Thank you, it's cool. Used for the first time because only then was the right drug. Very revealing detail: ordered Express shipping to get the order within 3 hours because didn't know how to get the order faster https://africarx.co.za/buy-cialis-south-africa.html The drug is authentic exactly. Consistent with the stated prices the Staff is knowledgeable.
Psyc.ucalgary.ca
Reduced Basal Ganglia Volumes After Switching to Olanzapine in Chronically Treated Patients With Schizophrenia Donna J. Lang, Ph.D. Objective: A follow-up study of patients Lili C. Kopala, M.D., F.R.C.P.C.
spectively) and did not differ from those of
healthy subjects at the follow-up evalua-
Robert A. Vandorpe, M.D.,
tion. Akathisia was also reduced. In the pa-
F.R.C.P.C. Method: Thirty-seven patients with schizo-
tients receiving risperidone at baseline,
Qing Rui, M.B.
typical antipsychotics (N=10) or risperidone
sponse, and no significant volume changes
Geoffrey N. Smith, Ph.D.
pine. Patients receiving risperidone and ex-
Vina M. Goghari, B.A.
hibiting a good response (N=14) continuedtreatment with risperidone. Caudate, puta-
Conclusions: Olanzapine reversed puta- Jocelyne S. Lapointe, M.D., F.R.C.P.C.
used to assess clinical signs and symptoms. William G. Honer, M.D., F.R.C.P.C. Results: At baseline, basal ganglia vol- umes in patients treated with typical anti-
pallidus: 20.7% larger). After the switch to
(Am J Psychiatry 2004; 161:1829–1836)
Antipsychotic medications are known to alter the patients experiencing decreases and responsive patients
structure and metabolism of basal ganglia in humans and
experiencing no changes in metabolic activity (18). In con-
animals (1–7). In patients with schizophrenia, typical anti-
trast, a study of clozapine and fluphenazine showed that
psychotics induce striatal enlargement, particularly in the
both medications decreased striatal and cingulate glucose
caudate, putamen, and globus pallidus (7–9). In contrast,
metabolism, with female subjects experiencing a greater
the majority of studies of patients switched from typical
change in glucose utilization than male subjects (19). Ris-
antipsychotics to clozapine report decreases in caudate
peridone was also reported to decrease striatal glucose
volume (6, 10–13). The effects in humans of alternate atyp-
metabolism after 6 weeks of treatment (20). Parallel rat
ical antipsychotics (risperidone, olanzapine, quetiapine,
studies showed that haloperidol has little effect on neu-
ziprasidone) are less understood. In one published study,
ronal activity levels in the striatum, whereas risperidone
long-term administration of risperidone did not induce
and clozapine decrease activity in the substantia nigra re-
striatal enlargement (7). The effects seen in animal studies
ticulata nucleus of the basal ganglia system in a dose-de-
are inconsistent. In rats, both increases and decreases in
pendent manner, thus differentially affecting the output of
striatal volumes occur after administration of either halo-
the basal ganglia system (21). Despite their potential for
peridol or clozapine (14, 15). In comparison, long-term
differential effects, few studies have made direct drug-to-
administration of olanzapine in rats decreases striatal
We performed two separate studies to examine in chron-
The effects of antipsychotic medications on basal gan-
ically treated schizophrenia patients the effects on striatal
glia metabolism may vary depending on medication type
volumes of switching from treatment with either typical an-
and patient characteristics (16, 17). Haloperidol does not
tipsychotics or risperidone to olanzapine. In the first study,
reduce striatal glucose metabolism and differentially re-
patients were switched from typical antipsychotic medica-
duces cortical glucose metabolism, with nonresponsive
tions to olanzapine and compared with healthy volunteers. Am J Psychiatry 161:10, October 2004BASAL GANGLIA VOLUME AND OLANZAPINE TABLE 1. Volumetric Data and Clinical Characteristics of Healthy Volunteers and Patients With Schizophrenia Switched From Typical Antipsychotic Treatment to Olanzapine
a Mixed regimens of typical antipsychotics. b Conversions based on the Clinical Handbook of Psychotropic Drugs (31).
