Ordered, immediately called back and the same day delivered the order.Very pleased with the work. Thank you for prompt and accurate work https://africarx.co.za/buy-cialis-south-africa.html great prices, delivered on the day of the order. Pleasant managers consult by phone.
Ecp28_3 inside_ecp28_3 inside
Living psychology: The ‘emotional warmth’ dimension of professional childcare Children and young people in public care are arguably the most vulnerable group in our society and, despiteconsiderable support and financial expenditure, the outcomes for these children have remained stubbornlypoor. While the worthy intentions of government initiatives over recent years are not in question, it is clearthat there is a need for a new theory-led, evidence-based model of professional care and support. This paperpresents a psychological perspective which links early childhood experiences with restricted life outcomes. It argues that it is parental rejection (sometimes accompanied by abuse and neglect) which is a majormediating factor in the often-restricted life outcomes for many of these children.The ‘emotional warmth’ approach to professional childcare enables a visiting applied psychologist toempower residential and foster carers to provide high quality parenting, sensitive support for post-traumastress and a deeper understanding of the (often hidden) signature strengths of these children and youngpeople. The inclusion of these three components in a support plan is likely to promote positive emotional,social and academic development of children in public care. The major role of the applied psychologistconsultant in the emotional warmth model is discussed and appropriate outcome measures for thisapproach of childcare are considered.‘Foster and residential care is a complex activity.’ (National Institute for Health and Clinical Excellence/Social Care Institute for Excellence, 2010, p.9)
‘We believe that the greatest gains in reforming our care system are to be made in identifying and removingwhatever barriers are obstructing the development of good personal relationships, and putting in place allpossible means of supporting such relationships where they occur.’ (House of Commons, 2009, p.27,para. 29)
THEemotional, social and academic prob- There has been no shortage of recom-
mendations for helping these children and
papers about educational psychologists’ work
with, or related to, such children. Reviewing
2009) which noted the potential of ‘social
the literature on children in residential care,
Nissim (2006) concluded: ‘the youngsters
Germany, a model which was later endorsed
concerned are among some of the most disadvan-
in the joint NICE-SCIE (2010) report. taged, damaged and vulnerable members of our
However, consistently positive outcomes for a
society, and their needs are extreme and complex’
variety of interventions have so far proved to
(p.275). In a similar vein, for foster care,
Guishard-Pine et al. (2007) have stated that
have pointed out in their review of education-
‘many children within the foster care system are at
based interventions and their disappointingly
significant risk of mental health problems because of
small impact on the attainments of pupils
their history of harsh treatment and neglect’ (p.79).
who are in public care. While official statis-
Educational & Child Psychology Vol. 28 No. 3 The British Psychological Society, 2011Living psychology: The ‘emotional warmth’ dimension of professional childcare
tics, like those released for England and
client group. Exemplars here would include
early intervention, child-focused initiatives
like school-based nurture groups designed
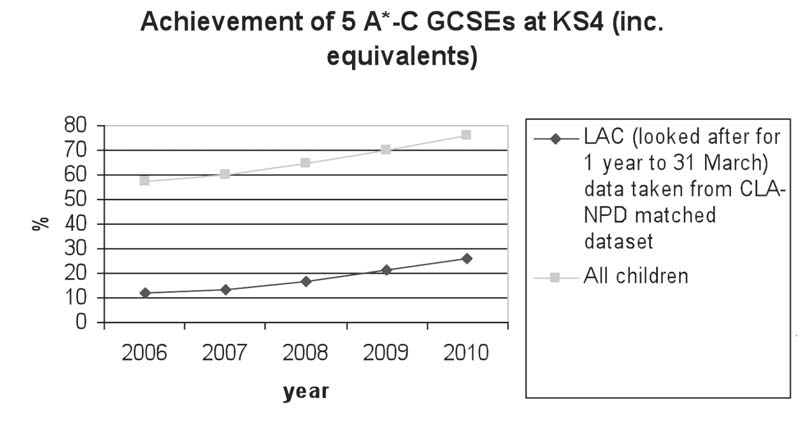
GCSEs at Key Stage 4 it has not been possible
2010), parent and teacher activities to build
to attribute this improvement to any partic-
up the resilience of these children (Dent &
ular intervention, since similar gains have
occurred in the general school population.
Guidance initiative which enables parents to
attune more closely to the needs of their
children in care and those in the general
child (Kennedy, Landor & Todd, 2010a,
population of their peers has remained the
outcomes which they experience, a wider
imperative when set against the emotional
intervention perspective is clearly needed. Such
cost to the children and young people them-
selves (and to society at large) since far too
who have had negative, early life experi-
ences, the carefully planned and specifically-
less, jobless, friendless and deeply unhappy.
