Ordered, immediately called back and the same day delivered the order.Very pleased with the work. Thank you for prompt and accurate work https://africarx.co.za/buy-cialis-south-africa.html great prices, delivered on the day of the order. Pleasant managers consult by phone.
Malaria notes class set
Malaria A disease of the developing world Introduction
There were an estimated 350-500 mil ion cases of malaria worldwide in 2009. An estimated 655,000 people died from malaria in 2010, a 18% decrease from the 781,000 who died in 2009, accounting for 2.23% of deaths worldwide. 90% of malaria deaths occur in sub-Saharan Africa, with the majority of deaths being young children. Plasmodium falciparum, the most severe form of malaria, is responsible for the vast majority of deaths (90%). Malaria is commonly associated with poverty, and can indeed be a cause of poverty and a major hindrance to economic development. History of malaria Malaria has infected humans for over 50,000 years, and Plasmodium may have been a human pathogen for the entire history of the species. References to the unique periodic fevers of malaria are found throughout recorded history, beginning in 2700 BC in China. Malaria may have contributed to the decline of the Roman Empire,104 and was so pervasive in Rome that it was known as the "Roman fever". A number of regions in ancient Rome were considered at- risk for the disease because of the favorable conditions present for the mosquitoes. This included areas such as: southern Italy, Sardinia and the city of Rome along the Tiber River. The presence of stagnant water in these places were preferred by mosquitoes for breeding grounds. Irrigated gardens, swamp-like grounds, runoff from agriculture, and drainage problems from road construction led to the increase of standing water. The term malaria originates from Medieval Italian: mala aria — "bad air"; the disease was formerly cal ed marsh fever due to its association with swamps and marshland. Malaria was once common in most of Europe and North America, where it is no longer endemic, though imported cases do occur. Malaria was the most important health hazard encountered by U.S. troops in the South Pacific during WWII, where about 500,000 men were infected. 60,000 American soldiers died of malaria during their campaigns. History: Discovery of the parasite Scientific studies on malaria made their first significant advance in 1880, when a French army doctor working in the military hospital of Constantine in Algeria named Charles Louis Alphonse Laveran observed parasites for the first time, inside the red blood cells of people suffering from malaria. He, therefore, proposed that malaria is caused by this organism, the first time a protist was identified as causing disease. For this and later discoveries, he was awarded the 1907 Nobel Prize for Physiology or Medicine. The malarial parasite was cal ed Plasmodium. History: Discovery of mosquito transmission In 1881 Carlos Finlay, a Cuban doctor treating patients with yellow fever in Havana, provided strong evidence that mosquitoes were transmitting disease to and from humans. In April 1894, a Scottish physician Sir Ronald Ross visited Sir Patrick Manson at his house on Queen Anne Street, London. This visit was the start of four years of col aboration and fervent research which culminated in 1898 when Ross proved the complete life-cycle of the malaria parasite in mosquitoes; thus proving that the mosquito was the vector for malaria in humans. He did this by showing that certain mosquito species transmit malaria to birds. He isolated malaria parasites from the salivary glands of mosquitoes that had fed on infected birds. For this work, Ross received the 1902 Nobel Prize in Medicine. After resigning from the Indian Medical Service, Ross worked at the newly established Liverpool School of Tropical Medicine and directed malaria- control efforts in Egypt, Panama, Greece and Mauritius. Malaria precautions were enacted by Wil iam Gorgas during the construction of the Panama Canal. This public-health work saved the lives of thousands of workers and helped develop the methods used in future public-health campaigns against the disease. History of treatment The first effective treatment for