Thank you, it's cool. Used for the first time because only then was the right drug. Very revealing detail: ordered Express shipping to get the order within 3 hours because didn't know how to get the order faster https://africarx.co.za/ The drug is authentic exactly. Consistent with the stated prices the Staff is knowledgeable.
Microsoft word - sl100297.doc
Progesterone ELISA Kit
Enzyme immunoassay kit for the quantitative determination of
Human Progesterone concentration in serum.
For in vitro diagnostic use only.
Email: info@signagenlabs.com Web Site: www.signagenlabs.com
TABLE OF CONTENTS
INTENDED USE
Enzyme immunoassay (EIA) permits the routine quantitative determination of many steroid hormones in body fluids and provides an accurate, sensitive, reproducible, rapid and specific assay. This enzyme immunoassay method makes it possible to measure very low concentration of Progesterone in small volumes of serum (0.025 mL per well). INTRODUCTION
Progesterone is a steroid hormone, which plays an important role in the preparation for and maintenance of pregnancy. It is synthesized from cholesterol via pregnenolone then rapidly metabolized to pregnanediol, for the most part, in the liver. 1,8,10 The ovary and placenta are the major production sites, but a small amount is also synthesized by the adrenal cortex in both men and women. Circulating Progesterone levels, which are characteristically low during the follicular phase, increase sharply during the luteal phase of menstrual cycles, reaching a maximum some 5 to 10 days after the mid-cycle LH peak.9 Unless pregnancy occurs, a steep decline to follicular levels sets in about 4 days before the next menstrual period. This pattern constitutes the rationale behind the well-established use of serum Progesterone measurements as a simple and reliable method for ovulation detection. 2,3,13 There is growing literature on luteal phase defects. 4,7,16,14,15 Daily Progesterone levels are considered the most accurate means for documenting a defective luteal phase.4,7 However, some investigators have found that three samples 17 or even a single sample
11,13 (if well timed) can provide valuable information on the adequacy of the luteal phase. Measurements of serum Progesterone have also been used to check the effectiveness of ovulation induction, 13 to monitor Progesterone replacement therapy 5 and to detect and evaluate patients at risk for abortion during the early weeks of pregnancy. 5,6,12 On the other hand, although Progesterone levels increase throughout pregnancy, they are not considered a suitable means for monitoring fetal well-being during the third trimester.8 PRINCIPLES OF THE ASSAY The ANOGEN Coated well immunoenzymatic assay for the quantitative measurement of serum Progesterone utilizes a monoclonal Anti-Progesterone and a Progesterone-HRP conjugate. The assay sample and the assay buffer are incubated together with anti- Progesterone antibody coated plate for sixty minutes and washed. Then the diluted Progesterone-HRP conjugate is incubated. After the incubation period, the wells are decanted and washed three times.
The wells are then incubated with a substrate for the enzyme. The product of the enzyme- substrate reaction forms a blue colored complex. Finally a stopping solution is added to stop the reaction, which will turn the solution to yellow. The intensity of color is measured spectrophotometrically at 450 nm in a microplate reader. The intensity of the color is inversely proportional to the Progesterone concentration since Progesterone from sample and Progesterone-HRP conjugate compete for the Anti-Progesterone antibody binding sites. Since the number of sites is limited, as more sites are occupied by Progesterone from the sample, fewer sites are left to bind Progesterone-HRP conjugate. Standards of known Progesterone concentrations are run concurrently with the samples being assayed and a standard curve is plotted relating the intensity of the color optical density (O.D) to the concentration of Progesterone. The unknown Progesterone concentration in each sample is interpolated from this curve. LIMITATIONS OF THE PROCEDURE
1. Reliable and reproducible results will be obtained when the assay procedure is carried
out with a strict adherence to the exact procedure described within this package insert and good laboratory practice.
2. Progesterone determination is for diagnostic purposes. The Progesterone
concentration should be used only as an adjunct to other data (ex.: results of other tests, clinical impressions, etc.) available to the physician who can take into consideration the history of the patient. Each laboratory should compile its own normal ranges, if possible.
3. This kit is suitable for use with serum of human origin only. 4. A maximal total pipetting time of ten (10) minutes per run is suggested. Rev. (06/04) PROG-D REAGENTS PROVIDED All reagents provided are stored at 2-8°C. Refer to expiration date on the label. 96 tests
1. MICROTITER PLATE 96 wells
Pre-coated wells with anti-Progesterone Monoclonal Antibody immobilized into the well.
2. CONJUGATE (Part PNEL-2) 0.6 mL
Concentrated Progesterone-HRP conjugate in stabilizer solution.
3. ASSAY BUFFER (Part PNEL-3) 11 mL
Glycine buffer and 0.09% sodium azide as preservative.
