Ordered, immediately called back and the same day delivered the order.Very pleased with the work. Thank you for prompt and accurate work https://africarx.co.za/buy-cialis-south-africa.html great prices, delivered on the day of the order. Pleasant managers consult by phone.
Lifeshape.net
OBES SURG (2009) 19:1084–1088DOI 10.1007/s11695-009-9879-6
Improvement of Metabolic Syndrome Following IntragastricBalloon: 1 Year Follow-up Analysis
Nicola Crea & Giacomo Pata & Domenico Della Casa &Luigi Minelli & Giovanni Maifredi & Ernesto Di Betta &Francesco Mittempergher
Received: 9 March 2009 / Accepted: 7 May 2009 / Published online: 9 June 2009
# Springer Science + Business Media, LLC 2009
16.7%, and 30.4% at t0 and 21.3%, 17.4%, 18.9%, and
Objective This study aimed to assess the impact of intra-
34.8% at t12. HbA1c blood concentration shifted from an
gastric balloon (IGB)-induced body weight loss on meta-
initial value of 7.5±2.1% to 5.7±1.9% (t0), 5.6±0.7% (t6),
bolic syndrome in obese patients and evaluate what
and 5.5±0.9% (t12). Patients suffering from DM or BH
stopped or diminished relative drug consumption at t12.
Methods To this end, data were collected on 143 obese
Negligible modifications were reported as regards HDL
patients (body mass index (BMI) 36.2±5.7 kg/m²) who
underwent IGB insertion between January 2000 and
Conclusion Weight regain is commonly observed during
December 2005. Outcomes were recorded at BioEnterics
long-term follow-up after IGB removal. Nevertheless, the
Intragastric Balloon removal time (t0) and at 6-month (t6)
maintenance of at least 10% of the BWL%, as reported at
1-year follow-up, is associated with an improvement in
Results Significant BMI, excess body weight loss percent-
age, and body weight loss percentage (BWL%) wereobserved at t0 (29.6±4.6 kg/m²; 29.3±4.8%; 14.1±5.7%),
Keywords Intragastric balloon . Obesity . Metabolic
followed by partial weight regain at t12 (32.4±4.3 kg/m²;
26.1±4.9%; 11.2±4.6%). Incidence of metabolic syndromedropped from 34.8% (pre-IGB value) to 14.5% (t0) and11.6% (t12). Likewise, type 2 diabetes mellitus (DM),
hypertriglyceridemia, hypercholesterolemia, and blood hy-pertension (BH) incidence decreased from 32.6%, 37.7%,
Although intensive research has demonstrated that the
33.4%, and 44.9% (pre-IGB values) to 20.9%, 14.5%,
weight gain is often associated with a cluster of metabolicalterations such as diabetes mellitus, blood hypertension,
N. Crea (*) : G. Pata : E. Di Betta : F. Mittempergher
dyslipidemia, heart and brain vascular diseases, degenera-
Department of Medical and Surgical Sciences, General Surgery,
tive diseases of the joints, hepatic steatosis (with or without
cirrhosis), and sleep apnea –], no study has been
reported so far assessing the impact of intragastric balloon
25123 Brescia, Italye-mail: cirioz@libero.it
(IGB)-induced body weight loss on obesity-related meta-bolic syndrome in long-term follow-up.
Currently, intragastric balloons (air- or liquid-filled) are
Department of Medical and Surgical Sciences,
applied in patients with body mass index (BMI)>30 kg/m²
Surgical Endoscopy, University of Brescia,
associated with obesity-related illnesses who failed torespond to conservative management and in subjects whose
cardiocirculatory or respiratory conditions preclude any
Department of Experimental and Applied Medicine, Institute of
Hygiene, Epidemiology and Public Health, University of Brescia,
exploiting the improvement of comorbidities expected after
balloon removal and to minimize surgical and anesthetic
hypertensive patients as high as 161 ± 13.7 and 94 ±
risks [, Tolerance and efficacy in terms of body weight
12.3 mmHg, respectively. Type 2 DM was found in
loss have been the most frequently assessed aspects of this
32.6% of patients, with values of HBA1C as high as 7.5±
2.1% among the 45 DM cases. Hyperuricemia (values ≥
The aim of this study was to evaluate whether the
7 mg/dL) was reported in 26.1% of patients. Hyper-
intragastric-balloon-induced body weight loss might have
triglyceridemia, hypercholesterolemia, and low HDL cho-
an impact on the metabolic syndrome and its protagonists,
lesterol levels were present in 37.7%, 33.4%, and 31.9% of
such as diabetes mellitus, blood hypertension, and dyslipi-
the patients, respectively (Table No case of micro-
demia and to discover what the trend of these modifications
Our indications for the BIB placement were: BMI>
30 kg/m² without the criteria for a surgical treatment,superobese patients for reducing perioperative risk, and
selection of patients for a gastric restrictive surgery.