post-trauma stress and enable them to grow
claimed success for specifically-targeted
and develop personally and socially, as well
approaches designed to help this vulnerable
Figure 1: Outcomes for children looked after by Local Authorities in England and Wales matched with data contained within the National Pupil Database. Educational & Child Psychology Vol. 28 No. 3R.J. (Seán) Cameron & Colin MaginnEmotional warmth: A wider view? ‘…rejection is not simply one misfortune
Explanations as to why looked-after children
among many, nor just a bit of sad drama – it
fail to develop emotionally, socially and
strikes at the heart of what the psyche is
academically have often focused on what is
designed for.’ (Baumeister, 2005, p.732)
quality care and schools which neglect to
address their educational needs (see Jackson
specific form of positive response – accept-
& Martin, 1998, and Jackson & McParlin,
ance – from parents and other primary care
debate the merits of such explanations, their
2004, 2005). When this need is not satisfacto-
rily met, children worldwide and regardless
concerned and for the allocation of scarce
ethnicity or other such defining factors, tend
Secretary of State for Education, clearly
aggressive, dependent or defensively inde-
perceived the public care system as failing its
pendent, impaired in their self-esteem and
children: ‘it is inexcusable and shameful that thecare system seems all too often to reinforce this early
mostly unstable and holding a negative view
disadvantage’ (Department for Education
of the world that they live in (Rohner et al.,
and Skills, 2006, p.3). Since the publication
2004). The main features of the PA-RT are
research has supported the PA-RT explana-
initiatives (for example, ‘virtual head
tion (see Rohner, 2004; Rohner et al., 2004,
teachers’ for looked after children) in an
investigations in this area) but the implica-
tions of this work seem to have been over-
As an alternative theoretical explanation
looked or ignored in UK policy making and
for the pain-based behaviour and poor life
planning for children who have experienced
rejection by their parents in one form or
authors of this paper have argued that it is
‘rejection’ in general and ‘parental rejec-
tion’ in particular (rather than failing care
presents a challenge to the uncritically-
and education systems exclusively) that are
accepted, current view that their poor educa-
the most significant contributors to the flat-
tened life trajectories of these young people
(Cameron & Maginn, 2005, 2008). The back-
ground to such a claim is discussed in the
restricting, emotionally-damaging or self-
worth reducing effects of the care andeducation systems. Instead, they have their
Parental Acceptance-Rejection Theory
roots in the quality of the affection bond
have been long aware of the negative effects
of psychological abuse, rejection and exclu-
sion on individuals or group members, it is
only relatively recently that satisfactory
For applied psychology practitioners, one
explanations of the accompanying negative
important and illuminative aspect of PA-RT
is the finding that parental rejection doesnot only consist of a specific set of overtly
Educational & Child Psychology Vol. 28 No. 3Living psychology: The ‘emotional warmth’ dimension of professional childcareFigure 2: A summary of the main components of Parental Acceptance-Rejection Theory (Rohner, 1986, 2004). Main themes from Parent Acceptance–Rejection Theory:● Children and young people need parental acceptance, not rejection. ● If the child or young person’s need for acceptance is not met, emotional problems result. ● Such emotional problems appear to be universal, across the human race. ● Rejection can be clearly evident or the child can perceive rejection: both types of rejection
can generate emotional difficulties in the child or young person.
● Many of these emotional problems result in dysfunctional and self-defeating behaviour which
● Other factors are involved in the adjustment of children, but parental acceptance-rejection
has been shown to be a particularly powerful mediating factor between early experiences andlater emotional development.
ical pain and the pain of rejection (DeWall et
al., 2010). They found that acetaminophen
beliefs that are held by the child or young
reduced neural responses to rejection. In
short, paracetamol did lessen the pain of
perceive significant rejection are likely to
feel ever-increasing anger, resentment and
neurological link between social pain and
other destructive emotions that may become
survival of the species depends on the bond
convincing explanation for the detrimental
between infant and carer. The ‘Dynamic-
effects of ‘parental rejection’ on educational
Maturational Model’ of attachment (Crit-
and life outcomes of looked after children.
tenden & Dallos, 2009) offers an optimistic
that ‘physiological processes responsible for detec-tion and regulation of physical pain were co-opted
respond positively to sensitive and respon-
to sense and respond to emotionally painful events,such as being rejected or excluded’ (p.3). They list
‘healing’ attachments with committed caring
studies that report decreased sensitivity to
physical pain following separation from care-
givers among rat pups, young mice, calves
experiences, such as parental rejection, to
Physical evidence that social pain piggy-
backs on those areas of the brain which react
to physical pain is provided in neurological
world together with the pain and distress
experienced by children in public care and
pose for carers and their support profes-
physical pain and social rejection arguing
that ‘for both caregiver and infant to feel painupon separation ensures social connection and
ture is the absence of specific implications
thus offspring survival’ (p. 891). DeWall and
for promoting parent acceptance behaviour
his colleagues carried out a series of experi-
and avoiding passive, negative or uninten-
ments to test the connection between phys-
tional parental rejection. Rohner (2004) and
Educational & Child Psychology Vol. 28 No. 3R.J. (Seán) Cameron & Colin Maginn
Rohner et al. (2004) do, however, offer two
1. The Pillars of Parenting. A procedure
general principles of parenting derived from
● Helping parents and other caregivers to
young people through the eight Pillars of
communicate acceptance to children.
culturally-appropriate ways to avoidbehaviours that indicate parental coldness and
2. Adaptive emotional development. A system
which empowers carers to supportchildren and young people in their
Emotional warmth and professional childcare
The starting point of the ‘emotional warmth’
model of professional childcare described in
this paper is the importance of the relation-
ship between each individual young person
and their carer. A new priority becomes the
empowering of residential and foster carers
3. Signature strengths. A strategy for teaching
with the knowledge and skills to understand
and respond appropriately to the emotional,
behavioural and attainment difficulties that
are exhibited by the children in their care.