4. STANDARD – 100 ng/L 0.5 mL
Prepared with human Progesterone in human serum containing 0.09% of sodium azide as preservative.
5. STANDARD – 50 ng/L 0.5 mL
Prepared with human Progesterone in human serum containing 0.09% of sodium azide as preservative.
6. STANDARD – 20 ng/L 0.5 mL
Prepared with human Progesterone in human serum containing 0.09% of sodium azide as preservative.
1. STANDARD – 5 ng/L (Part PNEL-7) 0.5 mL
Prepared with human Progesterone in human serum containing 0.09% of sodium azide as preservative.
7. STANDARD – 1 ng/L 0.5 mL
Prepared with human Progesterone in human serum containing 0.09% of sodium azide as preservative.
8. STANDARD – 0.25 ng/L 0.5 mL
Prepared with human Progesterone in human serum containing 0.09% of sodium azide as preservative.
9. STANDARD - 0 ng/L 1 mL
Prepared with human Progesterone in human serum containing 0.09% of sodium azide as preservative.
10. CONJUGATE DILUENT (Part PNEL-10) 11 mL
HEPES buffer pH 7.2 containing thimerosal as a preservative.
11. SUBSTRATE (Part PNEL-11) 11 mL
Buffered solution with TMB. 12. WASH BUFFER (Part 100 mL
Concentrated solution of saline phosphate buffer with thimerosal as a preservative. Dilute each bottle to one (1) liter with deionized or distilled water.
13. STOP SOLUTION (Part PNEL-13) 25 mL
0.5 M Sulfuric Acid (H2SO4). CAUTION:Caustic Material! WARNING: Sodium azide may react with lead and copper to form explosive azides. Flush with copious quantities of water. MATERIALS REQUIRED BUT NOT SUPPLIED 1. Precision pipettes (25 µL) with disposable tips or a SMI pipette 2. 8 channels pipette (50 and 100 µL) with disposable tips 3. Plate shaker (100 ± 10 rpm) 4. Microplate reader with filter 450 nm 5. 8 channels repeater pipette for the washing step or multichannel pipette 6. Deionized or distilled water 7. Absorbent paper PRECAUTIONS
1. All materials in this kit may be used only for in vitro clinical or laboratory tests not
involving internal or external administration of the material to human or animals.
2. The Standards contain products derived from human blood. Handle the materials as
though they were capable of transmitting infectious diseases, since no known test method can offer absolute assurance that such products will not transmit infectious agents even tested non-reactive.
3. Reagents are matched in each kit and therefore reagents from different lot numbers
should not be mixed. Do not use after the expiration date.
4. Optimal results will be obtained by strict adherence to this protocol. Respect
4. The kit containing sodium azide and thimerosal as preservatives. These are toxic and
therefore all reagents should be handled carefully to avoid ingestion or skin contact.
5. The stopping solution contains sulfuric acid. This solution should be handle with
6. Prior to assay, warm all reagents to ambient temperature by allowing them to stand at
room temperature. Gently mix all reagents.
Rev. (06/04) PROG-D REAGENT PREPARATION 1. Washing solution: dilute each bottle to 1 liter of deionized or distilled water. 2. Diluted PROGESTERONE-HRP conjugate: just before use, dilute the concentrated
Progesterone-HRP conjugate (EC-94051) with Conjugate Diluent (ED-94051) in the proportion of 1 volume of Progesterone-HRP in 20 volumes of Conjugate Diluent. (Dilution 1/21). Since the diluted Progesterone-HRP conjugate is not stable, prepare just enough for the required number of tests. Suggested volume of diluted Progesterone-HRP per number or wells:
Volume (mL) concentrated Volume (mL) Conjugate Progesterone-HRP
Discard unused portion of diluted Progesterone-HRP conjugate after completing the addition of the reagent to the wells. SAMPLE PREPARATION Serum must be used in this PROGESTERONE procedure. No additives or preservatives are necessary to maintain the integrity of the specimen. Store at 2-8°C and assay within one week after collection. If the assay cannot be performed within one week, freezing is recommended. ASSAY PROCEDURE
DO NOT INTERCHANGE REAGENTS BETWEEN KITS BEARING DIFFERENT LOT
ALL REAGENTS AND PATIENT SAMPLES SHOULD BE BROUGHT TO 22 ± 2°C
ALL REAGENTS AND PATIENT SAMPLES SHOULD BE MIXED BY SWIRLING OR
GENTLY VORTEXING. DO NOT INDUCE FOAMING.
Refer to the assay procedure, Table I 1. Pipette 25 µL of standard, control or patient sample into the corresponding wells. 2. Pipette 100 µL of the Assay Buffer into each wel . 3. Incubate for sixty (60) minutes on the plate shaker (100 ± 10 rpm) at room
4. Wash manually, precautions must be taken to avoid cross-contamination between
wells. Decant the well contents by inverting the plate over a container and without re-inverting, blot the plate against absorbing paper. Wash each well three times with 300 µL of washing solution. At the last wash, decant completely the washing solution by tapping the plate against absorbing paper until no trace of water is visible on the paper.