The absolute contraindications taken into consideration for
Between January 1, 2000 and December 31, 2005, 143
patient selection were voluminous hiatus hernia (>5 cm),
consecutive obese patients were admitted to our Depart-
abnormalities of the pharynx and esophagus, esophagus
ment of General Surgery for bariatric treatment by means of
varicose veins, use of anti-inflammatory or anticoagulant
IGB insertion (Bioenteric Intragastric Balloon (BIB)®
drugs, pregnancy and psychiatric disorders. We considered as
Inamed Health, Santa Barbara, CA, USA). We treated 41
relative contraindications esophagitis, ulceration, and acute
males (28.7%) and 102 females (71.3%). The mean age was
lesions of the gastric mucous membrane. The BIB was placed
36.2±9.7 years; the mean weight at admission was 98.5±
under sedation with endoscopic control and removed after an
16.3 kg and the mean BMI 36.2±5.7 kg/m². The mean
average period of 6 months with the same procedure. It was
excess weight was 39.1 ± 5.1 kg (Table Particular
filled with 500 ml of saline and the addition of 0.1% of
attention was paid to patients’ obesity-related comorbidities
methylene blue as a means of alerting patients should
(i.e., blood hypertension, type 2 diabetes mellitus, dyslipi-
unexpected premature rupture of the balloon occur. Patients
demia, and hyperuricemia), which were recorded at the first
followed a fluid diet from the second day after procedure, with
a regular diet (1,200-kcal/day diet) gradually introduced after
Before balloon insertion (IGB0), 34.8% of patients
1 week. Proton pump inhibitor (esomeprazole 40 mg daily)
showed the cluster of metabolic alterations known as
was given for the entire treatment period to prevent gastric
metabolic syndrome. The diagnosis of metabolic syndrome
was made according to WHO criteria [(BMI≥30 kg/
All patients were closely followed for 12 months after
m², waist to hip circumference ratio >0.90 in men and
balloon removal with a standardized follow-up protocol.
>0.85 in women, fasting blood glucose≥110 mg/dL, overt
The blood glucose and HbA1c values, triglycerides, total
diabetes mellitus (DM), triglycerides≥150 mg/dL, high-
cholesterol, HDL cholesterol, uric acid, and the blood
density lipoprotein (HDL)-cholesterol <40 mg/dL in men
pressure were evaluated for each patient at BIB removal
and <50 mg/dL in women, arterial blood pressure≥140/
time (t0) and then after 6 months (t6) and 12 months (t12)
90 mmHg, and presence of microalbuminuria). Patients
during routine follow-up investigations. The body weight
should have at least three of these criteria to be diagnosed
loss percentage (BWL%), BMI reduction, and excess of
body weight loss percentage (EWL%) were recorded.
The incidence of hypertension was 44.9%, with the
Statistical analysis was performed with software for
values of systolic and diastolic blood pressure in 62
biomedical research (McCalc® Software for Window;version 9.2.0.0). The paired-samples t test was used toanalyze differences in continuous data (presented as mean ±
Table 1 Body weight changes in terms of BMI (body mass index),
standard deviation) between two groups of patients (before
EWL% (excess weight loss percentage), and BWL% (body weight
and after treatment), while the chi-squared test was used for
loss percentage) at balloon removal time (T0) and during follow-up (t6:6 months;
was considered as statistically significant.