Caudate, putamen, and pallidal volumes were expected to
come scans were reported previously for 17 of the healthy com-
decrease after switching from typical antipsychotics to
parison subjects (7). Subjects were recruited through the NovaScotia Early Episode Psychosis Program in Halifax. Approval was
olanzapine. The severity of extrapyramidal symptoms was
obtained from the Dalhousie University Ethics Committee. In-
also expected to decrease after switching. In the second
formed written consent was obtained from all subjects. Exclusion
study, all subjects were taking risperidone at baseline. Sub-
criteria were a history of significant head injury or loss of con-
sequently, a subgroup was switched to olanzapine. The de-
sciousness exceeding 5 minutes, a history of facial or nasal
cision to switch treatments was based on clinical evaluation
trauma, a history of DSM-IV substance abuse, a current diagnosisof substance abuse during treatment or at follow-up, a history of
of the patients’ overall clinical response to risperidone.
seizure disorder, or a family history of psychotic disorders. Pa-
Olanzapine is pharmacologically more similar to clozapine
tients were reassessed after a mean interval of 45.6 weeks.
than risperidone (22), suggesting that the effects of olanza-pine on basal ganglia volumes may be similar to those of
Treatment and Clinical Measures
clozapine (10, 13, 23). Additionally, olanzapine is less likely
Clinical assessments included the Positive and Negative Syn-
to induce extrapyramidal symptoms compared with ris-
drome Scale (27) and the Extrapyramidal Symptom Rating Scale,
peridone at comparable doses, as is clozapine (24–26). In
a comprehensive rating of extrapyramidal symptoms and signs(28). Global scores on the Extrapyramidal Symptom Rating Scale
the second study, basal ganglia volumes were expected to
subscales are reported. Interrater reliability for clinical measures
decrease after switching from risperidone to olanzapine, as
based on intraclass correlations (ICCs) were high (Positive and
Negative Syndrome Scale: ICC=0.85; Extrapyramidal SymptomRating Scale: ICC=0.89). All ratings were performed by trained cli-nicians (L.C.K. and Heather M. Milliken, M.D., F.R.C.P.C.).
The first study investigated the effects of switching from typical
antipsychotics (loxapine, trifluoperazine, chlorpromazine, flu-
Subjects
phenazine, haloperidol) to olanzapine. Some patients were receiv-
Thirty-seven patients with DSM-IV schizophrenia and 23
ing additional anticholinergic medications to ameliorate extra-
healthy comparison subjects were included in this study. No sub-
pyramidal symptoms at baseline (Table 1). No patients required
jects in this study received adjunct treatments for mood disorders
anticholinergic agents at follow-up.
during the course of treatment. The baseline scans of 15 patients
Both patient groups in the second study were being treated
were included in a previous study, and both baseline and out-
with low to moderate doses of risperidone at baseline (Table 2). Am J Psychiatry 161:10, October 2004LANG, KOPALA, VANDORPE, ET AL. TABLE 2. Volumetric Data and Clinical Characteristics of Risperidone-Treated Schizophrenia Patients Switched to Olanzapine or Continuing Treatment With Risperidone
a Conversions based on the Clinical Handbook of Psychotropic Drugs (31).
Thirteen patients were switched to olanzapine treatment, and 14
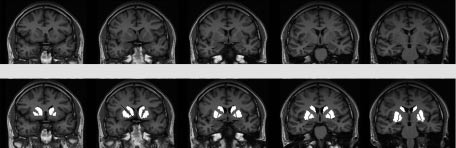
ments began two slices anterior to and ended two slices posterior
continued receiving risperidone. Medications were switched on
to the anterior commissure slice to cover a total distance of 25
the basis of a clinical evaluation by a psychiatrist. Those patients
mm in the anterior commissure-posterior commissure plane
switched from risperidone to olanzapine exhibited more severe
(Figure 1). Anatomically, this protocol excluded the anterior-most
extrapyramidal symptoms and more severe psychiatric symp-
portion of the head of the caudate (5-mm depth), the tail of the
toms at baseline compared with those who continued risperi-
caudate, and the posterior-most putamen. Similarly, the poste-
done treatment (Table 2). Complete follow-up clinical assess-
rior-most globus pallidus was excluded. The rater was blind to di-
ments were available for 10 of the 14 patients who continued
agnosis, treatment, gender, and time of scan. All measures were
risperidone and 11 of the 13 patients switched to olanzapine.