5. Pipette 100 µL of diluted Progesterone-HRP conjugate in each well. For the dilution
procedure see section VII, Reagent preparation.
6. Incubate for thirty (30) minutes on the plate shaker (100 ± 10 rpm) at room
7. Decant and wash the wells three times with 300 µL of washing solution as in step 4. 8. Pipette 100 µL of the TMB enzyme substrate solution to each well. 9. Incubate for twenty (20) minutes on the plate shaker (100 ± 10 rpm) at room
10. Add 50 µL of a stopping solution and shake the microplate to homogenize. 11. Measure the absorbance at 450 nm using a microplate reader NOTE: READ THE ABSORBANCES IMMEDIATELY AFTER COMPLETING THE ASSAY.
Wells Identification u
1. Incubate 60 minutes on the plate shaker (100 ± 10 rpm) at room temperature (22 ±
2. Wash 3 times (refer to the washing procedure) 3. Incubate 30 minutes on the plate shaker (100 ± 10 rpm) at room temperature (22 ±
4. Incubate 20 minutes on the plate shaker (100 ± 10 rpm) at room temperature (22 ±
CALCULATION OF RESULTS DO NOT ATTEMPT TO SUBSTITUTE ANY PART OF THIS SAMPLE DATA FOR YOUR OWN. Examine date for acceptance consistency with quality control guidelines. Aberrant values may be rejected. Refer to the sample data and calculations, Table II
For each standard, control and unknown sample, the optical density values are
On millimeter paper using the ordinate for the optical density (or the %B/B0) and the
abscissa for the standard concentrations (ng/mL), a smooth standard curve is plotted.
The values of the control and of unknown samples are read directly from the standard
TYPICAL DATA EXAMPLE Results of a typical standard run are shown below: OPTICAL DENSITY at 450 nm CONCENTRATION (ng/mL) EXAMPLE OF PROGESTERONE STANDARD CURVE Progesterone Concentration (ng/mL) PERFORMANCE CHARACTERISTICS 1. SENSITIVITY: The sensitivity of the assay, as defined by the amount of Progesterone
standard that will reduce the maximal binding (Bo = 100% of the Standard 0) by 5%, is 0.2 ng/mL.
2. PRECISION & REPRODUCIBILITY
a) Intra-assay variation: The precision of the assays was verified by assaying 10
replicates of 3 different sera. The results were:
Parameters
b) Inter-assay variation: Reproducibility of the protocol was established by assaying
3 different sera in replicates in successive runs. The results were:
Parameters
3. ACCURACY: Known amounts of Progesterone were added to a human serum sample
to determine recovery performance of the assay. The data obtained are below:
Expected value Observed value recovery
4. LINEARITY: 3 serum samples were diluted and run. The results were: Parameters
1/2 21.9 13.4 13.9 1/4 10.3 6.9 7.7 1/8 4.9 3.5 3.7
5. SPECIFICITY: Results are expressed as the ratio of Progesterone concentration to
the concentration of the cross- reactant.
CROSS-REACTANT % CROSS-REACTIVITY
6. CORRELATION STUDY: Clinical samples were analyzed by the ANOGEN
PROGESTERONE EIA kit in parallel with a similar method. The results of this study are as follows:
REGRESSION LINE FROM CORRELATION STUDY
6. EXPECTED NORMAL VALUES: It is recommended that, as with any assay, expected
values for given populations be determined by each laboratory over a suitable period of time and in a statistically significant number of assays before definitive clinical significance is attached to the results of the assay. However, the following may be used as a guide to preliminary interpretation.