In two (1.4%) patients, BIB removal was performed just a
Values are expressed as mean±standard deviation.
few days after its insertion due to persistent vomiting
Table 2 Metabolic modifications following intragastric balloon treatment: outcomes at removal time (t0), 6-month follow-up (t6), and 1-yearfollow-up (t12)
IGB0 before intragastric balloon positioning, DM diabetes mellitus
despite antiemetic drugs. We observed two cases of balloon
(difference = 18 mmHg; 95% CI = 13–23; p<0.001 for
migration and one case of rupture, which required prema-
systolic; difference =19 mmHg; 95% CI=14.7–23.3; p<
ture balloon extraction. In the 138 remaining patients, the 1-
0.001 for diastolic blood pressure, respectively). Likewise
year follow-up after balloon removal was completed and
with results reported by DM patients, all subjects who
they were therefore eligible for the study. A significant BMI
failed to reach a normalization of blood pressure values at t0
reduction was achieved at BIB removal time 29.6±4.6 kg/
(42 cases) did improve their pressure condition, thereby
m² (difference=6.6; 95% confidence interval (CI)=5.37–
reducing their need for antihypertensive drugs. The meta-
7.83; p<0.001). Likewise, we observed a BWL% as high as
bolic modifications which we recorded at t6 and t12 were
14.1±5.7%, with an EWL% as high as 29.3±4.8% (p<
similar to the results observed at t0, while they significantly
0.001). Compared with values recorded at t0, patients’ BMI
improved when compared with those observed at IGB0
showed a significant gain 6 and 12 months after balloon
(Figs. and ). Blood hypertension, hypertriglyceridemia,
extraction 31.1±3.7 and 32.4±4.3 kg/m2, respectively (p=
and hypercholesterolemia were present, respectively, in
0.0031 and <0.001), although this remained significantly
32.6%, 15.2%, and 16.7% of cases at t6 (p=0.79; 0.99
lower than the BMI recorded at IGB0 (p<0.0001). The
and 1, respectively), which did not differ much from values
EWL% measured at the same time intervals displayed a
observed at t12 (34.8%, 17.4%, and 18.9%, respectively; p=
similar trend: 27.4±4.7% and 26.1±4.9%, respectively (p=
0.79, 0.74, and 0.75, respectively). Patients who were
0.001 and <0.001 when compared with values at T0;
classified as hypertensive at IGB0 reported systolic and
Fig. ). At IGB removal time (after a mean treatment
diastolic blood pressure values as high as 138 ± 15.3 and
period of 178±21 days), metabolic syndrome incidence had
73 ± 12.6 mmHg, respectively, at t6 and 142±13.1 and 72±
dropped to 14.5% (difference=20.3%; 95% CI=10.42–
11.4 mmHg, respectively, at t12 (difference=4 mmHg;
30.18; p<0.001); the incidence of DM had been reduced to20.9% (difference=11.7%; 95% CI=1.35–22.05; p=0.039),while there was a decrease in insulin or metforminrequirement in the remaining diabetic patients (Table ). Among DM patients, the mean HbA1c improved signifi-cantly compared with baseline values (5.7±1.9%; differ-ence=1.8%; 95% CI 0.96–2.64; p=0.0001; Fig. ). As fortotal cholesterol and triglyceride levels, only 16.7% and14.5% of patients continued suffering from such metabolicalterations at t0 (p=0.0022 and <0.0001, respectively). Nosignificant change was observed in HDL levels afterballoon removal nor in uric acid blood concentration. Theincidence of blood hypertension dropped to 30.4% aftertreatment (difference =14.5%; 95% CI=3.2–25.8; p=0.018;Fig. The systolic and diastolic blood pressure of
Fig. 1 Body weight changes in terms of body mass index (BMI, kg/m²), excess weight loss percentage (EWL%), and body weight loss
hypertensive patients decreased to 143±14.4 and 75±
percentage (BWL%) at balloon removal time (T0) and during follow-
11.7 mmHg, respectively, after 6 months of IGB treatment
Fig. 2 Metabolic modificationsfollowing intragastric-balloon-induced body weight loss:outcomes are expressed asincidence (%) at balloonremoval time (T0), 6-monthfollow-up (T6), 1-year follow-up(T12). IGB0=before intragastricballoon positioning;DM=diabetes mellitus;Hypert=blood hypertension;Hypercol=hypercholesterol-emia; Hypertr=hypertriglyceri-demia; Met Syndr=metabolicsyndrome
95% CI = −1.06–9.06; p=0.12 for systolic; difference=
1 mmHg; 95% CI = −3.05–5.05; p=0.626 for diastolicblood pressure). The incidence of DM was 22.5% at t6 and
Obese patients show a higher risk of mortality []. In
21.3% at t12 (p=0.86 and 0.92, respectively, as compared
the long term, more than 95% of obese patients who are
with t0). Also, blood concentration of HbA1c in patients
submitted to conventional treatments (diet therapy, in-
presenting DM at IGB0 displayed further reduction,
creased physical activity, behavior change, and drug
although not statistically significant 5.6 ± 0.7% at t6 (p=
therapy) undergo the “rubber effect,” which means that
0.67) and 5.5 ± 0.9% at t12 (p=0.422). No significant
they cannot maintain the optimal weight and drop back to
change was observed in HDL levels at T6 and T12, nor in
the previous weight –Treatment for obesity should
uricemia. We observed an average BWL% as high as 11.2 ±
aim for the improvement and well-being of patients as well
4.6% at the end of follow-up. At t6 and t12, the overall
as the metabolic health of the individual, decreasing the risk
incidence of the metabolic syndrome continued to be
of future diseases. With the failure of conservative treat-
inferior to values measured prior to the treatment, showing
ments in producing permanent weight loss, other
further improvement (although scarcely significant) when
approaches have to be considered, such as bariatric surgery.