repeated four times. Final volumes were calculated on the mean
No patients in either study required mood stabilizing or antide-
of four repetitions to reduce the possibility of rater error. Volumes
were calculated on absolute slice thickness across all five slices. Total brain volumes were assessed from axial slices. Axial slices
Scanning and Measurement Protocols
were obtained with a T2-weighted sequence; TR/TE=4000/90
Subjects were scanned with a Siemens Magnetom Vision 1.5-
msec, field of view=220 mm, and matrix=238×256 pixels. Slice
Tesla MRI scanner. An inversion recovery sequence in the coronal
thickness for all T2-weighted images was 5 mm with a 1-mm in-
plane was obtained. The inversion recovery sequence was ob-
terslice gap, 22 slices were obtained in each T2-weighted plane.
tained as follows: TR/TE=2000/20 msec, field of view=200 mm,
Digitized slices were measured using a Macintosh G4 PowerMac
matrix=168×256 pixels. A total of 18 slices, 4 mm thick with a 1-
computer. All scans were reviewed by a neuroradiologist (J.S.L.).
mm interslice gap, were available for this sequence. Inversion re-
Intrarater reliability for all regions was greater than 0.90 (caudate:
covery images were chosen for their superior white-gray tissue
ICC=0.98; putamen: ICC=0.96; globus pallidus: ICC=0.97; total in-
contrast. The white-to-gray pixel intensity for the images ob-
tained with the inversion recovery sequence was 1.42, which
Data Analysis: Statistical Methods
compared favorably with three-dimensional volumetric spoiledgradient recall acquisition (pulse sequence) data from the same
Initial comparisons of left and right striatal volumes did not re-
scanner that had a pixel intensity ratio of only 0.89. A trained rater
veal any significant left-right asymmetries, therefore subsequent
made manual selections for all regions of interest using interac-
analyses were based on total (left plus right) volumes. An initial
tive shareware (NIH Image 1.62 pcc) (29). Selections were made
ANOVA of total brain volume did not reveal any differences be-
based on Duvernoy’s atlas of the human brain (30). Measure-
tween groups. Comparisons of the effects of treatment over time
Am J Psychiatry 161:10, October 2004BASAL GANGLIA VOLUME AND OLANZAPINE FIGURE 1. Sample Set of Manually Selected Striatal Regions for Volumetric Measures Raw images Modified images
were made with a repeated measures analysis of variance, with
nificant differences in basal ganglia volumes between pa-
time (baseline, follow-up) and region (caudate, putamen, globus
tients and healthy comparison subjects.
pallidus) as within-subject factors, and group (schizophrenia pa-
At baseline, five of 10 patients being treated with typical
tients, healthy subjects [first study]; continued with risperidone,
antipsychotic agents were receiving adjunct anticholin-
switched to olanzapine [second study]) as a between-subject fac-tor. Multivariate analyses of covariance (MANCOVAs) were per-
ergic medications (Table 1). While mean Extrapyramidal
formed to compare basal ganglia volumes between groups at
Symptom Rating Scale scores decreased following the
baseline or at follow-up, using the factor group, the covariates in-
switch to olanzapine, this was not statistically significant
tracranial volume and age at time of scan, and the dependent
(t=1.82, df=9, p>0.10). However, at follow-up none of the 10
measures caudate, putamen, and globus pallidus volumes.
