Ordered, immediately called back and the same day delivered the order.Very pleased with the work. Thank you for prompt and accurate work https://africarx.co.za/ great prices, delivered on the day of the order. Pleasant managers consult by phone.
My onn
Invited presentations of the latest cancer research
www.ajho.com
These arTicles are available from The January 2010 issue of aJho:
Jonathan B. Strauss; Monica Morrow; Balazs Halmos and Joshua R. Sonett William Small, Jr.
Is there a role for perioperative therapy in locally advanced
Predicting involvement of 4 or more lymph nodes: Does it
esophageal cancer? Case closed, time to move on
Rohini K. Hernandez; Henrik T. Sørensen; Hoshang Farhad; Maria-Victoria Orcurto; Lars Pedersen; Jacob Jacobsen; Michael Montemurro; Serge Leyvraz; John O. Timothy L. Lash Prior
Tamoxifen treatment and the risk of deep venous
Metabolic imaging with 18F-FDG-PET in patients with
imatinib-resistant gastrointestinal stromal tumor
Hillard M. Lazarus and Nathan A. Berger Farhana Sharmeen and David M. Jackman
Treating chronic lymphocytic leukemia in the elderly—
Bevacizumab in non-small cell lung cancer
Kandace P. McGuire; Alfredo A. Santillan; Krishnansu S. Tewari Paramjeet Kaur; Tammi Meade; Jateen Parbhoo;
A critical need for reappraisal of therapeutic options for women
Morgan Mathias; Corinne Shamehdi;
with metastatic and recurrent cervical carcinoma: Commentary
Michelle Davis; Daniel Ramos; Charles E. Cox
on Gynecologic Oncology Group Protocol 204
Mastectomy vs breast conservation: Mastectomy on the rise
Breast Cancer ask The exPerT Larissa Nekhlyudov and Laurel A. Habel Women with ductal carcinoma in situ are not getting follow- up mammograms after breast-conserving surgery PERSPECTIVE
Quality of Life after Dose-Escalated Radiation Therapy for Prostate Cancer
Mark W. McDonald, MD, and Peter A.S. Johnstone, MD, FACRDepartment of Radiation Oncology, Indiana University,Indianapolis, Indiana, and Midwest ProtonRadiotherapy Institute, Bloomington, Indiana
Men with localized prostate cancer have a variety of treatment choices and can expect similar disease con-trol and survival outcomes from radical prostatectomy, external beam radiation therapy, and interstitialprostate brachytherapy.1,2 In addition to cancer control, treatment-related side effects and quality-of-life end-points are influential in most men when deciding between therapeutic modalities.3 In the past decade,
results of several randomized trials have shown a statistically signifi-
between men treated on the conventional and high-dose arms. Patients
cant improvement in biochemical disease control for patients treated
treated on the conventional dose arm were more often concerned about
with high-dose external beam radiation therapy (74–79.2 Gy) com-
their cancer control and more often expressed regret about their treatment
pared to conventional dose radiation therapy (64–70.2 Gy).4–8 These
decision. Unfortunately, patient-reported data were not collected at baseline
trials also have generally observed an increased but clinically accept-
or at any other time point, which hinders interpretation of the data.
able rate of acute gastrointestinal (GI) toxicity with high-dose radia-
Prospective patient-reported quality-of-life assessment was conducted in the
tion. Not surprisingly given the study sizes and still limited follow-
Dutch CKTO 69-10 randomized prostate dose escalation trial,5 and prelim-
up, none have yet shown an improvement in cancer-specific or over-
inary results at 3 years of follow-up have similarly indicated no difference in
all survival. Notably lacking until recently have been patient-report-
quality-of-life outcomes between patients randomized to conventional (68
ed toxicity and quality-of-life outcomes.