compared with data recorded at balloon removal time
The intragastric balloon is the mildest nonmedical treatment
(13% and 11.6%, respectively; p=0.85 and 0.59).
of obese patients and it should be usefully included in thetherapeutic strategies of the obesity surgeon.
Several studies have evaluated the efficacy of the IGB
placement in terms of weight loss at 6 months or, atmost, 12 months of follow-up. Most of them concludedthat this procedure cannot be considered as the onlytreatment for the disease because the results obtainedneed to be consolidated by a definitive surgical procedure,
Herve and Mathus-Vliegen [evaluated the weight
regain 1 year after IGB removal and reported that theirpatients regained 41% and 28%, respectively, of the weightloss. Furthermore, Herve reported that only 56% of patientshad ≥20% excess weight loss after 1 year, as compared with74% at removal time; Mathus-Vliegen detailed that thepercentage of patients with a weight loss ≥10% decreasedfrom 75% at the BIB removal to 47% after 1 year.
Fig. 3 Trend of HbA1c blood concentration (mean ±95% confidence
Beside the weight loss, only a few studies have been
interval CI) following intragastric balloon-induced body weight loss:
performed so far to assess the effect of the BIB positioning
outcomes are evaluated at balloon removal time (T0), 6-month follow-
on obesity related comorbidities. A large retrospective
up (T6), 1-year follow-up (T12). IGB0=before intragastric balloonpositioning
study by the Italian group for Lap-Band has shown that
the weight loss induced by the BIB, though modest, caused
3. Doldi SB, Micheletto G, Perrini MN, et al. Treatment of morbid
obesity with intragastric balloon in association with diet. Obes
most comorbidities associated with obesity to be either
resolved or improved, in particular respiratory disorders,
4. De Waele B, Reynaert H, Urbain D, et al. Intragastric balloons for
hypertension, type 2 diabetes, and osteoarthropathy ].
preoperative weight reduction. Obes Surg. 2000;10:58–60.
They reported a resolution of comorbidities in 44.3% of
5. Wahlen CH, Bastens B, Herve J, et al. The BioEnterics Intra-
gastric Balloon (BIB): how to use it. Obes Surg. 2001;11:524–7.
subjects at the end of the treatment and an improvement of
6. Spyropoulos C, Katsakoulis E, Mead N, et al. Intragastric balloon
comorbidities with reduced pharmacological dosage in
for high-risk super-obese patients: a prospective analysis of
44.8% of cases, while no change was observed in 10.9%
efficacy. Surg Obes Relat Dis. 2007;3:78–83.
of patients. Similar conclusions have been drawn by Mui
7. Sallet JA, Marchesini JB, Pavia DS, et al. Brazilian multi center
study of intragastric balloon. Obes Surg. 2004;14:991–8.
8. Imaz I, Martinez-Cervell C, Garcia-Alvarez EE, et al. Safety and
No study is actually available assessing the long-term
effectiveness of the intragastric balloon for obesity. A meta-
evolutions (at 1 year or more) of metabolic syndrome
analysis. Obes Surg. 2008;18:841–6.
following intragastric-balloon-induced body weight loss.