patients in this group were being treated with anticholin-
For analysis of changes in extrapyramidal symptoms, paired t
ergic medications. Examination of individual Extrapyrami-
tests were used with the Extrapyramidal Symptom Rating Scale
dal Symptom Rating Scale subscores revealed a statistically
data, with Bonferroni alpha set at p=0.01 to control for five com-
significant decrease in akathisia scores (t=3.59, df=19, p=
parisons (total score, parkinsonism, dyskinesia, dystonia, andakathisia). Additional descriptive statistics of anticholinergic us-
0.007) but not in parkinsonism, dystonia, or dyskinesia. Risperidone Continuation Versus Switch to Olanzapine
As seen in Figure 3, basal ganglia volumes of risperi-
Schizophrenia Patients
done-treated patients subsequently switched to olanza-
Versus Healthy Comparison Subjects
pine did not differ at baseline from those continuing treat-ment with risperidone (Wilks’s lambda F=0.55, df=3, 21, p=
At baseline, patients treated with typical antipsychotic
0.65). For analysis of changes over time, the MANCOVA in-
drugs had overall larger basal ganglia structures than
dicated a significant effect of time (F=4.41, df=3, 23,
healthy comparison subjects (Wilks’s lambda F=7.68, df=
p<0.02) but no statistically significant effects of group
3, 27, p=0.0007). Differences were statistically significant
(Wilks’s lambda F=0.25, df=3, 23, p=0.86) or group-by-time
for the putamen (7.0% larger, F=9.11, df=1, 29, p=0.005)
interaction (F=2.87, df=3, 23, p=0.059). At follow-up, no
and the globus pallidus (20.7% larger, F=24.06, df=1, 29, p=
statistically significant differences between the groups in
0.0001). For analysis of changes over time in patients after
overall basal ganglia volumes were observed ( Wilks’s
medication switch relative to comparison subjects, the
MANCOVA indicated statistically significant effects of
Mean total Extrapyramidal Symptom Rating Scale scores
group (Wilks’s lambda F=5.05, df=3, 29, p=0.006), time (F=
at baseline in patients switched to olanzapine were higher
4.82, df=3, 29, p=0.008), and a group-by-time interaction
than scores in patients continuing risperidone treatment
(F=5.61, df=3, 29, p=0.004). As seen in Figure 2, basal gan-
(t=2.85, df=21, p=0.01) (Table 2). Extrapyramidal Symptom
glia volumes decreased over time in the patients switched
Rating Scale total scores at the follow-up evaluation did
from typical antipsychotics to olanzapine, while volumes
not significantly differ from baseline scores for either the
remained steady in healthy comparison subjects. Subse-
patients continuing risperidone treatment (t=–1.00, df=9,
quent analyses indicated volume decreases in the puta-
p>0.34) or those switched to olanzapine (t=–0.37, df=10,
men (smaller by 9.8%) and globus pallidus (smaller by
p>0.70). Examination of the subscales of the Extrapyra-
10.7%) associated with change from typical antipsychotics
midal Symptom Rating Scale did not reveal significant
to olanzapine. At follow-up, there were no statistically sig-
Am J Psychiatry 161:10, October 2004LANG, KOPALA, VANDORPE, ET AL. FIGURE 2. Baseline and Follow-Up Basal Ganglia Volumes FIGURE 3. Baseline and Follow-Up Basal Ganglia Volumes of Healthy Volunteers and Patients With Schizophrenia of Risperidone-Treated Schizophrenia Patients Switched Switched From Typical Antipsychotic Tre atm ent to to Olanzapine or Continuing Treatment With Risperidone Olanzapine Patients Switched Patients Switched From Patients Continuing From Risperidone Typical Antipsychotics Risperidone Treatment to Olanzapine Volunteers to Olanzapine Volume (mm Volume (mm Baseline Follow-Up Follow-Upa Baseline
a Significant decrease from baseline in putamen volume (F=6.62, df=
1, 31, p<0.02) and globus pallidus volume (F=6.02, df=1, 31, p=
Baseline Follow-Up Baseline Follow-Up Discussion
gional inconsistencies may be a reflection of specific ef-fects of previously administered typical antipsychotics or
As expected, treatment with typical antipsychotics was
differences in effects of clozapine and olanzapine. The role
associated with larger basal ganglia volumes, and switch-
of the putamen in both the presentation of schizophrenia-
ing to olanzapine was associated with reduction in basal
related symptoms and extrapyramidal symptoms is not
ganglia volumes. Specifically, the putamen and globus pal-
fully understood. An earlier study by Stratta and colleagues
lidus volumes were normalized following the switch to
(32) demonstrated a significant correlation of performance
olanzapine. The pattern of regional changes differs some-
on the Wisconsin Card Sorting Test and left-sided putamen
what from two earlier reports of the effects of switching
volume, suggesting a role in executive functioning, which
from typical antipsychotic medications to clozapine. Fol-
is known to be affected in schizophrenia (33, 34).