utilise these effectively in their everyday
4. Living psychology through consultation.
access to the knowledge base of psychology
through regular child focused consultations
applied psychologists to provide on-going
with a qualified and experienced consultant
advice and support for residential/foster
psychologist. Second, in support of the on-
the-spot learning which takes place in the
consultation sessions, the continuing profes-
employing the emotional warmth model.
sional development of the caregivers is then
The individual action plan for each child,
supported by a programme of training in the
which results from these group consultation
sessions, lists activities which carers and
warmth’ model. This programme (which can
lead to a formal qualification) covers attach-
intend to carry out to meet the child’s
ment theory, authoritative parenting, adap-
parenting needs, support the child though
tive emotional development, the effective
strengths. Therefore, the emotional warmth
strengths, involving young people in deci-
approach is designed to bring about positive
child and carer’s progress and development.
fulfilling lives and to avoid the fate of too
warmth’ approach to professional childcare
many children in care: homeless, jobless,
and the psychological theory and research
friendless and incarcerated. In the case of
which underpin this approach can be found
the latter outcome, it is estimated that over a
quarter of the prison population have been
in care (Social Exclusion Unit, 2002). Educational & Child Psychology Vol. 28 No. 3Living psychology: The ‘emotional warmth’ dimension of professional childcareThe Pillars of Parenting
parents and foster ‘parents’ to identify and
Words shape the way we see the world, and
agree what ‘good parents’ should do.
completely as ‘parenting.’ Children in care
have often been disadvantaged by the termi-
nology used. ‘Looked after’ implies a passive
dependent on the needs of each individual
receiving of some ‘looking after’ behaviour
child at any given time. The child is the
by adults, while ‘caring’ is devoid of the
viewed as a set of tools to provide a trans-
which comes with the ‘parenting’ process.
parent structure for everyone working with
the child. While the eight pillars are not hier-
‘parenting’ for particularly vulnerable
archical, and individual pillars may some-
times overlap to some extent, their structure
the skills and knowledge of parenting cannot
is designed to help caregivers, who are often
be left to trial and error, but need to be
unpacked, analysed, understood and imple-
Vocational Qualification Level 3 in England,
mented so that even in challenging circum-
Wales or Northern Ireland (Qualifications
stances, the ‘professional parents’ will know
equivalent elsewhere, to make sense of the
consultant, carers can select one pillar (occa-
people in their care and to agree purposeful
sionally two) which is particularly relevant to
the parenting needs of the child or young
person at that point in time. For each of the
eight pillars, there is a menu of parenting
together with a sample of carer activities
activities, from which the group of carers can
which could support each pillar, while Figure
choose and discuss and agree the two or three
3 contains an extract from the action plan
activities which are the most appropriate for
for ‘Renae’ whose behaviour can often be
supporting the child or young person in the
thoughtless, random and (unintentionally)
previously selected pillar. In the case of a
dangerous for children and carers alike.
children’s home, all the carers would agree tocarry out these selected support activities
Adaptive emotional development
A simplified and carer-friendly description of
themselves, while foster carers would involve
a child’s emotional journey through devel-
other family members in these activities.
theory and research, the Pillars of Parenting
extended in the ‘emotional warmth’ model
are closely linked with many of the specific
to include the type of support and manage-
outcomes of the Every Child Matters outcomes
ment required by traumatised children and
Skills, 2005), especially in the areas of
are attempting to make sense of, or find ways
mental and emotional health, personal and
of living with, the traumatic events which
have occurred in their lives. (See Table 2 for
an overview of the three phases of the Cairns
significant life changes and challenges.
The selection of each of the eight ‘pillars’
carer activities which can support children
Educational & Child Psychology Vol. 28 No. 3R.J. (Seán) Cameron & Colin MaginnTable 1: A summary of the Pillars of Parenting and some of the staff behaviours and tasks which support these. Seán Cameron & Colin Maginn (2008) Primary care and Making close Positive self- Emotional protection relationships perception competence Why? See Ziegenhain Why? For more Why? A useful Why? See Maslow Examples of support required from Examples of support care staff required from care staff Examples of support Examples of support required from required from care staff care staff Educational & Child Psychology Vol. 28 No. 3Living psychology: The ‘emotional warmth’ dimension of professional childcareSelf-management Resilience A sense of belonging Personal and social
● Resilient individuals ● Research and
responsibility Why? For details of Why? See Lewis and Why? Personal social Why? See Dent and Examples of support required from care staff Examples of support required from care staff Examples of support required from care staff Examples of support required from care staff
recognise ‘stranger danger’ from helpful adult behaviour. Educational & Child Psychology Vol. 28 No. 3R.J. (Seán) Cameron & Colin MaginnFigure 3: Case example. Meeting ‘Renae’s’ parenting needs through the Pillars of Parenting.
The pillar which was chosen as a priority for Renae at this point was Pillar No 8: Developingpersonal and social responsibility. Selected support for 13-year-old Renae would involve theresidential carers in the following:● Encouraging Renae to ‘assume positive intent’ for the behaviour of her carers, their friends
and the other children in this home (rather than negative intentions).
● Discussing the importance of different types of relationships (e.g. work, leisure, sexual, etc.)
and how to make relationships with peers that will last.
● Helping Renae to think about her future aspirations. ● Teaching Renae the concept of ‘building up social capital’ – for example, doing something for
a friend or a member of the foster family, helping someone in need, or ‘showing willing’: all these without expecting immediate reward.
