Thank you, it's cool. Used for the first time because only then was the right drug. Very revealing detail: ordered Express shipping to get the order within 3 hours because didn't know how to get the order faster https://africarx.co.za/ The drug is authentic exactly. Consistent with the stated prices the Staff is knowledgeable.
HAVING A LAPAROSCOPIC RADICAL PROSTATECTOMY What is the prostate?
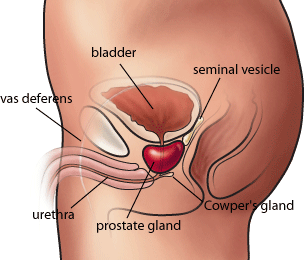
The prostate is one of the male sex glands. The prostate adds nutrients and fluid to the sperm. During ejaculation, the prostate secretes fluid that is part of the semen.
The prostate is about the size of a walnut and lies just below the urinary bladder and surrounds the upper part of the urethra. The urethra is the tube that carries urine from the bladder and semen from the sex glands out through the penis.
What is cancer?
Our bodies are made up of cells; each cell can divide to make two new cells. Sometimes the process of cell division goes wrong and the cell continues to divide in an uncontrolled way, causing a cancer to develop.
You have recently been diagnosed with cancer in the prostate, and an operation called a radical Retropubic prostatectomy has been recommended. This means that your prostate will be removed, in order to try and cure you of your cancer.
What is a laparoscopic radical prostatectomy?
Radical prostatectomy means removing the entire prostate gland. Laparoscopic refers to the surgical approach by which this is performed – through 5 tiny keyhole incisions in the lower abdomen.
Keyhole surgery for prostate cancer is now replacing open surgery. The advantages of keyhole surgery include less blood loss, less pain after the operation, and a quicker return to normal day to day activities. The only disadvantages are that it takes longer to perform, and is technically demanding.
The operation also removes the seminal vesicles. Every attempt will be made to preserve the nerves that run next to the prostate which help to produce erections. However, these may have to be sacrificed in order to remove all the prostate cancer.
Your surgeon may also elect to remove the lymph glands draining the prostate – this will be discussed this with you before the operation.
What are the benefits of having a laparoscopic radical prostatectomy?
If left alone prostate cancer can grow and invade surrounding structures e.g. bowel and bladder, or even spread to other parts of the body e.g. lymph glands and bones. The operation aims to remove all of the cancer.
What are the risks, consequences and alternatives associated with having a radical retropubic prostatectomy?
Most operations are straightforward; however as with any major surgical procedure there is a chance of side effects or complications. If you are concerned about any of these risks, or have further queries, please speak with your surgeon directly about them.
• Temporary insertion of a bladder catheter and a wound drain
• High risk of impotence due to unavoidable nerve damage
• Dry orgasm with no seminal fluid produced causing infertility
• Urinary incontinence, temporary or permanent, requiring pads or further surgery
• Discovery that cancer cells already outside the prostate, needing observation or
further treatment including radiotherapy or hormonal therapy.
• Conversion to an open procedure, as removal of the prostate not possible via keyhole
• Blood loss requiring transfusion or repeat surgery
• Anaesthetic or cardiovascular problems possibly requiring intensive care admission
(including chest infection, pulmonary embolus, stroke, deep vein thrombosis, heart attack and death)
• Rectal injury, very rarely needing temporary colostomy
Alternatives to laparoscopic radical prostatectomy
• Watchful waiting – monitoring the PSA level
• High Intensity Focussed Ultrasound (HIFU)
• Radiotherapy – giving radiation treatment to the prostate
• Brachytherapy – the implantation of radioactive seeds into the prostate
• Perineal or open removal of the prostate
Getting ready for the operation
If you smoke, try and cut down or preferably stop, as this reduces the risks of heart and chest complications during and after the operation. If you do not exercise regularly, try and do so for at least half an hour per day e.g. brisk walk or swimming.
You will be sent an appointment to see the continence nurse specialist. She will discuss pelvic floor exercises with you. These are important in speeding up your return to full continence after the operation.
You will be sent an appointment to visit the pre-assessment clinic a few days before your operation date. This is a general health check to ensure you are fit for surgery. The pre assessment nurse will organise for you to have bloods taken and have an ECG (heart tracing), and answer any questions that you may have.
You will meet the anaesthetist and discuss your anaesthetic and pain relief.
Before the operation you will be asked to sign a consent form. It is important that you read the consent form before signing. It is also important that you be aware of any potential side effects of the operation before you sign the consent form.
The day before your admission you can eat and drink as normal. You should not eat or drink anything after midnight on the night / morning before your operation.
You will be admitted on the morning of your operation. As soon as you are admitted, you will be given an enema that helps to clear the rectum and prevent rectal injury during the operation.
Precautions will be taken to stop you developing a blood clot; you will be asked to wear elasticated support stockings and will be given injections of blood thinning drugs after your operation.