malaria came from the bark of cinchona tree, which contains quinine. This tree grows on the slopes of the Andes, mainly in Peru. The indigenous peoples of Peru made a tincture of cinchona to control malaria. The Jesuits noted the efficacy of the practice and introduced the treatment to Europe during the 1640s, where it was rapidly accepted. It was not until 1820 that the active ingredient, quinine, was extracted from the bark, isolated and named. In the 20th century, chloroquine replaced quinine as treatment of both uncomplicated and severe falciparum malaria until resistance supervened. Artemisinins, discovered by Chinese scientists in the 1970s, are now recommended treatment for falciparum malaria, administered in combination with other antimalarials as well as in severe disease. Society and culture Malaria is not just a disease commonly associated with poverty but also a cause of poverty and a major hindrance to economic development. Tropical regions are affected most; however, malaria’s furthest extent reaches into some temperate zones with extreme seasonal changes. The disease has been associated with major negative economic effects on regions where it is widespread. During the late 19th and early 20th centuries, it was a major factor in the slow economic development of the American southern states. A comparison of average per capita GDP in 1995, adjusted for parity of purchasing power, between countries with malaria and countries without malaria gives a fivefold difference ($1,526 USD versus $8,268 USD). In countries where malaria is common, average per capita GDP has risen (between 1965 and 1990) only 0.4% per year, compared to 2.4% per year in other countries. Poverty is both cause and effect, however, since the poor do not have the financial capacities to prevent or treat the disease. In its entirety, the economic impact of malaria has been estimated to cost Africa £8 bil ion every year. The economic impact includes costs of health care, working days lost due to sickness, days lost in education, decreased productivity due to brain damage from cerebral malaria, and loss of investment and tourism. In some countries with a heavy malaria burden, the disease may account for as much as 40% of public health expenditure, 30–50% of inpatient admissions, and up to 50% of outpatient visits. Malaria in Famous Victims and Florida Sufferers Epidemiology (Focus on the disease itself)
The continued existence of malaria in an area requires a combination of high human population density, high mosquito population density and high rates of transmission from humans to mosquitoes and from mosquitoes to humans. If any of these is lowered sufficiently, the parasite wil sooner or later disappear from that area, as happened in North America, Europe and much of the Middle East. However, many countries are seeing an increasing number of imported malaria cases owing to extensive travel & migration.
Malaria is presently endemic in a broad band around the equator, in areas of the Americas, many parts of Asia, and much of Africa; however, it is in sub-Saharan Africa where 85 - 90% of malaria fatalities occur. The geographic distribution of malaria within large regions is complex, and malaria-afflicted and malaria-free areas are often found close to each other. Malaria is prevalent in tropical regions because of the significant amounts of rainfal and consistent high temperatures; warm, consistent temperatures and high humidity, along with stagnant waters in which mosquito larvae readily mature, providing them with the environment they need for continuous breeding.
In drier areas, outbreaks of malaria can be predicted with reasonable accuracy by mapping rainfal . Malaria is more common in rural areas than in cities; this is in contrast to dengue fever where urban areas present the greater risk. For example, several cities in Vietnam, Laos and Cambodia are essential y malaria-free, but the disease is present in many rural regions. By contrast, in Africa malaria is present in both rural and urban areas, though the risk is lower in the larger cities.
By 2010 countries with the highest death rate per 100,000 population are Cote d'Ivoire with (86.15), Angola (56.93) and Burkina Faso (50.66) — al in Africa.