lowing switching, Chakos et al. (3) reported a reduction in
Eight out of 10 patients receiving typical medications at
caudate volume in adult patients, and Frazier et al. (12)
baseline had movement disorders according to the Ex-
found reduction in both the caudate and the globus palli-
trapyramidal Symptom Rating Scale. This scale covers a
dus in childhood-onset schizophrenia patients. The re-
full range of potential motor abnormalities and is sensitive
Am J Psychiatry 161:10, October 2004BASAL GANGLIA VOLUME AND OLANZAPINE
to subtle movement disorders (35). The mean total base-
tial or poor risperidone response. Additional variance in
line Extrapyramidal Symptom Rating Scale scores were
the volumetric measures may have been related to MRI
likely partially ameliorated by anticholinergic medication.
slice thickness and slice angulation. However, a compari-
These are most effective in treating tremors, rigidity, and
son of volumes reported in other studies with thinner
bradykinesia but have low efficacy for treating antipsy-
slices did not reveal any deviation in the volumes reported
chotic-induced akathisia (36). The observed reduction in
akathisia after the switch to olanzapine may be a true re-
Individual atypical antipsychotic agents exhibit specific
flection of olanzapine’s low propensity to induce extrapy-
neurochemical pathways of activity, and this specificity
may contribute to differential volumetric changes in the
In our second study, overall basal ganglia volumes did
striatum in response to antipsychotic challenge (15, 39). In
not differ between patients with good and poor responses
a study of striatal volumes in rats, caudate or putamen vol-
to risperidone. Subsequent switching to olanzapine in
umes were significantly increased by chronic exposure to
those with a poor response to risperidone was not associ-
haloperidol and clozapine (15). In contrast, this same
ated with a significant change in basal ganglia volume.
study found that chronic exposure to risperidone had no
This observation suggests the effects of olanzapine on
effect on caudate or putamen volumes whereas long-term
basal ganglia volume in patients previously treated with
exposure to olanzapine resulted in a significant decrease in
typical antipsychotics represent normalization rather
striatal volumes (15). Additionally, a recent study employ-
ing fMRI in patients with schizophrenia demonstrated dif-
Neither overall symptom severity nor overall extrapyra-
ferential activation of the caudate and putamen during a
midal symptom severity changed when patients with a
cognitive challenge (40). Signal intensity was reduced in
poor response to risperidone were switched to olanza-
the putamen and anterior cingulate during testing in pa-
pine. However, patients previously receiving typical anti-
tients relative to healthy subjects, but not in the caudate.
psychotics did have moderate reductions in dyskinesia
These findings are supported by differential responses to
and akathisia. The extrapyramidal symptoms present in
individual antipsychotic medications (41). These differ-
the group of patients poorly responsive to risperidone
ences are likely related to different receptor-targeting pro-
may be related to a different mechanism, perhaps intrin-
files of specific antipsychotic agents (39). While the evi-
sic to schizophrenia, that is less responsive to switching to
dence for increased striatal volumes in humans or animals
olanzapine than are extrapyramidal symptoms related to
exposed to typical antipsychotic medications treatment is
typical antipsychotic medications. Moreover, relative dos-
convincing (1, 3, 4, 6, 7, 10–12, 14, 15, 42), there are no data
suggesting that clozapine increases striatal volumes. The
from risperidone to olanzapine remained relatively equal,
majority of published reports in human subjects indicated
thus there would be little expectation for a change in ex-
that exposure to clozapine is associated with a reduction in
trapyramidal symptom severity (37). The relationships
striatal volumes in patients previously exposed to typical
among antipsychotic dose, striatal volume, and extrapyra-
antipsychotics (12–14, 23). Studies of risperidone’s and
midal symptom severity are not clear. Data from this study
olanzapine’s effects on striatal volumes after chronic ad-
do not demonstrate any relationship of either total dose or
ministration are far fewer in number (7, 15). The findingsfrom the current study in conjunction with those from ani-
current dose of antipsychotic medication being correlated
mal studies suggest that closer examination in subpopula-
with striatal volumes, change in striatal volumes, or sever-
tions of patients with schizophrenia is required to clarify
ity of extrapyramidal symptoms scores (all exploratory re-
the true physiological and clinical effects of individual an-
gression analyses had r values <0.40 and corresponding p
tipsychotic medications in the treatment of schizophrenia.