It is worth noting here that the selected pillar of parenting and the accompanying supportactivities chosen by carers are likely to change over time as Renae’s needs evolve and herresilience and emotional adjustment increase (or decrease). Table 2: A summary of the Cairns model of trauma and loss, together with some good practice suggestions at each phase. (Adapted from Cairns, 2002.) Stabilisation Integration Adaptation Some examples of good practice suggested by carers Educational & Child Psychology Vol. 28 No. 3Living psychology: The ‘emotional warmth’ dimension of professional childcare
Of course, some highly resilient children
young person moving through their current
emotional phase. In Box 1 there is an extract
adversity in their individual ways, but most
from an action plan drawn up for 13-year-old
children in care are likely to require sensitive
‘Renae’ who as well as exhibiting self-
support from carers to begin the emotionally
demanding task of modifying the impact of
overview of post-trauma stress is particularly
useful since it can help residential and foster
phase of the Cairns model, together with the
carers to view a child’s often-disruptive
accompanying staff support activities, are
likely to change over time as Renae’s needs
evolve and her adaptive development grows.
lish a safe and stable environment where the
child is able to talk about and learn more
and encouraging them to form healthy rela-
tionships with the young people in their care
trauma (stabilisation), to deal with the often-
has an important role to play in the ‘healing’
conflicting feelings which accompany such
information, to process, control and manage
‘Most of the therapeutic experiences do not take
any resulting psychological or physiological
place in ‘Therapy’ but in naturally occurring
reactions (integration) and, finally, to support
healthy relationships. The most effective
the child in re-establishing social connected-
treatments to help child trauma victims is
ness, developing personal efficacy, achieving
anything that increases the quality and
a satisfactory level of emotional adjustment
number of relationships in the child’s life.’
to the negative events which have been expe-
view of the future (adaptation).
sense of the young person’s journey through
provides carers and consultants with a menu
of post-trauma stress activities from which
psychologist’s role is to bring a wider and
carers can determine the specific phase that
deeper understanding of the trauma process
and to use clinical skills to pick up on any
atypical trajectories in the young person’s
two or three activities which will provide the
most appropriate support for the child or
Box 1: Case example. Supporting ‘Renae’ through post-trauma stress with the adaptive emotional development component of the ‘emotional warmth’ model. The residential carers felt that Renae’s adaptive emotional development needs currently lay between the Stabilisation and Integration phases of Cairns’s model. Key activities for all carers were discussed and agreed as follows: ● Reassuring Renae that all the carers in her children’s home were friendly, kind and good at
listening to children’s worries as well as their happy stories.
● Establishing a closer relationship between Renae and all the carers, but especially her
● Trying to understand the source of Renae’s current unhappy and withdrawn behaviour. Educational & Child Psychology Vol. 28 No. 3R.J. (Seán) Cameron & Colin MaginnSignature strengths
strengths can be employed in everyday life.
Seligman (2002) believes that each person
In the case of a looked after child, the uncov-
possesses several signature strengths. These
ering and utilisation tasks could be carried
are strengths of character that a person self-
out most effectively in a discussion between a
consciously owns, celebrates and, if possible,
incorporates into daily contexts, such as
person, and then shared with other carers,
school, work, relaxation activities, relation-
teaching colleagues or family members.
ships and hobbies. Focusing on the signature
These significant adults in the life of a child
or character strengths of children and young
in care would then use this information to
provide opportunities (or would look out for
and energy for everyone involved. In partic-
appropriate windows of opportunity) which
ular, it can shift carers’ perceptions of a young
allow the child or young person to employ
person from ‘problems’ to ‘possibilities’.
A list of signature strengths (which might
include a love of learning, a sense of fairness,
the ability to use humour in everyday life andenthusiasm) can be found in Seligman
Living psychology through consultation
(2002) or Linley (2010), but some of the less
obvious ones, which may apply particularly
‘emotional warmth’ model is the everyday
contribution of those residential or foster
● Curiosity and interest in the world. Curious
children and young people. Monitoring and
themselves, the world they live in and the
training and professional development, all
● Practical thinking. This strength often
quality care. Responding to a child whose
behaviour can be perceived as deliberately
frequently reject or exploit acts of kindness,
● Courage. Included here are both moral
considerable conviction as well as informed
(asking for help with one’s own fears and
side, tackling the challenges of providing
emotionally warm caring in their encounters
● Discretion. An important strength which
with difficult and rejecting children, of
tuously that might be regretted later on.
trauma stress process and of enabling them
● Gratitude. This involves being aware of
strengths effectively, all demand that resi-
dential and foster carers require a combina-
● A sense of purpose. Developing ambitious,
informed professional expertise. While these
but achievable, aspirations for the future
direct contact carers have amassed detailed
knowledge about the children in their care,
After the signature strengths of a child or
it is an ‘indirect contact’ or consultant
psychologist who is able to draw upon the
knowledge base of psychology, and who can
provide carers with the much needed insight
Educational & Child Psychology Vol. 28 No. 3Living psychology: The ‘emotional warmth’ dimension of professional childcareTable 4: Case example: Building on ‘Renae’s’ signature strengths to promote personal and inter-personal competence.
Renae has two big signature strengths – humour (there are times when she is unhappy when shebecomes withdrawn and non-communicative, but she is also able to make people laugh) andcreativity (she can sketch, enjoys street dance and is good at gymnastics). Possible activities which carers agreed would allow Renae to use these strengths more effectivelywere as follows: ● Build in a few ‘sketch sessions’ with Anwar (a social work student on placement in the home)
● After supper on Friday, staff member would introduce ‘Renae’s stand-up comedy time’ and
invite her to start off a series of jokes told by the children and staff.