Cause of Malaria Malaria is caused by a tiny parasite cal ed plasmodium in a person’s bloodstream. Four species of plasmodium can infect and be transmitted by humans. Severe disease is largely caused by Plasmodium falciparum while the disease caused by Plasmodium vivax, Plasmodium ovale, and Plasmodium malariae is general y a milder disease that is rarely fatal. The disease results from the multiplication of Plasmodium parasites within red blood cells, causing symptoms that typical y include fever and headache, in severe cases progressing to coma or death. Life cycle The Plasmodium parasite's secondary hosts are humans and other vertebrates. Female mosquitoes of the Anopheles genus are the primary transmission vectors. Young mosquitoes first ingest the malaria parasite by feeding on the blood of an infected human carrier and the infected Anopheles mosquitoes carry Plasmodium antibodies in their salivary glands. Once ingested, the parasite gametocytes taken up in the blood wil further differentiate into male or female gametes and then fuse in the mosquito's gut. This produces an ookinete that penetrates the gut lining and produces an oocyst in the gut wal . When the oocyst ruptures, it releases sporozoites that migrate through the mosquito's body to the salivary glands, where they are then ready to infect a new human host. The sporozoites are injected into the skin, alongside saliva, when the mosquito takes a subsequent blood meal. Only female mosquitoes feed on blood while male mosquitoes feed on plant nectar, thus males do not transmit the disease. The females of the Anopheles genus of mosquito prefer to feed at night. They usual y start searching for a meal at dusk, and wil continue throughout the night until taking a meal. The life cycle of malaria parasites in the human body. A mosquito infects a person by taking a blood meal. First, sporozoites enter the bloodstream, and migrate to the liver. They infect liver cells (hepatocytes), where they multiply into merozoites, rupture the liver cells, and escape back into the bloodstream. Then, the merozoites infect red blood cells, where they develop into ring forms, trophozoites and schizonts which in turn produce more merozoites. Sexual forms (gametocytes) are also produced, which, if taken up by a mosquito, wil infect the insect and continue the life cycle. Method of transmission Malaria is a mosquito-borne infectious disease of humans and other animals
• The plasmodium parasite enters a person’s bloodstream when they are bitten by a mosquito. • Not al mosquitoes carry the disease. Only the female anopheles mosquito spreads malaria• It bites an infected person and sucks blood containing the parasite into its stomach. • The parasite then multiplies in the mosquito’s stomach. • The mosquito then bites someone else and the parasite enters the new victim on the saliva of the mosquito. Mosquito FAQs How fast can mosquitoes fly? Depending upon the species, mosquitoes can fly at about 1 to 1.5 miles per hour. How far can mosquitoes fly? Mosquito species preferring to breed around the house, like the Asian Tiger Mosquito, have limited flight ranges of about 300 feet. Most species have flight ranges of 1-3 miles. The undisputed champions, though, are the saltmarsh breeders - having been known to migrate up to 100 miles in exceptional circumstances, although 20 to 40 miles are much more common when hosts are scarce. When caught up in updrafts that direct them into winds high above the ground, mosquitoes can be carried great distances. How much do they weigh? Smal er species found around houses commonly weigh about 2.5 mil igrams. Our largest species weigh in at a whopping 10 mil igrams! How much blood does a mosquito take in a meal? When feeding to repletion, mosquitoes imbibe anywhere from 0.001 to 0.01 mil ilitre. Why do mosquitoes feed on blood? Female mosquitoes imbibe blood so that their eggs can mature prior to laying. It serves no nourishment function. Males do not take blood meals at al . In order to obtain energy, both male and female mosquitoes feed upon plant nectars - much in the same manner as honeybees. How long do mosquitoes live? Lifespan vary by species. Most adult female mosquitoes live 2-3 weeks. Some species that over-winter in garages, culverts and attics can live as long as 6 months. How high do mosquitoes fly? In general, mosquitoes that bite humans prefer to fly at heights of less than 25 ft. Asian Tiger Mosquitoes have been found breeding in treeholes over 40 feet above ground. In Singapore, they have been found in apartments 21 stories above ground. Mosquitoes have been found breeding up to 8,000 feet in the Himalayas and 2000 feet underground in mines in India. What attracts mosquitoes to me? Why some people seem to be more attractive than others to mosquitoes is the subject of much repellent (and attractant for traps) research being conducted nationwide. Carbon dioxide is the most universal y recognized mosquito attractant and draws mosquitoes from up to 35 meters. When female mosquitoes sense carbon dioxide they usual y adopt a zigzagging flight path within the plume to locate its source. Once in the general vicinity of a potential host, other cues predominate, including body odours (sweat, lactic acid, etc.) and heat. Odours produced by skin microflora also play a part in inducing the mosquito to land. Over 350 compounds have been isolated from odours produced by human skin. Either singly or in combination, many of these compounds may be attractants - and many may be repellents. Visual stimuli, such as movement, also factor into host-seeking. What can be safely stated, though, is that ingestion of garlic, vitamin B12 and other systemics has been proven in control ed laboratory studies to have no impact on mosquito biting. Conversely, eating bananas did not attract mosquitoes as the myth suggests, but wearing perfumes does. People drinking beer have been shown to be more attractive to mosquitoes. Limburger cheese has also been found to be attractive. Scientists have suggested that this may explain the attraction some mosquitoes find for human feet! Malaria and Society Environmental Factors
(1) There are physical factors that determine where malaria occurs:
• The mosquitoes live in warm and hot areas, where temperatures are above 16oC. • Areas of shade in which the mosquito can digest human blood. Hot wet climates such as those experienced in
the tropical rainforests or monsoon areas of the world are therefore ideal.