9. Mittempergher F, Di Betta E, Pata G, et al. The obstructive sleep
apnea in bariatric surgery. Ann Ital Chir. 2008;79:165–70.
This lack prompted us to estimate what happens to our
10. Alberti KG, Zimmet PZ. Definition, diagnosis and classification
obese patients in a long-term follow-up protocol. We
of diabetes mellitus and its complications. Part 1: diagnosis and
observed an average body weight loss as high as 14.1±
classification of diabetes mellitus provisional report of a WHO
5.7% at BIB removal time and a partial weight regain at
consultation. Diabet Med. 1998;15:539–53.
11. Strazzullo P, Barbato A, Siani A, et al. Diagnostic criteria for
1-year follow-up (average weight loss > 10%). Such
metabolic syndrome: a comparative analysis in an unselected
maintenance of the body weight loss, although partial,
sample of adult male population. Metabolism. 2008;57:355–61.
proved sufficient in preserving the benefits obtained for
12. Pischon T, Boeing H, Hoffmann K, et al. General and abdominal
obesity-related comorbidities at the end of the treatment
adiposity and risk of death in Europe. N Engl J Med. 2008;359:2105–20.
(t0). HDL cholesterol and uric acid blood concentration
13. Ammar KA, Redfield MM, Mahoney DW, et al. Central obesity:
have been the only parameters which remain largely
association with left ventricular dysfunction and mortality in the
unchanged in our patients, while the incidence of metabolic
community. Am Heart J. 2008;156:975–81.
syndrome, blood hypertension, hypertriglyceridemia, type 2
14. Shimabukuro M. Cardiac adiposity and global cardiometabolic
risk: new concept and clinical intervention. Circ J. 2008;73:27–34.
DM, and hypercholesterolemia have been clearly demon-
15. Artham SM, Lavie CJ, Patel HM. Impact of obesity on the risk of
strated as diminishing at both 6 months and 1 year
heart failure and its prognosis. J Cardiometab Syndr. 2008;3:155–61.
16. Franz MJ, VanWormer JJ, Crain AL, et al. Weight-loss outcomes:
The crucial role of such a cutoff (10%) of body weight
a systematic review and meta-analysis of weight-loss clinical trialswith a minimum 1-year follow-up. J Am Diet Assoc.
loss percentage has been previously highlighted by Deitel
and colleagues ]. Likewise, Imaz et al. reported that
17. Avenell A, Brown TJ, McGee MA, et al. What interventions
the loss of 10% of the weight is sufficient to improve
should we add to weight reducing diets in adults with obesity? A
certain morbid conditions associated with obesity (blood
systematic review of randomized controlled trials of adding drugtherapy, exercise, behaviour therapy or combinations of these
hypertension, diabetes, hyperlipidemia) and also to reduce
interventions. J Hum Nutr Diet. 2004;17:293–316.
18. Curioni CC, Lourenço PM. Long-term weight loss after diet and
In conclusion, our data documented that the intragastric
exercise: a systematic review. Int J Obes (Lond). 2005;29:1168–74.
balloon is an effective device for obtaining a body weight
19. Herve J, Wahlen H, Schaeken A, et al. What becomes of patients
one year after the intragastric balloon has been removed? Obes
loss, but long-term results are poor since weight regain is
usually expected. Nevertheless, the maintenance of at least
20. Angrisani L, Lorenzo M, Borrelli V, et al. Is bariatric surgery
10% of body weight loss, as reported at 1-year follow-up,
necessary after intragastric balloon treatment? Obes Surg.
proved sufficient in improving or resolving many obesity-
21. Mathus-Vliegen EM, Tytgat GN. Intragastric balloon for
related comorbidities responsible for the higher cardiovas-
treatment-resistant obesity: safety, tolerance, and efficacy of 1-
cular risk in this category of patients.
year balloon treatment followed by a 1-year balloon free follow-up. Gastrointest Endosc. 2005;61:19–27.
22. Genco A, Bruni T, Doldi SB, et al. BioEnterics intragastric
Balloon: the Italian Experience with 2.515 patients. Obes Surg.