● Provide opportunities for Renae to display some of her finished drawings publically. ● Investigating the possibility of helping Renae to join and settle into a local dance club or a
into children’s complex problems, offer
in the case of the children’s home, selected
sections and actions from the consultation
discussion of the sophisticated strategies
notes are then transferred into the care plan
required to help children and young people
for the particular child or young person. By
to deal with problems resulting from rejec-
way of illustration, through this process
‘Renae’s’ parenting needs (Figure 3),
In their review of consultation effective-
support for post-trauma stress (Box 1) and
personal/social development (Table 4) are
‘well-constructed models (of consultation),
all addressed. In short, this is an integrated
articulated from sound theoretical bases may
approach to supporting ‘Renae’ in all major
be superior to those without clear concep-
tual frameworks’ (p.349). In this regard, the
specific tasks of the applied psychologist in a
sents a different approach to the more tradi-
residential or foster care group consultation
The total time involved in a group consul-
carers to support the child or young person.
tation session focusing on one child or young
The goal of group consultation is to enable
the carers themselves to provide support for
hours. At the end of the consultation session,
and management of problems in the context
the psychologist consultant produces notes of
in which the child or young person is having
each session. These contain a clear descrip-
difficulties (see Dent & Golding, 2006 for a
tion of the agreed management strategy for
discussion of this issue). Residential and
self-defeating behaviour, the activities agreed
foster carers are ideally placed to carry out
by staff for supporting the chosen pillar of
such context-based work since opportunities
parenting, the agreed strategy for supporting
the adaptive emotional development of the
through the sensitive management of those
child and a list of activities which will enable
the child or young person to utilise signature
strengths more effectively in everyday life.
These notes are distributed to all the residen-
tial or foster carers who have taken part and,
Educational & Child Psychology Vol. 28 No. 3R.J. (Seán) Cameron & Colin MaginnTable 5: Protocol for a group consultation session involving an applied psychologist and residential team or foster carers’ group.
1. Discussion of big and modest successes achieved by staff since the last consultation session. 2. Update on agreed actions and outcomes for child or young person discussed at previous
3. Discussion of the behaviour management problems of today’s child or young person,
as follows:● A pen portrait of the child or young person by the foster carer or key worker. ● A thumbnail outline of the child’s self-defeating behaviour(s). ● Discussion of the Antecedent (A), (Background) (B), Consequences (C) and
(Communication*) (+C) factors surrounding the problem.
● Consideration of how to change the key A, B and C factors and how to teach functional
+C skills (see Cameron and Maginn, 2009 for an account of the ABC+C approach to behaviour management).
● Agreed action strategies for management and support. ● A plan for implementing, monitoring and evaluating the agreed action by carers. ● A written and shared summary of agreed action, provided by the psychologist consultant.
4. Discussion and identification of the child’s current parenting needs (using the Pillars of
Parenting list and selecting from the staff support activities menu).
5. Identification and discussion of the child’s post-trauma emotional needs (using the Adaptive
Emotional Development model and selecting from the menu of staff support activities).
6. Discussion of child’s assets and talents and consideration of the learning opportunities that
7. Meta-analysis of the session. Discussion of the process of the consultation process and
consideration of its usefulness and possible areas for improvement. * The Communication factor in point 3 relates to the question, ‘What is the child trying tocommunicate through behaviour?’ Possible messages here might include: revenge, or a need toescape from an uncomfortable situation, or immediate attention, or other reasons. (See Dreikurset al., 1982, for details of this important factor in understanding and managing self-defeatingbehaviour.)Measuring changes in vulnerable children
and self-defeating behaviour, a reduction (or
a rise) in overt self-harming behaviour and
applied psychologists can inform (and some-
absconding, or a reduction or increase in the
times challenge) carers by drawing on infor-
reported frequency of intrusive thoughts,
mation from psychology theory and research
sleep patterns or night terrors. Records of
to improve child care practice: they can also
such gross behaviour changes are important.
enable carers to make changes to existing
practice by evaluating the outcomes of their
inform carers why these events are occurring
efforts for the children and young people in
and, equally important, what they are doing
Of course, there are ‘hard data’ indica-
emotional development and resilience.
tors of change and these can include: any
attempting to measure pre- and post-inter-
ment levels, an increase (or decrease) in the
vention changes in a child’s life, including
number of incidents of unwanted, anti-social
external global measures such as improve-
Educational & Child Psychology Vol. 28 No. 3Living psychology: The ‘emotional warmth’ dimension of professional childcare
behaviour or increases in cognitive ability/
IQ. The problem with general measures like
these is that the answer to why the interven-
effects of negative early life experiences.
tion led to the changes which occurred canoften only be speculated upon. While such
Bespoke measures
gross measures are important, they tend to
oversimplify or ignore the complexity of the
should not only provide feedback to carers on
problems of children and young people who
the results of their efforts, but should also
have been rejected, neglected and abused.
permit external validation of the success of
employed to record the way in which looked
commissioners might be satisfied with infor-
recorded serious incidents, more sensitive
measures are required to plot the process ofchange in children over a longer period. For
Standardised measures
this reason, the ‘cobweb diagram’ was created
both to measure and illustrate the child’s or
Children (Briere, 1996) has been chosen to
young person’s response to positive parenting
and post-trauma stress support (see Figure 4).