• They need also stil (stagnant) water surfaces as breeding areas, but these areas do not need to be large. A filled
• As a result, al warm, rainy areas with stil or slow-moving water are suitable environments for the anopheles
(2) Human factors (people’s activities) also affect the distribution of malaria.
• Where people have created padi fields, built dams and made irrigation channels, they have created suitable
breeding grounds for the mosquito and so malaria increases.
• People migrate (e.g., migrant workers) and travel (e.g., holiday makers) much more now and this makes it easier
• Nearby settlements with high density living to provide a ‘blood reservoir’. • Areas of bad sanitation, often in urban slums or poor rural areas which often have open sewers and cess pits• Exposure of bare skin by using short sleeved tops or shorts/dresses. • Sufferers not completing courses of medication properly, often through ignorance or misunderstanding
western drugs as magic pil s (e.g., the more you take, the quicker you get better).
Symptoms and consequences of malaria Malaria is a horrendous disease. Symptoms of malaria depend on the Plasmodium species, but in most cases develop between seven and thirty days after the bite of an infected mosquito. The symptoms are as fol ows:
• The infected person initial y suffers headaches and stomach pains. • This is then fol owed by fevers of high temperature and shivering fits lasting four to six hours, occurring every
• More seriously, cerebral malaria can develop, frequently building to a coma and final y in the death of the victim. • If malaria does not kil the victim, it can cause kidney failure. • When properly treated, a patient with minor malaria can expect a complete recovery. In the most severe cases
of the disease, fatality rates can exceed 20%, even with intensive care treatment.
• It leaves the patient weak and anaemic and prone to other diseases. Susceptible people
• The person’s life expectancy is reduced considerably. • Malaria is a particularly big kil er of children, who have not had time to build up immunity from the disease. • Pregnant women are also very susceptible to the disease. • Areas that have malaria also suffer economical y. In areas where malaria occurs, many people wil have the
disease. As a result, the amount of wealth (from farms and factories) that the area produces is seriously reduced because many people are too sick to work. Broader consequences for the endemic areas Areas that have malaria also suffer economical y. In areas where malaria occurs, many people wil have the disease. As a result, the amount of wealth (from people working on farms and in factories and offices) that the area produces is seriously reduced because many people are too sick to work. At the same time a lot of time and money has to be spent on caring for al the victims. In the Philippines in SE Asia, when malaria was rife in the 1940s, 35% of the working population was absent from work because of the disease. Many young people can miss out on years of education. Controlling malaria
At present there are a number of ways in which the disease is attacked. However, no one solution has been found that is total y effective. Most control methods have their problems and difficulties:
Focussing on the parasite Antimalarial Drugs/Prophylactics
Malaria can be treated using prophylactic (preventative) drugs. Quinine was used historical y, however the
development of more effective alternatives such as chloroquine mefloquine (Lariam), and malarone in the 20th
century reduced its use. Today, quinine is not general y used for prophylaxis. Research into successful drug
treatment is on-going as those in use are becoming ineffective because the parasites have built up resistance to
them. General y, these drugs are taken daily or weekly.