23. Mui WL, Ng EK, Tsung BY et al. Impact on obesity-related
1. Loffredo A, Cappuccio M, De Luca M, et al. Three years
illnesses and quality of life following intragastric balloon. Obes
experience with the new intragastric balloon, and a preoperative
test for success with restrictive surgery. Obes Surg. 2001;11:330–
24. Ricci G, Bersani G, Rossi A, et al. Bariatric therapy with
intragastric balloon improves liver dysfunction and insulin
2. Roman S, Napoleon B, Mion F, et al. Intragastric balloon for
resistance in obese patients. Obes Surg. 2008;18:1438–42.
“non-morbid” obesity: a retrospective evaluation of tolerance and
25. Deitel M. How much weight loss is sufficient to overcome major
efficacy. Obes Surg. 2004;14:539–44.
co-morbidities? Obes Surg. 2001;11:659.
LEY N° 868 DE DIBUJOS Y MODELOS INDUSTRIALES EL CONGRESO DE LA NACION PARAGUAYA SANCIONA CON FUERZA CAPITULO I DE LOS DIBUJOS Y MODELOS INDUSTRIALES Art. 1° Se considera dibujo industrial toda combinación de líneas y colores; y modelo industrial toda forma plástica de líneas y colores, destinados a dar una apariencia especial a un producto industrial artesanal y que s
Southend Gastroenterology Associates, PLLC Sanjay Jain, MD Colonoscopy 4402 Churchman Ave, Suite 408, Louisville, KY 40215 Colyte Preparation Instructions Please follow the following instructions one day prior to examination. 1. Prepare the colon prep by filling the gallon jug to the fill line with tap water, shake well, and set on the counter. Do not refrigerate. 2. That mornin
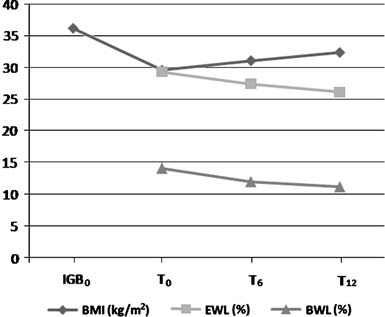 Table 2 Metabolic modifications following intragastric balloon treatment: outcomes at removal time (t0), 6-month follow-up (t6), and 1-yearfollow-up (t12)
IGB0 before intragastric balloon positioning, DM diabetes mellitus
despite antiemetic drugs. We observed two cases of balloon
(difference = 18 mmHg; 95% CI = 13–23; p<0.001 for
migration and one case of rupture, which required prema-
systolic; difference =19 mmHg; 95% CI=14.7–23.3; p<
ture balloon extraction. In the 138 remaining patients, the 1-
0.001 for diastolic blood pressure, respectively). Likewise
year follow-up after balloon removal was completed and
with results reported by DM patients, all subjects who
they were therefore eligible for the study. A significant BMI
failed to reach a normalization of blood pressure values at t0
reduction was achieved at BIB removal time 29.6±4.6 kg/
(42 cases) did improve their pressure condition, thereby
m² (difference=6.6; 95% confidence interval (CI)=5.37–
reducing their need for antihypertensive drugs. The meta-
7.83; p<0.001). Likewise, we observed a BWL% as high as
bolic modifications which we recorded at t6 and t12 were
14.1±5.7%, with an EWL% as high as 29.3±4.8% (p<
similar to the results observed at t0, while they significantly
0.001). Compared with values recorded at t0, patients’ BMI
improved when compared with those observed at IGB0
showed a significant gain 6 and 12 months after balloon
(Figs. and ). Blood hypertension, hypertriglyceridemia,
extraction 31.1±3.7 and 32.4±4.3 kg/m2, respectively (p=
and hypercholesterolemia were present, respectively, in
0.0031 and <0.001), although this remained significantly
32.6%, 15.2%, and 16.7% of cases at t6 (p=0.79; 0.99
lower than the BMI recorded at IGB0 (p<0.0001). The
and 1, respectively), which did not differ much from values
EWL% measured at the same time intervals displayed a
observed at t12 (34.8%, 17.4%, and 18.9%, respectively; p=
similar trend: 27.4±4.7% and 26.1±4.9%, respectively (p=
0.79, 0.74, and 0.75, respectively). Patients who were
0.001 and <0.001 when compared with values at T0;
classified as hypertensive at IGB0 reported systolic and
Fig. ). At IGB removal time (after a mean treatment
diastolic blood pressure values as high as 138 ± 15.3 and
period of 178±21 days), metabolic syndrome incidence had
73 ± 12.6 mmHg, respectively, at t6 and 142±13.1 and 72±
dropped to 14.5% (difference=20.3%; 95% CI=10.42–
11.4 mmHg, respectively, at t12 (difference=4 mmHg;
30.18; p<0.001); the incidence of DM had been reduced to20.9% (difference=11.7%; 95% CI=1.35–22.05; p=0.039),while there was a decrease in insulin or metforminrequirement in the remaining diabetic patients (Table ).