values >0.05). This suggests that striatal volume, while re-sponsive to specific types of antipsychotic agents, does
Received May 30, 2003; revision received Dec. 29, 2003; accepted
not affect the presence or severity of extrapyramidal
Jan. 9, 2004. From the Departments of Psychiatry and Radiology, Uni-
versity of British Columbia, Vancouver; and the Departments of Psy-chiatry and Radiology, Dalhousie University, Halifax, N.S., Canada; Ad-
Summary
dress reprint requests to Dr. Lang, VGH Research Pavilion, Centre forComplex Disorders, West 10th Ave., Room 211–828, Vancouver, Brit-
The main findings of the present study were significant
ish Columbia, Canada V5Z 1L8; dlang@interchange.ubc.ca (e-mail).
reductions in putamen and globus pallidus volumes in pa-
Supported by a Canadian Institutes of Health Research Scientist
tients switched to olanzapine from typical antipsychotics.
Award to Dr. Honer and by a grant from the Norma Calder Founda-tion for Schizophrenia Research to Dr. Lang. Dr. Kopala was sup-
These subregional-specific results may be due to differen-
ported by a Clinical Scientist Award from Dalhousie University. Partial
tial effects of olanzapine on striatal structures or of an un-
funding for MRI scanning was provided by investigator-initiated
known sampling bias of the subjects chosen for this study.
grants from Janssen-Ortho of Canada and Eli Lilly Canada. Additionalfunding for scanning was provided by the Queen Elizabeth-II Hospital
As well, the results from the risperidone-to-olanzapine
Health Science Research Foundation and the Department of Psychi-
group may only be valid for those patients who have par-
Am J Psychiatry 161:10, October 2004LANG, KOPALA, VANDORPE, ET AL.
The authors thank Melissa M. Butler, R.T.N.M., C.C.R.C.; Jason O.
amine-induced alterations in regional brain metabolism. J
Brown, B.Sc., R.T.N.M.; Diana L. Sonnichsen, B.Sc., R.T.N.M.; Charlene
A. Day, R.N., M.N.; Janet L. Gallant, R.N., B.Sc., C.N.; Heather M. Mil-
18. Bartlett EJ, Brodie JD, Simkowitz P, Schlösser R, Dewey SL, Lin-
liken, M.D., F.R.C.P.C.; and David Whitehorn, Ph.D., M.Sc.N., for their
denmayer J-P, Rusinek H, Wolkin A, Cancro R, Schiffer W: Effect
of a haloperidol challenge on regional brain metabolism inneuroleptic-responsive and nonresponsive schizophrenic pa-tients. Am J Psychiatry 1998; 155:337–343
References
19. Cohen RM, Nordahl TE, Semple WE, Pickar D: The brain meta-
1. Benes FM, Paskevich PA, Domesick VB: Haloperidol-induced
bolic patterns of clozapine- and fluphenazine-treated female
plasticity of axon terminals in rat substantia nigra. Science
patients with schizophrenia: evidence of a sex effect. Neuro-
2. Benes FM, Paskevich PA, Davidson J, Domesick VB: The effects
20. Liddle PF, Lane CJ, Ngan ET: Immediate effects of risperidone
of haloperidol on synaptic patterns in the rat striatum. Brain
on cortico-striato-thalamic loops and the hippocampus. Br J
3. Chakos MH, Lieberman JA, Bilder RM, Borenstein M, Lerner G,
21. Bruggenman R, Westerink BHC, Timmerman W: Effects of ris-
Bogerts B, Wu H, Kinon B, Ashtari M: Increase in caudate nuclei
peridone, clozapine and haloperidol on extracellular record-
volumes of first-episode schizophrenic patients taking antipsy-
ings of substantia nigra reticulata neurons of the rat brain. Eur
chotic drugs. Am J Psychiatry 1994; 151:1430–1436
4. Chakos MH, Shirakawa O, Lieberman J, Lee H, Bilder R, Tam-
22. Keck PE Jr, McElroy SL: Clinical pharmacodynamics and phar-
minga CA: Striatal enlargement in rats chronically treated with
macokinetics of antimanic and mood-stabilizing medications. J
