not cut patch, cover ½ not in
Excellent synergistic effect with opioids
Excellent synergistic effect with opioids
Anesthetics INHALATION INJECTABLE
Minor surgery only; lower doses used for
anesthetic induction when isoflurane used for
induction when isoflurane used for anesthetic maintenance
induction when isoflurane used for anesthetic
Page 10 of 11
induction when isoflurane used for anesthetic
Reversal agents
More specific for reversal of medetomidine than
Reverses sedative, cardiodepression, analgesic
Local anesthetics
Mix in same syringe for infiltration or local nerve block.
Bupivacaine has slow onset (20-30 minutes), longer duration (4-8 hours); Lidocaine has rapid onset (5-10 minutes), shorter duration (1-2 hours).
References Primary reference: Fish RE et al. Anesthesia and Analgesia in Laboratory Animals, 2nd edition, 2008. Other references: 1. Carpenter J. Exotic Animal Formulary, 4th ed, 2012. 2. (denoted by * in table) Kuehn N. North American Companion Animal Formulary, 9th ed, 2010. 3. Swindle, MM. Swine in the Laboratory: Surgery, Anesthesia, Imaging, and Experimental Techniques, 2nd Ed, 2007. 4. Langford DJ, Bailey AL, Chanda ML, Clarke SE, Drummond TE, Echols S, Glick S, Ingrao J, Klassen-Ross T, Lacroix-Fralish ML, Matsumiya
L, Sorge RE, Sotocinal SG, Tabaka JM, Wong D, van den Maagdenberg AM, Ferrari MD, Craig KD, Mogil JS. 2010. Coding of facial expressions of pain in the laboratory mouse. Nature methods 7:447-449.
Page 11 of 11 Figure 1. Mouse Grimace Scale4
COMPANY POLICY FORM IIPC offers fundamental continuing educational classes for licensed professionals in thehealth and beauty industry seeking to enhance their existing skills and knowledge. Students must complete 70 + hours of education before you s tart your hands-oneducation at IIPC. This will consist of studying , tests, Questions and Answers of:IPC educational manual “The Ultimate Guid
Dr. H. A. Nieper, M.D., Paracelsus Klinik, Hannover, Germany Translated from "Zeitschrift fur praklinische GERIATRIE" vol. 3, 4/73 THE CLINICAL EFFECT OF CALCIUM OROTATE * ON CARTILAGE TISSUE *also known as calcium diorotate A Specific function in relation to pentose metabolism of bradytrophic tissue? We are presenting here an orientation into the clinical effect of calcium orotate. Ca
 Veterinary Recommendations for Anesthesia and Analgesia
Veterinary Recommendations for Anesthesia and Analgesia 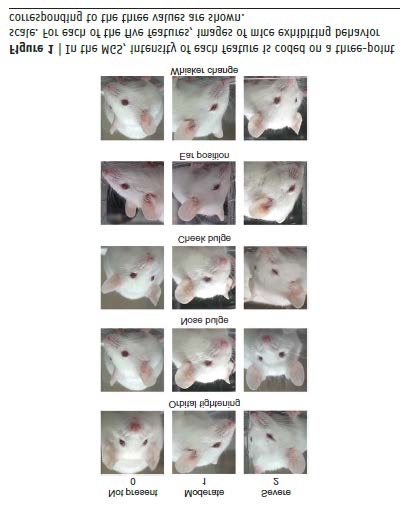 Page 11 of 11
Page 11 of 11