Since quality-of-life measures appear to worsen with longer follow-up
Talcott et al suggest that their results may validate the ability of proton
time,9,10 to properly gauge the therapeutic benefit of dose escalation, it is
therapy to deliver a higher and more efficacious dose to the prostate with-
important to assess for increased toxicity in the high-dose radiation arms as
out increasing long-term toxicity. Although a significant portion of the radi-
these trial data continue to mature. The recent report by Talcott et al11 pro-
ation dose was delivered with x-rays in PROG 9509, and there was no arm
vides long-term patient-reported outcomes from a randomized prostate
treated with dose-escalated x-ray radiation alone for comparison, these
dose-escalation trial. All living patients enrolled in the Proton Radiation
results provide valuable long-term patient-reported toxicity outcomes after
Oncology Group (PROG) 9509 randomized controlled trial of radiation
dose-escalated proton therapy for prostate cancer. Proton therapy is a form
dose escalation in prostate cancer were contacted and asked to answer a
of conformal external beam radiation therapy that uses accelerated protons
questionnaire using validated assessments of urinary and bowel complica-
instead of high-energy x-rays. Unlike x-rays, protons can be modulated to
tions, sexual function, and disease-focused quality of life. PROG 9509 ran-
have a defined stopping point in tissue where they deposit most of their
domized 393 patients with clinically localized stage T1b to T2b prostate
energy.14 This peak dose deposition at the termination of the proton path is
cancer with prostate-specific antigen (PSA) less than 15 ng/mL treated with
known as the Bragg peak and allows treatment with protons to effectively
external beam radiation therapy alone to a total dose of either 70.2 Gy or
stop dose in tissue at a given point and eliminate dose to tissues beyond that
79.2 Gy.4 All patients received 50.4 Gy with conformal x-ray therapy and
point. Protons also have a sharp beam penumbra, meaning that on the lat-
either 19.8 Gy or 28.8 Gy equivalent with proton therapy. At a median fol-
eral edges of the beam, the dose drops from full intensity to zero intensity
low-up time of nearly 9 years, patients treated on the high-dose radiation
arm were significantly more likely to have local control and biochemical dis-
With its unique physical properties, proton therapy for prostate cancer
ease control with a hazard ratio for local failure of 0.57.12 Physician assess-
can be delivered through two lateral fields, eliminating the entrance and exit
ment found no difference in acute or late genitourinary (GU) toxicity nor
dose to normal tissues outside of these fields that would otherwise be tra-
in late GI toxicity, although acute GI toxicity of grade 2 or higher was seen
versed with multi-field x-ray treatment. Formal comparisons of proton ther-
in 64% of patients in the high-dose arm compared to 45% in the conven-
apy and intensity-modulated (x-ray) radiation therapy (IMRT) for prostate
cancer have quantified the reductions in radiation dose to normal tissues,
Eighty-three percent of the patients remaining alive (n = 280) respond-
such as the bladder and rectum, achieved with proton therapy.16,17
ed to the questionnaire at a median time of 9.4 years after treatment. Results
Given the correlation of dose to normal structures and resultant tox-
showed no difference in patient-reported GU, GI, or sexual function
icity, quality radiation treatment planning and delivery are expected to
The authors were invited to provide this commentary on the research findings reported in Talcott JA, Rossi C,Shipley WU, et al. Patient-reported long-term outcomes after conventional and high-dose combined proton andphoton radiation for early prostate cancer. JAMA. 2010;303:1046–1053.
88 • AJHO MAY 2010;9(3) • WWW.AJHO.COM
Perspective / Quality of life after radiation therapy for prostate cancer
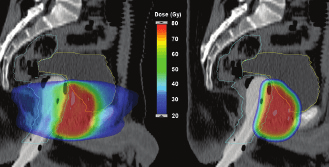
Sagittal views of a 7-field IMRT photon planfor prostate cancer (left) and a proton plan(right), prescribed to 79.2 Gy. The bladder(yel ow) and rectum (blue) are outlined. Arectal bal oon fil ed with radiopaque fluid isused to increase rectal sparing and for pro-static immobilization. Both modalitiesclosely conform the high-dose volume (redarea) to the target, while the proton planreduces the volume of normal tissuesreceiving low and moderate doses of radia-tion (blue and green, here 20 Gy to 50 Gy). Images courtesy of Chee-Wai Cheng, PhD,Midwest Proton Radiotherapy Institute.