• These prophylactic drugs are seldom practical for full-time residents of malaria-endemic areas. Their use
is usual y restricted to short-term visitors and travelers to malarial regions. This is due to cost and the negative side effects (personality changes and mood swings) from long-term use.
• It is much cheaper to prevent the disease rather than cure it. Treatment for malaria
• The prophylactics are used at a higher dose in the case of a person who has actual y contracted the
disease. Severe malaria was treated with intravenous or intramuscular quinine.
• Resistance has developed to several antimalarial drugs, most notably Chloroquine. • Artemisinins, a traditional Chinese medicine, discovered by scientists in the 1970s, are now the
recommended and superior treatment for malaria, administered in combination with other antimalarials. This is known as ACT (artemisinin-combination therapy). This is used in order to avoid the development of drug resistance against artemisinin-based therapies. Prevention: Immunisation - a vaccine for malaria
The chal enge of producing a widely available vaccine that provides a high level of protection for a sustained
period is stil to be met, although several are under development. Immunity does occur natural y, but only in
response to repeated infection with multiple strains of malaria. SPf was tested extensively in endemic areas in
the 1990s, but clinical trials showed it to be insufficiently effective. Other vaccine candidates, targeting the
blood-stage of the parasite's life cycle, have also been insufficient on their own. Focussing on the mosquito as an adult Spray insecticides (e.g. DDT) on breeding grounds and in and around houses.
After feeding, many mosquito species rest on a nearby surface while digesting the bloodmeal, so if the wal s of
dwellings have been coated with insecticides, the resting mosquitos wil be kil ed before they can bite another
victim, transferring the malaria parasite.
The first pesticide used was DDT. Overspraying of DDT on crops led to DDT resistance in Anopheles
mosquitoes. Since the use of DDT has been limited or banned for agricultural use for some time, DDT may now
be more effective as a method of disease-control.
• chemicals pol ute the environment, kil ing other life forms. • they are expensive. • mosquitoes are stil becoming resistant to them. Creating a mosquito barrier: Insecticide-treated bed nets
Mosquito nets help keep mosquitoes away from people and greatly reduce the infection and transmission of
malaria. The nets are not a perfect barrier and they are often treated with an insecticide designed to kil the
mosquito before it has time to search for a way past the net. Insecticide-treated nets (ITNs) are estimated to be
twice as effective as untreated nets and offer greater than 70% protection compared with no net. Although ITNs
are proven to be very effective against malaria, less than 2% of children in urban areas in Sub-Saharan Africa are
Genetic engineering
Scientists have ‘doctored’ male mosquitoes to make them sterile. These male mosquitoes are then released into
the wild and are unable to mate with the female mosquito to produce offspring.
• expensive to do• public concern about such research
Sterile insect technique is emerging as a potential mosquito control method. Progress towards transgenic, or genetical y modified, insects suggest that wild mosquito populations could be made malaria-resistant. Prevention: Hi-Tech! Furthering attempts to reduce transmission rates, a proposed alternative to mosquito nets is the mosquito laser, or photonic fence, which identifies female mosquitoes and shoots them using a medium-powered laser. The device is currently undergoing commercial development, although instructions for a DIY version of the photonic fence have also been published. Focussing on the mosquito as a larvae/pupae Drain breeding grounds
• very expensive• requires large inputs of manpower• impossible to do thoroughly, as only smal areas of water are needed, e.g. pot holes in roads. • water is also needed for drinking, washing, for crops and animals. Destruction of larvae by spraying oil onto the water surface
• the film of oil suffocates the larvae, however, it is expensive and wasteful• it pol utes water sources and kil s wildlife. Mustard seed ‘bombing’
This is when mustard seeds are thrown into the breeding grounds. The seeds become wet and sticky in water
and drag the mosquito larvae below the surface and drown them.