The morning of your operation you should have a bath or a shower. You will be given a theatre gown to wear before you go down to theatre. A nurse or porter will take you to the operating theatre reception, your details will be checked and you will go through to the anaesthetic room.
What sort of anaesthetic will I have?
The anaesthetist will visit you before the operation to discuss this with you. This operation is performed under a general anaesthetic. This means that you will be fully asleep during the operation.
What should I expect after the operation?
After your operation you will normally go back to the male urology ward. Occasionally patients go to the High Dependency Unit for 24 hours where the doctors and nurses can monitor you more closely. The purpose of your stay here is to monitor your blood pressure, heart rate and fluid levels using accurate equipment. You will be given oxygen through a mask or nasal tube; this is to aid your recovery.
The physiotherapist will visit you and discuss your progress after the operation including breathing and leg exercises, walking and stairs.
Pain from this operation can be easily controlled. Different methods of pain control are available, and include epidural analgesia and patient controlled analgesia. Your anaesthetist will explain the advantages and disadvantages of these to you. There is a separate information sheet available from the acute pain team to explain this to you. If you are experiencing any pain it is important to tell the nurses so that they can adjust your medication to control this. Usually after a couple of days the pain has lessened so it can be controlled using tablets alone.
You can start drinking small amounts of clear fluid immediately after your surgery. You will also have a drip, which will give you any extra fluids that you need. If you feel sick you are advised not to drink until this feeling has passed. You will be offered medication if the feeling doesn’t go away. You should be able to start eating the day after your surgery.
You will have two flexible tubes coming out of your abdomen, near to the wound; their purpose is to drain away any blood collecting underneath your wound. The tube is connected to a bag or bottle. When the amount of blood coming from the tube has slowed down to only a small amount it can be removed.
A urinary catheter is a tube that runs from the bladder out through the tip of the penis and drains into a bag. It is important to drain the urine in this way until the new connections that are made after removing the prostate have healed. The catheter stays in for 3 weeks (i.e. you go home with it still in).
Discharge information and at home advice
Most patients stay in hospital for approximately 5 days. Your surgeon will monitor your progress and decide when it is appropriate for you to go home.
• You must be eating and drinking normally
• Mild painkillers such as Paracetamol and Voltarol must adequately control any pain
Mild painkillers such as Paracetamol should be enough to deal with any pain
It is important that you do not get constipated. There are no dietary restrictions but you should try and eat plenty of fruit and vegetables and wholemeal bread. If you feel that you may be constipated, see your GP.
Three weeks after your operation, you will be re-admitted to hospital for an overnight stay when you will have you catheter taken out.
If you have any problems with your catheter, you should ring the urological ward for advice. It is very important that your catheter does not block or become dislodged.
Do not allow anyone to remove your catheter unless you have been admitted to hospital
You should take it easy for a month, although it is important to take some gentle exercise like walking, as you will be at a slight risk of developing a blood clot in your legs
During the first 4 weeks you should not:
Recovery takes 6-8 weeks from your operation date; your surgeon will be able to advise you when it will be safe to return to work as this depends on your occupation. The nurse can provide a sick note for your hospital stay, once home they should be obtained from your GP.
You should not attempt to drive a car for 6 weeks after your operation. Your insurance company may refuse to meet a claim if they feel you have driven too soon. It is also advisable to contact your insurance company with regards to cover following a general anaesthetic.
The issue of resuming sexual function will have been discussed with you prior to your surgery as this type of operation affects sexual function. It is an issue that can be revisited post surgery when you feel that the time is right for you to do this. It is rare to get erections immediately after the catheter has been removed, and I may recommend trying some tablets (e.g. Viagra, Levitra, Cialis) in the early phase of recovery to improve the chances of attaining an erection.
We collect and submit data on all my major cancer operations to the British Association of Urological Surgeons for audit (all data is anonymous). I also internally review all my figures for various outcomes specifically related to radical Retropubic prostatectomy. For this reason you are kindly requested to fill in the following 2 questionnaires related to continence and potency, and will be asked to do so again after the operation. This helps me to monitor my results and compare them with other surgeons.
You can hand these questionnaires in to your surgeon on your admission.
PREMEDICATION FOR ARTIFICIAL JOINTS The oral cavity is a portal of entry as well as the site of disease for microbial infections that affect general health. Streptococcus viridian is the main infective agent that can enter the bloodstream from areas with considerable bleeding such as the oral cavity, urinary tract and gastrointestinal tract. This bacteria may lodge on the heart valves, i
E-GOVERNMENT CONCEPT DEVELOPMENT TASK FORCE For attention of reviewers Prime Minister approved this document 6th November 2000. Now it is in the process of reviewing and correcting. Final approval by Government ofLithuania will occur presumably from middle of December to January 2001. During that process your comments concerning all aspects of Concept will be highlyappreciated by Task Force.

 HAVING A LAPAROSCOPIC RADICAL PROSTATECTOMY
HAVING A LAPAROSCOPIC RADICAL PROSTATECTOMY