including anxiety, stress, depression and
carers to assess the progress of a child or
dissociation, anger and sexual concerns.
young person on a five-point scale on each of
This information is particularly important,
the eight Pillars of Parenting. As an example,
especially since the ‘emotional warmth’
approach is designed to reduce the level of
development on Pillar 4 (emotional compe-
developmental trauma and to promote adap-
well as measuring pathological aspects of
experienced applied psychology consultants
children’s homes before the final version of
the five point scales for each of the eight
information on the strength characteristics
pillars was finally completed. These carer
which are associated with more successful
ratings can then be plotted on the cobweb
personal and social development, especially
diagram which allows progress to be meas-
sense of mastery, sense of relatedness and
ured and noted over time. Different colours
can be used to provide a visual display of
improvements or deterioration over a longer
discuss these findings and their implications
residential or foster carers’ group consulta-
baseline measurements for ‘Renae’ show
tion session and is able to keep an ongoing
that she is rated at Level 1 (the lowest level of
development) in all the pillars, apart from
different factors being measured. Eventually,
emotional competence where she is rated at
it is hoped that the results from a larger
level 2. Three months later, ‘Renae’ has
analysed and published, not only to evaluate
the results from the ‘emotional warmth’
resilience. In the case of emotional compe-
approach, but also to provide much-needed
Educational & Child Psychology Vol. 28 No. 3R.J. (Seán) Cameron & Colin MaginnFigure 4: The cobweb record chart of a child’s progress and development over a three-month period. Box 2: The criteria used to evaluate progress and development on Pillar 4 (emotional competence). The emotional competence hierarchy Level 5: Child is able to understand and accept own feelings and the feelings of others and to respond appropriately to both. Level 4: Child can understand, control and manage a range of own emotions. Level 3: Child has knowledge of a range of emotions and is beginning to match appropriate emotions to context. Level 2: Child too often misinterprets the emotions of others as well as own emotional responses. Level 1: Child is unable to understand or control own emotions or has inexplicable changes of mood or blames others for own moods. Educational & Child Psychology Vol. 28 No. 3Living psychology: The ‘emotional warmth’ dimension of professional childcare
A similar five-point cobweb scale is used
of contemporary society. According to Fraser
to obtain essential information on a child’s
recognition that as well as competence in
professional practice, an additional dynamic
identify emotional progress, failure to make
for professional development has emerged –
progress or regression. It has been noted by
capability – the latter being a characteristic
one of the referees of this paper that the
progress of a young person on the parenting
constant change. It can be argued that the
pillars is likely to be reflected on measures of
emotional warmth approach to professional
that young person’s journey towards adap-
model. Such parallel links are most likely to
● It focuses on the psychological needs of
be seen with Pillar 1 (care and protection)
ment) and 6 (resilience) and the Integration
● There is a rationale, based in applied
phase and Pillars 2 (close relationships), 3
(self-perception), 7 (a sense of belonging)
and 8 (personal and social responsibility)
emotional development and theutilisation of the child’s signature or
Some reflections for applied psychologists
● The ‘good practice’ menu for the Pillars
For children or young people who have not
received adequate parenting and upbringing
Strengths components are ‘owned’ by the
violence, abuse and rejection, their progress
direct contact care staff: the role of the
often be a long, slow process which needs to
professional childcare. Achieving a trans-
knowledge and practice base and the prob-
requires clinical, educational or develop-
mental psychology practitioners to utilise
sophisticated consultation processes and an
in-depth knowledge of the discipline, so that
they can provide carers with a deeper under-
standing of problematic situations, offer
Based on findings from their survey of prac-
research-based, creative and effective ways of
tices and issues relating to children in care in
five local authority educational psychology
proactive approaches to minimise the occur-
Norwich et al. (2010) drew some practical
conclusions, including the need to develop
specialist roles for educational psychologists
uing, self-critical and reflective stance that
in supporting staff working with children in
examines applied psychology practice within
the context of the complexities and changes
Educational & Child Psychology Vol. 28 No. 3R.J. (Seán) Cameron & Colin MaginnAcknowledgement
tional psychology services need to clarify the
The authors would like to acknowledge with
distinctiveness of the kinds of contributions
thanks the creative contributions which the
senior management and care staff at Ingle-
services, while welcoming opportunities to
side Children’s Home, Sanderstead, Surrey
develop joint work with other services and
made to the early development of the ‘Pillars
professionals’ (p.388). The role of the
of Parenting’ component of the childcare
applied psychologist (clinical, educational or
developmental) which is outlined in thispaper highlights such a distinctive contribu-
Address for correspondence
tion, since it not only relies on the consulta-
Dr R.J. (Sean) Cameron
tion skills of an applied psychologist, but it
paper is that emotionally warm caring can
not only enhance the well-being of children
and young people in care but can also lead
to vastly improved life opportunities (seeLinley & Joseph, 2002). The emotionalwarmth approach to professional childcareprovides carers with the skills, knowledgeand support needed to meet the complexpsychological needs of these children andyoung people. It also offers applied psychol-ogists the personal and professional satisfac-tion of using psychology as a powerful forcefor positive change in the lives of childrenwho have been rejected, neglected andabused. Educational & Child Psychology Vol. 28 No. 3Living psychology: The ‘emotional warmth’ dimension of professional childcareReferences Baumeister, R. (2005). Rejected and alone.