neuroleptic. Biol Psychiatry 1998; 44:675–684
5. Hokama H, Shenton ME, Nestor PG, Kikinis R, Levitt JJ, Metcalf
23. Scheepers FE, Gispen de Wied CC, Hulshoff Pol HE, Kahn RS: Ef-
D, Wible CG, O’Donnell BF, Jolesz FA, McCarley RW: Caudate,
fect of clozapine on caudate nucleus volume in relation to
putamen, and globus pallidus volume in schizophrenia: a
symptoms of schizophrenia. Am J Psychiatry 2001; 158:644–
quantitative MRI study. Psychiatry Res 1995; 61:209–229
6. Keshavan MS, Bagwell WW, Haas GL, Sweeney JA, Schooler NR,
24. Sacritstan JA, Gomez JC, Ferre F, Gascon J, Perez Bravo A, Oli-
Pettegrew JW: Changes in caudate volume with neuroleptic
vares JM: Incidence of extrapyramidal symptoms during treat-
treatment (letter). Lancet 1994; 344:1434
ment with olanzapine, haloperidol and risperidone: results of
7. Lang DJ, Kopala LC, Vandorpe RA, Rui Q, Smith GN, Goghari VM,
an observational study. Actas Esp Psiquiatr 2001; 29:25–32
Honer WG: An MRI study of basal ganglia volumes in first-epi-
25. Tarsy D, Baldessarini RJ, Tarazi FI: Effects of newer antipsychot-
sode schizophrenia patients treated with risperidone. Am J
ics on extrapyramidal function. CNS Drugs 2002; 16:23–45
26. Miller CH, Mohr F, Umbricht D, Woerner M, Fleishchaker WW,
8. Shenton ME, Dickey CC, Frumin M, McCarley RW: A review of
Lieberman JA: The prevalence of acute extrapyramidal signs
MRI findings in schizophrenia. Schizophr Res 2001; 49:1–52
and symptoms in patients treated with clozapine, risperidone,
9. Raz S, Raz N: Structural brain abnormalities in the major psy-
and conventional antipsychotics. J Clin Psychiatry 1998; 59:69–
choses: a quantitative review of the evidence from computer-
ized imaging. Psychol Bull 1990; 108:93–108
27. Kay SR, Opler LA, Fiszbein A: Positive and Negative Syndrome
10. Chakos MH, Lieberman JA, Alvir J, Bilder R, Ashtari M: Caudate
Scale (PANSS). Toronto, Multi-Health Systems, 1987
nuclei volumes in schizophrenic patients treated with typical
28. Chouinard G, Ross-Chouinard A, Annable L, Jones B: Extrapyra-
antipsychotics or clozapine. Lancet 1995; 345:456–457
midal Symptom Rating Scale (abstract). Can J Neurol Sci 1980;
11. Corson PW, Nopoulos P, Miller DD, Arndt S, Andreasen NC:
Change in basal ganglia volume over 2 years in patients with
29. Rasband W: NIH Image. Rockville, Md, National Institutes of
schizophrenia: typical versus atypical neuroleptics. Am J Psy-
30. Duvernoy HM: The Human Brain: Surface, Three-Dimensional
12. Frazier JA, Giedd JN, Kaysen D, Albus K, Hamburger S, Alagh-
Sectional Anatomy and MRI. New York, Springer-Verlag Wien,
band-Rad J, Lenane MC, McKenna K, Breier A, Rapoport JL:
Childhood-onset schizophrenia: brain MRI rescan after 2 years
31. Bezchlibnyk-Butler KZ, Jeffries JJE: Clinical Handbook of Psy-
of clozapine maintenance treatment. Am J Psychiatry 1996;
chotropic Drugs. Toronto, Hogrefe & Huber, 1999
32. Stratta P, Mancini F, Mattei P, Daneluzzo E, Casacchia M, Rossi
13. Scheepers FE, de Wied CC, Pol HE, van de Flier W, van der Lin-
A: Association between striatal reduction and poor Wisconsin
den JA, Kahn RS: The effects of clozapine on caudate nucleus
Card Sorting Test performance in patients with schizophrenia.
volume in schizophrenic patients previously treated with typi-
cal antipsychotics. Neuropsychopharmacology 2001; 24:47–54
33. Townsend LA, Malla AK, Norman RMG: Cognitive functioning in
14. Lee H, Tarazi FI, Chakos M, Wu H, Redmond M, Alvir JM, Kinon
stabilized first-episode psychosis patients. Psychiatry Res 2001;
BJ, Creese I, Lieberman JA: Effects of chronic treatment with
typical and atypical antipsychotic drugs on the rat striatum.