translate into lower rates of toxicity and fewer adverse effects on quality
the MRC RT01 randomised controlled trial. Lancet Oncol. 2007;8:475–487.
of life. Indeed, subsequent correlation of the PROG 9509 patient-report-
9. Johnstone PA, Gray C, Powell CR. Quality of life in T1-3N0 prostate cancer
ed outcomes with radiation dosimetry found a significant association
patients treated with radiation therapy with minimum 10-year follow-up. Int J Radiat
between increased dose to the anterior rectal wall and subsequent GI dys-
Oncol Biol Phys. 2000;46:833–838.
function, independent of the prescribed dose to the prostate.18
10. Gardner BG, Zietman AL, Shipley WU, Skowronski UE, McManus P. Late nor-
These quality-of-life data from the Dutch CKTO 69-10 and PROG
mal tissue sequelae in the second decade after high dose radiation therapy with com-
9509 randomized trials, at short- and long-term follow-up, respectively,
bined photons and conformal protons for locally advanced prostate cancer. J Urol.
provide the first confirmation that the improved disease control
obtained with dose-escalated radiation therapy can be achieved without
11. Talcott JA, Rossi C, Shipley WU, et al. Patient-reported long-term outcomes after
increased patient-reported late toxicity. Corollary data confirm that
conventional and high-dose combined proton and photon radiation for early prostate
quality radiation planning matters, and techniques and interventions
cancer. JAMA. 2010;303:1046–1053.
that reduce dose to normal tissue sparing can translate into improved
12. Zietman AL, Bae K, Slater JD, et al. Randomized trial comparing conventional-
dose with high-dose conformal radiation therapy in early-stage adenocarcinoma of
the prostate: long-term results from proton radiation oncology group/american col-
lege of radiology 95-09. J Clin Oncol. 2010;28:1106–1111.
1. Kupelian PA, Potters L, Khuntia D, et al. Radical prostatectomy, external beam
13. Al-Mamgani A, van Putten WL, van der Wielen GJ, Levendag PC, Incrocci L.
radiotherapy <72 Gy, external beam radiotherapy > or =72 Gy, permanent seed
Dose Escalation and Quality of Life in Patients with Localized Prostate Cancer
implantation, or combined seeds/external beam radiotherapy for stage T1-T2
Treated with Radiotherapy: Long-Term Results of the Dutch Randomized Dose-
prostate cancer. Int J Radiat Oncol Biol Phys. 2004;58:25–33.
Escalation Trial (CKTO 96-10 Trial). Int J Radiat Oncol Biol Phys. 2010 Apr 24.
2. Wilt TJ, MacDonald R, Rutks I, Shamliyan TA, Taylor BC, Kane RL. Systematic
review: comparative effectiveness and harms of treatments for clinically localized
14. Wilson RR. Radiological use of fast protons. Radiology. 1946;47:487–491.
prostate cancer. Ann Intern Med. 2008;148:435–448.
15. Urie MM, Sisterson JM, Koehler AM, Goitein M, Zoesman J. Proton beam
3. Zeliadt SB, Ramsey SD, Penson DF, et al. Why do men choose one treatment over
penumbra: effects of separation between patient and beam modifying devices. Med
another?: a review of patient decision making for localized prostate cancer. Cancer.
16. Trofimov A, Nguyen PL, Coen JJ, et al. Radiotherapy treatment of early-stage
4. Zietman AL, DeSilvio ML, Slater JD, et al. Comparison of conventional-dose vs
prostate cancer with IMRT and protons: a treatment planning comparison. Int J
high-dose conformal radiation therapy in clinically localized adenocarcinoma of the
Radiat Oncol Biol Phys. 2007;69:444–453.
prostate: a randomized controlled trial. JAMA. 2005;294:1233–1239.