Dreikurs, R., Grimwald, R.R. & Pepper, F.C. (1982). The Psychologist, 18(12), 732–735. Maintaining sanity in the classroom: Classroom
Bowlby, J. (1969). Attachment and loss. Vol. 1: Attach-management techniques. New York: Harper & Row.
Emler, N. (2001). Self-esteem: The causes and costs of low
Briere, J. (1996). Trauma Symptom Checklist for Childrenself-worth. York: York Publishing Services (for the
(TSCC): Professional Manual. Odessa, FL: Psycho-
Fraser, S. & Greenhalgh, T. (2001). Coping with
Burnett, P. (1999). The relationship between signifi-
complexity: Educating for capability. British
cant others’ positive and negative statements,
Medical Journal, 323, 799–803.
self-talk and self-esteem. Child Study Journal, 29,
Guishard-Pine, J., McCall, S. & Hamilton, L. (2007). Understanding looked after children: An introduction
Cairns, K. (2002). Attachment, trauma and resilience.to psychology for foster care. London: Jessica
London: British Association for Adoption and
House of Commons (2009). Children, Schools and
Cameron, R.J. & Maginn, C. (2005). What would a
Family Committee, 3rd report: Looked after children.
good parent do? Children Now, September, 22–23.
Cameron, R.J. & Maginn, C. (2008). Professional
Jackson, S. & Martin, P.Y. (1998). Surviving the care
childcare: The authentic warmth dimension.
system: Education and resilience. Journal ofBritish Journal of Social Work, 38, 1151–1172.
Cameron, R.J. & Maginn, C. (2009). Positive outcomes
Jackson, S. & McParlin, P. (2006) The education of
for children in care. London: Sage.
children in care. The Psychologist, 21(2), 90–93.
Carpendale, J. & Lewis, C. (2006). How children
Kennedy, H. Landor, M. & Todd, L. (2010a). Videodevelop social understanding. Oxford: Blackwell. Interactive Guidance: A relationship-based interven-
Crittenden, P.M. & Dallos, R. (2009). All in the
tion to promote attunement, empathy and well-being as
family: Integrating attachment and family
a method to promote secure attachment. London:
systems theories. Clinical Child Psychology andPsychiatry, 14(3), 389–409.
Kennedy, H., Landor, M. & Todd, L. (2010b) Video
Dent, H.R. & Golding, K.S. (2006). Engaging the
Interactive Guidance as a method to promote
network: Consultation for looked after and
secure attachment. Educational & Child
adopted children. In K.S. Golding, H.R. Dent,
R. Nissim & L. Stott (Eds.), Thinking psycho-
Lieberman, M.D. & Eisenberger, N.I. (2009). Pains
logically about children who are looked after and
and pleasures of social life. Science, 323, 890–891. adopted (pp.164–194). Chichester: Wiley.
Lewis, R. & Frydenberg, E. (2002). Concomitants of
Dent, H.R. & Cameron, R.J. (2003). Developing
failure to cope: What should we teach adoles-
resilience in children who are in public care: The
cents about coping? British Journal of Educational
educational psychology perspective. EducationalPsychology in Practice, 19(1), 1–19.
Linley, A. (2010). From Average to A+: Realising strengths
Department for Education (2010). Outcomes forin yourself and others. Coventry: Centre for
children looked after by local authorities in England asat 31 March 2010. SFR 38-2010. London: Author.
Linley, A. & Joseph, S. (2002). Post-traumatic growth.
Department for Education and Skills (2004). EveryCounselling and Psychology, 1(1), 14–17. child matters: Change for children. London: DfES.
Maslow, A.H. (1971). The farther reaches of human
Department for Education and Skills (2006). Carematters: Transforming the lives of children and young
Moore, J. (2005). Recognising and questioning the
people in care. Norwich: HMSO.
epistemological basis of educational psychology.
DeWall, C.N. & Baumeister, R.F. (2006). Alone but
Educational Psychology in Practice, 21(2), 103–116.
feeling no pain: Effects of social exclusion on
National Institute for Health and Clinical Excel-
physical pain tolerance and pain threshold, affec-
lence/Social Care Institute for Excellence
tive forecasting, and interpersonal empathy.
(2010). Promoting the quality of life of looked afterJournal of Personality and Social Psychology, 91(1),
children and young people. London: NICE.
Newman, T. & Blackburn, S. (2002). Transition in the
DeWall, C.N., MacDonald, G., Webster, G.D., Masten,
lives of children and young people: Resilience factors.
C.L., Baumeister, R.F., Powell, C., Combs, D. et al.
Edinburgh: Scottish Executive Education Depart-
(2010). Acetaminophen reduces social pain:
Behavioural and neural evidence. PsychologicalScience, 21(7), 931–937. Educational & Child Psychology Vol. 28 No. 3R.J. (Seán) Cameron & Colin Maginn
Nissim, R. (2006). More than walls: The context of
Rohner, R.P., Khaleque, A. & Couronoyer, D.E.
residential care. In K.S. Golding, H.R. Dent,
(2005). Parental Acceptance-Rejection: Theory,
R. Nissim & L. Stott (Eds.), Thinking psycho-
methods, cross-cultural evidence and implica-
logically about children who are looked after and
tions. Ethos, 33(3), 299–334. adopted (pp.255–278). Chichester: Wiley.