34. Bryson G, Whelahan HA, Bell M: Memory and executive func-
tion impairments in deficit syndrome schizophrenia. Psychia-
15. Andersson C, Hamer RM, Lawler CP, Mailman RB, Lieberman
JA: Striatal volume changes in the rat following long-term ad-
35. De Deyn PP, Wirshing WC: Scales to assess the efficacy and
ministration of typical and atypical antipsychotic drugs. Neu-
safety of pharmacologic agents in the treatment of behavioral
and psychological symptoms of dementia. J Clin Psychiatry
16. Colangelo V, Di Grezia R, Passarelli F, Musicco M, Pontieri FE,
Orzi F: Differential effects of acute administration of clozapine
36. Lima AR, Weiser KVS, Bacaltchuk J, Barnes TRE: Anticholin-
or haloperidol on local cerebral glucose utilization in the rat.
ergics for neuroleptic-induced acute akathisia. Cochrane Data-
17. Duncan GE, Miyamoto S, Leipzig JN, Lieberman JA: Comparison
37. Kapur S, Zipursky RB, Remington G: Clinical and theoretical im-
of the effects of clozapine, risperidone, and olanzapine on ket-
plications of 5-HT2 and D2 receptor occupancy of clozapine,
Am J Psychiatry 161:10, October 2004BASAL GANGLIA VOLUME AND OLANZAPINE
risperidone, and olanzapine in schizophrenia. Am J Psychiatry
of reduced left prefrontal activation in schizophrenia during
normal inhibitory function. Schizophr Res 2001; 52:47–55
38. Gur RE, Maany V, Mozley PD, Swanson C, Bilker W, Gur RC: Sub-
41. Miller DD, Andreasen NC, O’Leary DS, Rezai K, Watkins GL,
cortical MRI volumes in neuroleptic-naive and treated patients
Boles Ponto LL, Hichwa RD: Effect of antipsychotics on regional
with schizophrenia. Am J Psychiatry 1998; 155:1711–1717
cerebral blood flow measured with positron emission tomog-
39. Sakai K, Gao XM, Hashimoto T, Tamminga CA: Traditional and
raphy. Neuropsychopharmacology 1997; 17:230–240; correc-
new antipsychotic drugs differentially alter neurotransmission
markers in basal ganglia-thalamocortical neural pathways.
42. Dean B, Hussain T, Scarr E, Pavey G, Copolov DL: Extended
treatment with typical and atypical antipsychotic drugs differ-
40. Rubia K, Russell T, Bullmore ET, Soni W, Brammer M, Simmons
ential effects on the densities of dopamine D2-like and GABAA
A, Taylor E, Andrew C, Giampietro V, Sharma T: An fMRI study
receptors in rat striatum. Life Sci 2001; 69:1257–1268
Am J Psychiatry 161:10, October 2004
Note: The data below are based on cases identified as “Asperger Syndrome” N=1,366 PARENT RATINGS OF BEHAVIORAL EFFECTS OF BIOMEDICAL INTERVENTIONS Autism Research Institute ● 4182 Adams Avenue ● San Diego, CA 92116 The parents of autistic children represent a vast and important reservoir of information on the benefits—and adverse effects— of the large variety of drugs and
LISTINO PREZZI / PRICE LIST 2014 VILLAGGIO ISAMAR Via Isamar, 9 - I 30015 Isolaverde - Chioggia (Venezia) Tel: +39 (0)41 - 5535811 Fax: +39 (0)41 - 490440 e-mail: booking@villaggioisamar.com 00 800 17112009 www.villaggioisamar.com UNITA' ABITATIVE / HOUSING UNITS Prezzo in Euro per notte 4 persone inclusePrice in Euro per night 4 persons included BUNGALOW (14/6-6/9: giorno di arri
 BASAL GANGLIA VOLUME AND OLANZAPINE
BASAL GANGLIA VOLUME AND OLANZAPINE