17. Chera BS, Vargas C, Morris CG, et al. Dosimetric study of pelvic proton radio-
5. Peeters ST, Heemsbergen WD, Koper PC, et al. Dose-response in radiotherapy for
therapy for high-risk prostate cancer. Int J Radiat Oncol Biol Phys.
localized prostate cancer: results of the Dutch multicenter randomized phase III trial
comparing 68 Gy of radiotherapy with 78 Gy. J Clin Oncol. 2006;24:1990–1996.
18. Nguyen PL, Chen RC, Hoffman KE, et al. Rectal Dose-Volume Histogram
6. Kuban DA, Tucker SL, Dong L, et al. Long-term results of the M.D. Anderson
Parameters Are Associated with Long-Term Patient-Reported Gastrointestinal
randomized dose-escalation trial for prostate cancer. Int J Radiat Oncol Biol Phys.
Quality of Life After Conventional and High-Dose Radiation for Prostate Cancer: A
Subgroup Analysis of a Randomized Trial. Int J Radiat Oncol Biol Phys. 2010 Mar 5.
7. Shipley WU, Verhey LJ, Munzenrider JE, et al. Advanced prostate cancer: the
results of a randomized comparative trial of high dose irradiation boosting with con-
formal protons compared with conventional dose irradiation using photons alone. IntDisclosures: The authors disclose no relevant conflicts of interest. J Radiat Oncol Biol Phys. 1995;32:3–12. Correspondence address: Mark W. McDonald, MD, 535 Barnhill Dr, RT 041,
8. Dearnaley DP, Sydes MR, Graham JD, et al; for the RT01 collaborators. Escalated-
Indianapolis, IN 46202; e-mail: mwmcdona@iupui.edu.
dose versus standard-dose conformal radiotherapy in prostate cancer: first results from
WWW.AJHO.COM • AJHO MAY 2010;9(3) • 89
HARTRESEARCH Views On Alcoholism & Treatment Alan Rivlin Senior Vice President Peter D. Hart Research Associates September 29, 2005 Research Methods - Overview Internet surveys were conducted among the following populations:1,000 adults age 20+; margin of error = ±3.1 percentage points– 300 physicians; margin of error = ±5.7 percentage pointsThe Internet
Testing the Difference Between Proportions (p1 - p2) BACKGROUND VIAGRA is a prescription medicine that is used to treat male impotence. To protect American consumers, the U. S. Food and Drug Administration requires drug manufacturers to conduct clinical trials to demonstrate a drug’s safety and effectiveness. In applying for FDA approval for VIAGRA, Pfizer Pharmaceuticals, Inc. submitted
 Perspective / Quality of life after radiation therapy for prostate cancer
Sagittal views of a 7-field IMRT photon planfor prostate cancer (left) and a proton plan(right), prescribed to 79.2 Gy. The bladder(yel ow) and rectum (blue) are outlined. Arectal bal oon fil ed with radiopaque fluid isused to increase rectal sparing and for pro-static immobilization. Both modalitiesclosely conform the high-dose volume (redarea) to the target, while the proton planreduces the volume of normal tissuesreceiving low and moderate doses of radia-tion (blue and green, here 20 Gy to 50 Gy).
Perspective / Quality of life after radiation therapy for prostate cancer
Sagittal views of a 7-field IMRT photon planfor prostate cancer (left) and a proton plan(right), prescribed to 79.2 Gy. The bladder(yel ow) and rectum (blue) are outlined. Arectal bal oon fil ed with radiopaque fluid isused to increase rectal sparing and for pro-static immobilization. Both modalitiesclosely conform the high-dose volume (redarea) to the target, while the proton planreduces the volume of normal tissuesreceiving low and moderate doses of radia-tion (blue and green, here 20 Gy to 50 Gy).