Rose, J. (2010). How nurture protects children: Nurture
Norwich, B., Richards, A. & Nash, T. (2010). Educa-
and narrative in work with children, young people and
tional psychologists and children in care: Prac-
their families. Skelmersdale, West Lancashire:
tices and issues. Educational Psychology in Practice,
Saarni, C, (1999). The development of emotional compe-
Perry, B. (2008). The boy who was raised as a dog, andtence. New York: Guilford Press. other stories from a child psychiatrist’s notebook: What
Seligman, M.E.P. (2002). Authentic happiness: Using thetraumatised children can teach us about loss, love andnew positive psychology to realise your potential for deepfulfilment. London: Nicholas Brealey.
Prince-Embury, S. (2006). Resiliency Scales for Children
Sheridan, S.M., Welch, M. & Orme, S.F. (1996).
and Adolescents. Oxford: Pearson Assessment.
Is consultation effective? A review of outcome
Qualifications and Curriculum Authority (2006).
research. Remedial and Special Education, 17(6),
The National Qualifications Framework. London:
Social Exclusion Unit (2002). Reducing reoffending by
Rohner, R.P. (1986). The warmth dimension: Founda-tions of Parental Acceptance-Rejection Theory.
Ziegenhain, U. (2004). The contribution of attach-
ment theory to early and preventive intervention
Rohner, R.P. (2004). The parental ‘Acceptance-
and to professional training. Educational and
Rejection Syndrome’. American Psychologist,Child Psychology, 21(1), 46–58.
Zimmerman, B.J. (1998). Academic studying and the
Rohner, R.P., Khaleque, A. & Couronoyer, D.E.
development of personal skill: A ‘self-regulatory
(2004). Parental Acceptance-Rejection: Theory,
perspective. Educational Psychologist, 33(2/3),
methods and implications. Downloadable from
Educational & Child Psychology Vol. 28 No. 3
6 december 2007 De Codecommissie KOAG/KAG (Kamer II) heeft het navolgende overwogen en beslist naar aanleiding van de klacht in kort geding (KK07.003) op de voet van artikel 3.2, laatste volzin, juncto artikel 6 van het Reglement voor de Codecommissie KOAG/KAG (hierna: het Reglement) van: Keuringsraad KOAG/KAG GlaxoSmithKline B.V. Het verloop van de procedure in kort geding 1.1 De C
F O R M A T O E U R O P E O P E R I L C U R R I C U L U M V I T A E INFORMAZIONI PERSONALI COGNOME e NOME Data di nascita Qualifica Incarico attuale Numero telefonico Numero fax Email istituzionale TITOLI DI STUDIO E PROFESSIONALI Titoli di studio Laurea Medicina Chirurgia Università degli Studi di Trieste (1980) Altri titoli di studio e/o Spec
 Living psychology: The ‘emotional warmth’ dimension of professional childcare
tics, like those released for England and
client group. Exemplars here would include
early intervention, child-focused initiatives
like school-based nurture groups designed
GCSEs at Key Stage 4 it has not been possible
2010), parent and teacher activities to build
to attribute this improvement to any partic-
up the resilience of these children (Dent &
ular intervention, since similar gains have
occurred in the general school population.
Living psychology: The ‘emotional warmth’ dimension of professional childcare
tics, like those released for England and
client group. Exemplars here would include
early intervention, child-focused initiatives
like school-based nurture groups designed
GCSEs at Key Stage 4 it has not been possible
2010), parent and teacher activities to build
to attribute this improvement to any partic-
up the resilience of these children (Dent &
ular intervention, since similar gains have
occurred in the general school population.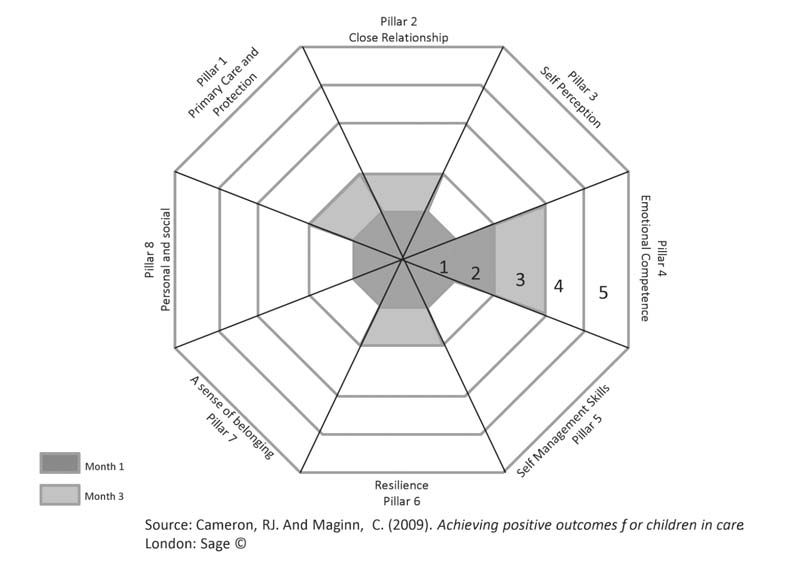 R.J. (Seán) Cameron & Colin Maginn
Figure 4: The cobweb record chart of a child’s progress and development over a
R.J. (Seán) Cameron & Colin Maginn
Figure 4: The cobweb record chart of a child’s progress and development over a