Table 2 Metabolic modifications following intragastric balloon treatment: outcomes at removal time (t0), 6-month follow-up (t6), and 1-yearfollow-up (t12)
IGB0 before intragastric balloon positioning, DM diabetes mellitus
despite antiemetic drugs. We observed two cases of balloon
(difference = 18 mmHg; 95% CI = 13–23; p<0.001 for
migration and one case of rupture, which required prema-
systolic; difference =19 mmHg; 95% CI=14.7–23.3; p<
ture balloon extraction. In the 138 remaining patients, the 1-
0.001 for diastolic blood pressure, respectively). Likewise
year follow-up after balloon removal was completed and
with results reported by DM patients, all subjects who
they were therefore eligible for the study. A significant BMI
failed to reach a normalization of blood pressure values at t0
reduction was achieved at BIB removal time 29.6±4.6 kg/
(42 cases) did improve their pressure condition, thereby
m² (difference=6.6; 95% confidence interval (CI)=5.37–
reducing their need for antihypertensive drugs. The meta-
7.83; p<0.001). Likewise, we observed a BWL% as high as
bolic modifications which we recorded at t6 and t12 were
14.1±5.7%, with an EWL% as high as 29.3±4.8% (p<
similar to the results observed at t0, while they significantly
0.001). Compared with values recorded at t0, patients’ BMI
improved when compared with those observed at IGB0
showed a significant gain 6 and 12 months after balloon
(Figs. and ). Blood hypertension, hypertriglyceridemia,
extraction 31.1±3.7 and 32.4±4.3 kg/m2, respectively (p=
and hypercholesterolemia were present, respectively, in
0.0031 and <0.001), although this remained significantly
32.6%, 15.2%, and 16.7% of cases at t6 (p=0.79; 0.99
lower than the BMI recorded at IGB0 (p<0.0001). The
and 1, respectively), which did not differ much from values
EWL% measured at the same time intervals displayed a
observed at t12 (34.8%, 17.4%, and 18.9%, respectively; p=
similar trend: 27.4±4.7% and 26.1±4.9%, respectively (p=
0.79, 0.74, and 0.75, respectively). Patients who were
0.001 and <0.001 when compared with values at T0;
classified as hypertensive at IGB0 reported systolic and
Fig. ). At IGB removal time (after a mean treatment
diastolic blood pressure values as high as 138 ± 15.3 and
period of 178±21 days), metabolic syndrome incidence had
73 ± 12.6 mmHg, respectively, at t6 and 142±13.1 and 72±
dropped to 14.5% (difference=20.3%; 95% CI=10.42–
11.4 mmHg, respectively, at t12 (difference=4 mmHg;
30.18; p<0.001); the incidence of DM had been reduced to20.9% (difference=11.7%; 95% CI=1.35–22.05; p=0.039),while there was a decrease in insulin or metforminrequirement in the remaining diabetic patients (Table ).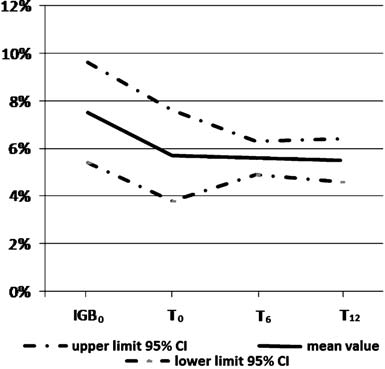
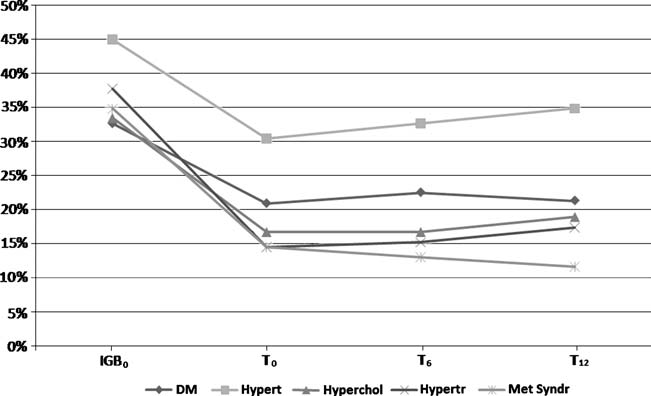 Fig. 2 Metabolic modificationsfollowing intragastric-balloon-induced body weight loss:outcomes are expressed asincidence (%) at balloonremoval time (T0), 6-monthfollow-up (T6), 1-year follow-up(T12). IGB0=before intragastricballoon positioning;DM=diabetes mellitus;Hypert=blood hypertension;Hypercol=hypercholesterol-emia; Hypertr=hypertriglyceri-demia; Met Syndr=metabolicsyndrome
95% CI = −1.06–9.06; p=0.12 for systolic; difference=
