Thank you, it's cool. Used for the first time because only then was the right drug. Very revealing detail: ordered Express shipping to get the order within 3 hours because didn't know how to get the order faster https://africarx.co.za/ The drug is authentic exactly. Consistent with the stated prices the Staff is knowledgeable.
Microsoft powerpoint - warfarin poster presentation 2013 (3).ppt [compatibility mode]
Warfarin Safety for Residents in Skilled Nursing Facilities Principal Investigator: Darren Triller, Pharm D, Senior Director, Health Care Quality Improvement IPRO Project Director: Karen Morris, RN, MS Director Clinical and Quality Services NYSHFA/FQC Background Data Collection Intervention #1 – Policy and Procedure Review
As many as 12% of the 1.6 million American nursing home residents receive long term oral anticoagulant therapy with warfarin to prevent strokes and other thromboembolic events. Warfarin is among the medications most frequently associated with emergency department visits, hospitalizations and death, and, unfortunately, the quality of warfarin management in the LTC setting has been shown to be suboptimal. Previous research estimates that there may be as many as 34,000 fatal, life-threatening, or serious adverse warfarin-related adverse events annually, and that the majority of the most serious events are preventable. Nursing home residents on warfarin that are co-prescribed antibiotics are at even higher risk for adverse events. Given the incidence of residents in American long term care (LTC) facilities receiving warfarin, the safe and effective utilization of anticoagulants in the long term care setting is ofparamount importance. Despite the high level of resident oversight afforded by LTC facilities, high quality warfarin management continues to prove elusive. Mandated features of LTC services such as control of patient diet and medication administration, routine skilled nursing assessment, and mandated monthly drug regimen reviews, have proven insufficient to provide the levels of safety and INR control achieved in other settings. Likewise, interventions designed to improve nurse-physician communication relating to warfarin management have not demonstrated the ability to significantly reduce preventable adverse events.
The primary objective of this study is to document and improve the proportion of anticoagulated patients receiving INR testing within 3-7 days of a warfarin-antibiotic interaction “event” (i.e. receiving warfarin and prescribed interacting antibiotic). Secondary measures of interest will also be evaluated to assess the impact of the intervention components on quality of warfarin management and actual patient outcomes for patients prescribed antibiotics and the overall warfarin population. Such measures include: proportion of warfarin users receiving monthly INR, time in therapeutic range, INR excursions (<1.5 or >5.0), mean INR, and adverse events relating to anticoagulation or underlying indications for anticoagulation (eg. emergency department visits, overall, bleeding, thromboembolism). The solution summary will demonstrate that a multifaceted intervention will improve quality of care while providing insight into benefits/impact of
Intervention #2 – Fax Notification Intervention #3 - Education
individual intervention components. The study will test the hypothesis that a multidisciplinary intervention consisting of real time pharmacist intervention, administrative involvement, and nurse education will improve the frequency of therapeutic monitoring of anticoagulated patients prescribed interacting antibiotics.
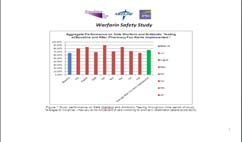
The study setting was skilled nursing facilities in New York State. To maximize participation and compliance with the interventions, FQC identified long term care facilities that are affiliated with NYSHFA, its affiliated membership association of more than 270 skilled nursing facilities. Those selected were part of corporate entities (multi-facilities), who utilized a pharmacy distributor that is not Omnicare (who had participated in a pilot project), and were located in multiple geographic regions of New York State. While all facilities were known to maintain relevant policies and procedures (and some may reflect current anticoagulation best practices), published studies and data from the previous IPRO pilot demonstrated that, in general, LTC facilities do not yet provide optimal anticoagulation management to their residents. To identify which intervention components are best able to improve anticoagulation control and minimize preventable adverse drug events, additional data and analysis appeared necessary. A full package of interventions was rolled out over the course of the study. The first intervention/independent variable was a pharmacy alert system begun in month two. In the fifth month a policy and procedure review for safe warfarin therapy was added that occurred monthly in QI meetings. By the eighth month, physicians, licensed nurses and quality improvement staff participated in in-service reviews on safe warfarin therapy. Each of these interventions was tested separately for the degree of effectiveness compared to the retrospective analysis and the month of baseline data. The baseline data served as the reference for this test. In addition we compared the effect of all three interventions together against the baseline data. Outcome Measures
The primary purpose of this study was to increase the proportion of anticoagulated patients receiving INR testing within 3-7 days of a warfarin-antibiotic interaction “event” (i.e. receiving warfarin and prescribed interacting antibiotic). Such events
have been associated with INR elevation and adverse events, and have been included as a component of a quality measure endorsed by the National Quality Forum. Resident level inclusion into the analysis was defined by experiencing such an event. A resident may be entered in the analysis more than once, as an antibiotic may be prescribed more than
Conclusions
once during the study period. Events will be categorized as a dichotomous “yes/no” variable based on existence or absence of an INR result within the 3-7 day time interval. Secondary measures of interest were also evaluated to assess the impact of the intervention components on quality of warfarin management and actual patient outcomes. Time in
Although a significant improvement in the primary outcome measure was achieved, the study did not
therapeutic range (TTR) was evaluated (Rosendaal method) for the patient population exposed to antibiotic “events”, as it is possible that the intervention may result in improved overall control among such patients. Likewise, TTR was calculated
demonstrate improvement in important secondary measures. The slight improvement in time in therapeutic
across warfarin patients not exposed to antibiotics, as it is possible that components of the intervention (e.g. improved
range was not statistically significant, nor was there a significant reduction in extremely elevated lab results
policies, nurse education) “spilled over” and affected care of patients beyond the exposure to interacting antibiotics. The
that may be associated with avoidable bleeding events. The frequency of laboratory testing in the long term
study also quantified and evaluated the frequency of INR “excursions” (i.e. INR <1.2 or >5), as extreme INR values have
care facilities far exceeded the norm for other outpatient settings (avg. 6 days vs. standard 30 days). But
been associated with dramatic increases in risk of bleeding and thromboembolic events. Finally, the study attempted to
this potentially excessive vigilance was not associated with improved quality of care, further indicating the
assess the impact of the intervention on rates of actual clinical events using data available through participant homes and
need for improved processes to guide drug dosing. Further study and initiation of best practices related to
IPRO. Events such as emergency department visits and hospitalizations for bleeding or thromboembolism were of
particular interest, and were quantified and reported in detail regardless of sample size or statistical significance.
Veterinaria, Anno 15, n. 1, Febbraio 2001 EFFICACIA DELLA CLOREXIDINA DIGLUCONATO SHAMPOO AL 2% E SOLUZIONE ALLO 0,45% NELLE PIODERMITI DI SUPERFICIE E SUPERFICIALI DEL CANE S. COLOMBO, L. CORNEGLIANI*, G. GHIBAUDO** Istituto di Patologia Speciale e Clinica Medica Veterinaria - Facoltà di Medicina Veterinaria di Milano * Libero Professionista - Via Mario Borsa 63/163 I-20151
Samedi 21 /11/2009 Intitulé 8h30 à 9h30 Introduction à la cérébrolésion Delire Ralph Kinésithérapeute Réflexions autour des techniques passives, actives, 9h30 à 10h30 10h45 à 11h 45 Marie –Dominique Gazagnes Reconnaître, prévenir, traiter voire guérir de l’AVC Neurologue- Médecin réadaptateur 11h 45 à 12h45 12h 45 à 13h45 R e





















 Warfarin Safety for Residents in Skilled Nursing Facilities
Warfarin Safety for Residents in Skilled Nursing Facilities