• difficult to do thoroughly over large areas• wasteful
Egg-white sprayed on stagnant water surfaces
This suffocates the larvae by clogging up their breathing tubes.
• wasteful and impractical (what happens to al those egg yolks!)• difficult to do thoroughly over large areas
Larvae-eating fish
• The smal fish eat mosquito larvae and they provide an added source of protein in the people’s diet
Bti bacteria grown in coconuts
Fermented coconuts are, after a few days, broken open and thrown into mosquito-infested water. Larvae eat the
bacteria and have their stomach linings destroyed and die!
• cheap to produce• environmental y friendly bacteria which is harmless to livestock and humans• coconuts are plentiful and often grow beside ponds infested with mosquito larvae• 2 to 3 coconuts wil ‘control’ a smal pond for up to 45 days
Restricting the breeding areas Malaria was successfully eradicated or control ed also in several tropical areas by removing or poisoning the breeding grounds of the mosquitoes or the aquatic habitats of the larva stages, for example by filling or applying oil to places with standing water. Additional y, larvae eating fish are placed in water sources to remove the mosquito larvae before they become a threat to the human population. Obstructions are also removed from these sources in order to maintain water flow and reduce stagnant water. Similarly, marsh or swamp-like environments are drained and filled to diminish mosquito breeding grounds. Focussing on education Prevention: Education Education in recognizing the symptoms of malaria has reduced the number of cases in some areas of the developing world by as much as 20%. Recognizing the disease in the early stages can also stop the disease from becoming a kil er. Education can also inform people to cover over areas of stagnant, stil water e.g. water tanks (open communal areas in Indian vil ages) which are ideal breeding grounds for the parasite and mosquito, thus cutting down the risk of the transmission between people. This is most put in practice in urban areas where there are large centers of population in a confined space and transmission would be most likely in these areas. Education Local health campaigns may be very successful, especial y primary health care. This is discussed in more detail under in the section below.
• requires manpower and organisational skil s• requires to be communicated in the correct way, e.g., drama to il iterate people and correct metaphors and
• people need to be persuaded to change their lifestyles, both in the large things (moving a whole vil age away
from an infested area) and in the smal things (e.g., wearing long sleeved clothes
Eradication efforts Historical An early effort at malaria prevention occurred in 1896, just before the mosquito malaria link was confirmed in India by a British physician, Ronald Ross. The WHO (World Health Organisation) launched a world campaign to eradicate malaria in the 1950s and 1960s. They used drugs to cure people and insecticides to kil mosquitoes. This was very successful initial y and malaria was reduced. But, the campaign final y failed because
• it was very expensive for poor countries to buy insecticides, and• the mosquitoes were becoming resistant to the chemicals used.
WHO were responsible for the development of DDT and, when that became less effective developed, dieldrin. They have also been responsible for introducing sterile male mosquitoes and fish that eat mosquito larvae. Geographical A 2008 study that examined international financing of malaria control found large regional variations in the levels of average annual per capita funding ranging from 1p per head in Myanmar to £1 per head in Suriname. There are 16 countries where funding was 3p per head or less, including seven of the poorest countries in Africa (Ivory Coast, Congo, Chad, Mali, DR Congo, Somalia, and Guinea) and two of the most densely populated stable endemic countries in the world (Indonesia and India). Brazil, Eritrea, India, and Vietnam, unlike many other LEDC’s nations, have successfully reduced the malaria burden. Rationale for recent high investment approaches Many researchers argue that prevention of malaria may be more cost-effective than treatment of the disease in the long run, but the capital costs required are out of reach of many of the world's poorest people. The economist Jeffrey Sachs estimates that malaria can be control ed for £2 bil ion in aid per year.
Several notable attempts are being made to eliminate the parasite from sections of the world, or to eradicate it worldwide. In 2006, the organization Malaria No More set a public goal of eliminating malaria from Africa by 2015, and the organization plans to dissolve if that goal is accomplished.