1 mmHg; 95% CI = −3.05–5.05; p=0.626 for diastolicblood pressure). The incidence of DM was 22.5% at t6 and
Obese patients show a higher risk of mortality []. In
21.3% at t12 (p=0.86 and 0.92, respectively, as compared
the long term, more than 95% of obese patients who are
with t0). Also, blood concentration of HbA1c in patients
submitted to conventional treatments (diet therapy, in-
presenting DM at IGB0 displayed further reduction,
creased physical activity, behavior change, and drug
although not statistically significant 5.6 ± 0.7% at t6 (p=
therapy) undergo the “rubber effect,” which means that
0.67) and 5.5 ± 0.9% at t12 (p=0.422). No significant
they cannot maintain the optimal weight and drop back to
change was observed in HDL levels at T6 and T12, nor in
the previous weight –Treatment for obesity should
uricemia. We observed an average BWL% as high as 11.2 ±
aim for the improvement and well-being of patients as well
4.6% at the end of follow-up. At t6 and t12, the overall
as the metabolic health of the individual, decreasing the risk
incidence of the metabolic syndrome continued to be
of future diseases. With the failure of conservative treat-
inferior to values measured prior to the treatment, showing
ments in producing permanent weight loss, other
further improvement (although scarcely significant) when
approaches have to be considered, such as bariatric surgery.
Fig. 2 Metabolic modificationsfollowing intragastric-balloon-induced body weight loss:outcomes are expressed asincidence (%) at balloonremoval time (T0), 6-monthfollow-up (T6), 1-year follow-up(T12). IGB0=before intragastricballoon positioning;DM=diabetes mellitus;Hypert=blood hypertension;Hypercol=hypercholesterol-emia; Hypertr=hypertriglyceri-demia; Met Syndr=metabolicsyndrome
95% CI = −1.06–9.06; p=0.12 for systolic; difference=
1 mmHg; 95% CI = −3.05–5.05; p=0.626 for diastolicblood pressure). The incidence of DM was 22.5% at t6 and
Obese patients show a higher risk of mortality []. In
21.3% at t12 (p=0.86 and 0.92, respectively, as compared
the long term, more than 95% of obese patients who are
with t0). Also, blood concentration of HbA1c in patients
submitted to conventional treatments (diet therapy, in-
presenting DM at IGB0 displayed further reduction,
creased physical activity, behavior change, and drug
although not statistically significant 5.6 ± 0.7% at t6 (p=
therapy) undergo the “rubber effect,” which means that
0.67) and 5.5 ± 0.9% at t12 (p=0.422). No significant
they cannot maintain the optimal weight and drop back to
change was observed in HDL levels at T6 and T12, nor in
the previous weight –Treatment for obesity should
uricemia. We observed an average BWL% as high as 11.2 ±
aim for the improvement and well-being of patients as well
4.6% at the end of follow-up. At t6 and t12, the overall
as the metabolic health of the individual, decreasing the risk
incidence of the metabolic syndrome continued to be
of future diseases. With the failure of conservative treat-
inferior to values measured prior to the treatment, showing
ments in producing permanent weight loss, other
further improvement (although scarcely significant) when
approaches have to be considered, such as bariatric surgery.