Females: Follicular Phase Pregnant Females:
QUALITY CONTROL
Good laboratory practice requires that quality control specimens be run with each calibration curve to check the assay performance. Commercial controls are suitable. Any material used should be assayed repeatedly to establish mean values and acceptable ranges to assure proper performance. REFERENCES
1. Aufrere MB, Benson H. Progesterone: an overview and recent advances. J Pharm Sci
2. Bauman J. Basal body temperature: unreliable method of ovulation detection. Fertil
3. Brown JB. Timing of ovulation. Med J Austral 1977;2:780-3 4. Gautray JP et al. Clinical investigation of the mentrual cycle: clinical,endometrial and
endocrine aspects of luteal defect. Fertil Steril 1981;35:296-303
5. Hensleigh PA, Fainstat T. Corpus luteum dysfunction: serum progesterone levels in
diagnostis and assessment of therapy for recurrent and threatened abortion. Fertil Steril 1979;32:396-9
6. Hernandez Horta JL, et al Direct evidence of luteal insufficiency in women with
habitual abortion. Obstet Gynecol 1977;49:705-8
7. Jones G. luteal phase defects. In: Behrman SJ, Kistner RW, editors. Progress in
infertility. Boston: Little, Brown and company. 2nd ed, 1975:299-324
8. Klopper A, Fuchs F. Progestagens. In: Fuchs F, Klopper A, editors. Endocrinology of
Pregnancy. Hagerstown: Harper&Row, 1977:99-122
9. March CM. Goebelsmann U, Nakamura RM, Mishell DR. Roles of estradiol and
progesterone in eliciting the midcycle luteinizing hormone and follicle-stimulating hormone surges. J Clin Endocrinol Metab 1979;49:507-13
Progesterone, A BIO-ED TM slide/seminar educational program. Rochester: Bioeducational Publications, 1981
11. Radwanska E, et al. Plasma progesterone and oestradiol estimations in the diagnostis
and treatment of luteal insufficiency in menstruating infertile women. Acta Eur Fertil 1976;7:39-47
12. Radwanska E, et al. Plasma progesterone levels in normal and abnormal early human
pregnancy. Fertil Steril 1978;30:398-402
13. Radwanska E, et al. Single midluteal, progesterone assay in the management of
ovulatory infertility. J Reprod Med 1981;26:85-9
14. Sheehan KL, Casper RF, Yen SSC. Luteal phase defects induced by an antagonist of
luteinizing hormone-releasing factor: a model for fertility control. Science 1982;215:170-2
15. Wentz A. Pathophysiology of luteal phase inadequacy. In: Tozzini RI, Reeves G,
Pineda RL, editors. Endocrine Physiopathology of the ovary. Amsterdam: Elsevier/North Holland, 1980:257-74
16. March CM. Luteal phase defects. In: Mishell DR, Davajan V, editors. Reproductive
Endocrinology, Infertility and Contraception. Philadelphia: F.A. Davis Company, 1979:469-76
17. Abraham GE. The application of natural steroid radioimmunoassay to gynecologic
endocrinology. In: Abraham GE, editor. Radioassay Systems in Clinical Endocrinology. Basel: Marcel Dekker, 1981:475-529
A Holistic Approach to TMJ Utilizing Advanced Therapeutic Massage Techniques Nutritional Therapy, and Emotional Release Processes Understanding that TMJ (temporo-mandibular joint) pain and associated problems make it difficult if not impossible to identify the exact nature of the cause of the problem. We have approached TMJ with the attitude that we cannot fix everyone, but can contribut
Próftafla og lesefni – 5. bekkir Maí 2007 Sum próf eru á skólatíma og eru hluti af venjulegum skóladegi. Tímasetning þeirra er breytileg milli bekkja og mun umsjónarkennari hvers bekkjar láta nemendur vita um tímasetningu þeirra. Sérstakir prófadagar eru 22. – 24. maí og eru tvö próf hvorn daginn með stuttu hléi á milli. Kennsla fellur niður þá daga og n
 Progesterone ELISA Kit
Progesterone ELISA Kit 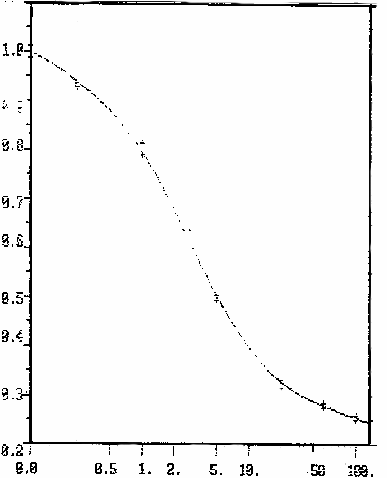 EXAMPLE OF PROGESTERONE STANDARD CURVE
EXAMPLE OF PROGESTERONE STANDARD CURVE 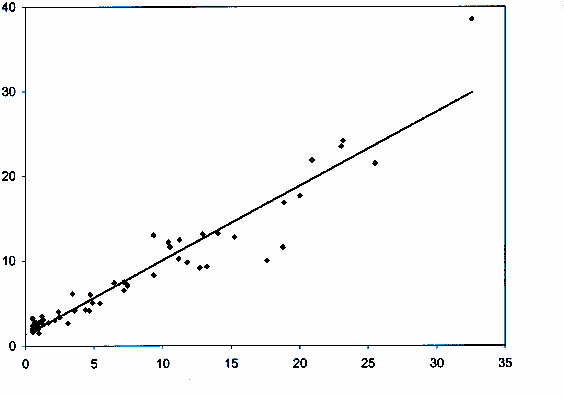 6. CORRELATION STUDY: Clinical samples were analyzed by the ANOGEN
6. CORRELATION STUDY: Clinical samples were analyzed by the ANOGEN