The WHO Roll Back Malaria campaign. Research carried out by the Bil and Melinda Gates Foundation.
The U.S.-based Clinton Foundation has reduced the cost of drugs to treat malaria by 60%, and is working to further reduce the spread of the disease. Other efforts, such as the Malaria Atlas Project focus on analyzing climate and weather information required to accurately predict the spread of malaria based on the availability of habitat of malaria- carrying parasites. Malaria has been successfully eradicated in certain areas. The Republic of Mauritius, a tropical island located in the western Indian Ocean, considered ecological connections to malaria transmission when constructing their current plan for malaria control. In order to prevent mosquitoes from breeding in aquatic areas, DDT is used in moderate amounts. The role of aid agencies: the Red Cross The Red Cross provides emergency medical help (e.g. drugs, equipment, nurses) when epidemics of malaria occur. They believe as well that prevention is better than cure. So they also provide longterm medical help to improve health conditions, especial y in countryside areas. This involves taking someone from each vil age and training them in Primary Health Care. That person then becomes a vil age health worker. Primary Health Care includes giving advice on how diseases such as malaria are spread and low-cost ways of reducing these diseases. These methods include:
• persuading people to use mosquito bednets• covering water containers• filling in puddles• reducing visits to the river• cut grass around houses, because mosquitoes use tal grass for resting)• wear clothing which covers your arms and legs, especial y at night, when mosquitoes are most active Fig 6:
Primary Health care can be very effective because it involves the local people (locals are more likely to listen to, and trust, one of their own people instructing them, rather than an outsider). Their workers also use cheap methods which are affordable by the vil agers. The benefits of controlling the disease on a LEDC might include:
• Saving money on health, medicines, doctors, drugs etc. • Reduction in the national debt. • Healthier workforce and increased productivity. the workforce wil be fitter (eg farmers better able to produce
food), thus also helping to raise health levels productivity wil increase as the workforce takes less sick leave and decreased infant mortality rates.
• Scarce financial resources could be spent on other areas such as education or housing. • More tourists/foreign investment may be attracted if there was less risk of disease - leading to more job
opportunities, foreign currency earnings and increased prosperity.
IL MATTINO LA PRIMA PROVA SCRITTA IN PROGRAMMA IL 25 GIUGNO Esami di maturità, ecco le commissioni I COMMISSIONE SPERIMENTALE CO "R.LIVATINO", VIA G. MATTEOTTI N. 2 (BN)BENEVENTO - ISTITUTO MAGISTRALE IM G.GUACCI BENE- Istituto prima sede: PONTELANDOLFO - IST PROF INDUSTRIA E Presidente: MOTTOLA LUIGI N. IL 14/10/1957 (BN) - MORCONE - Indirizzo: PC00 - CLASSICO 2 - M770
BMJ. BRITISH MEDICAL JOURNAL VOL. 322, NO. 7277; 6 JANUARY 2001 EDITORIALSPubMed Central: creating an Aladdin´s cave of ideasTony Delamothe, Richard SmithA new mental health (and public protection) actGeorge SmzuklerThe renaissance of C reactive proteinMark B Pepys, Abi Berger"Normal" blood glucose and coronary riskElizabeth Barrett-Connor , Deborah L WingardNEWSCommons votes fo
 Malaria
Malaria Society and culture
Society and culture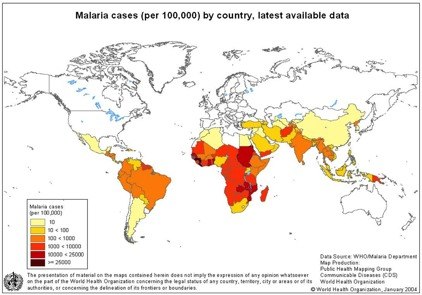 Epidemiology (Focus on the disease itself)
Epidemiology (Focus on the disease itself)